
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Disassembly of hip prosthesis is rare but challenging clinical scenario which should be managed by being very watchful and gentle while attempting closed reduction of dislocated hip prosthesis and should have high index of suspicion for possible disassembly of prosthesis via “Bottleopener effect”.
Case Report | Volume 10 | Issue 9 | JOCR December 2020 | Page 90-93 | Mukesh Kumar Saini, Neelam Ramana Reddy, Pera Jayavardhan Reddy. DOI: 10.13107/jocr.2020.v10.i09.1916
Authors: Mukesh Kumar Saini1, Neelam Ramana Reddy1, Pera Jayavardhan Reddy1
[1]Department of Orthopaedics, (Arthroplasty Division), Star Hospitals Hyderabad, Telangana, India.
Address of Correspondence:
Dr. Mukesh Kumar Saini,
Department of Orthopaedics (Arthroplasty Division) Star Hospitals, B Block Road No.10 Banjara Hills, Hyderabad, Telangana, India.
E-mail: sainimk.saini8@gmail.com
Abstract
Introduction: Bipolar hemiarthroplasty has been reliable and successful treatment for geriatric patients following neck of femur fractures. Dissociation/disassembly of bipolar prosthesis is a rare complication in which separation of outer head from inner head leads to failure of prosthesis and needs revision surgery. The disassembly though commonly seen after years of primary surgery as a result of polyethylene wear leading to fixed varus position of outer head but it can happen in an acute setting anytime in immediate or late post-operative period following posterior dislocation with closed reduction attempt. We describe a rare case of disassembly of monoblock (non-modular) bipolar prosthesis following attempt of closed reduction for posterior dislocation of the prosthesis.
Case Report: The patient was a 70-year-old male with 3 weeks prior bipolar hemiarthroplasty of hip joint, presented with posterior dislocation. While manipulation during closed reduction maneuvers, the outer head got locked behind acetabulum and component dissociation happened through bottle opener phenomena. The patient managed with revision surgery in the form of bipolar extraction and revision with total hip joint prosthesis.
Conclusion: Disassembly of bipolar prosthesis is a rare and unforeseen complication which obviates for revision surgery. A modular bipolar prosthesis can be reassembled or can be managed with shell, liner, and head exchange with retention of femoral stem but it is impossible to reassemble a non-modular bipolar due to its characteristic locking mechanism. It is vital to look for proper orientation and stability of components, integrity of abductor mechanism and short external rotators, and restoration of horizontal and vertical offsets during revision.
Keywords: Bipolar disassembly, hip prosthesis dissociation, bottle opener effect.
Introduction
Hemiarthroplasty of hip joint following subcapital neck femur fracture in elderly population has been reliable and successful treatment. Over the time, the bipolar hip prosthesis replaced earlier used unipolar prosthesis due to added advantage of modularity and motion at two different articulations [1]. Nevertheless, the prosthesis too comes with certain disadvantages like wear of polyethylene liner and rare but possible chances of dissociation of components of bipolar prosthesis during primary traumatic event or during manipulative reduction maneuvers following dislocation. The iatrogenic dissociation, which is known to happen with typical “bottle opener effect,” has been reported only in a few reports described with modular bipolar prosthesis [2, 3, 4, 5].
We hereby report on a patient who had iatrogenic dissociation of components following attempted closed reduction for posterior dislocation of bipolar prosthesis. We discuss the characteristic mechanism responsible for the catastrophic complication, anticipated problems, and important considerations during revision surgery and post-operative course of treatment.
Case Report
A 70-year-old male presented to the emergency department with complaints of sudden onset of severe pain in his left hip while getting up from bed. He was unable to bear weight on his affected lower limb since the episode. The patient had undergone left-sided cemented bipolar hemiarthroplasty for subcapital neck femur fracture 3 weeks ago (Fig. 1). On examination, there was well-healed surgical scar over posterolateral aspect of hip showing no sign of infection. His left lower limb was shortened, adducted, and internal rotated with diffuse severe tenderness over anterior and posterior aspect of his left hip joint without any neurovascular deficit. Pelvis and hip radiographs were ordered in suspicion of dislocation of prosthetic joint. The radiographs reveal posterior dislocation of non-modular bipolar prosthesis (Fig. 2). The patient was taken for urgent closed reduction under general anesthesia. During closed reduction with Allis maneuver under image intensifier, sudden clunk was felt and limb length and alignment improved, though not to the full. Image intensifier images revealed separation of outer head of the bipolar prosthesis from inner head stem assembly. The inner head slipped and got reduced in acetabulum while the separated outer head of prosthesis was floating outside the acetabulum (Fig. 3). The procedure abandoned and the patient and his attendants were counseled for revision surgery in the form of hemiarthroplasty or total hip joint replacement in elective setting.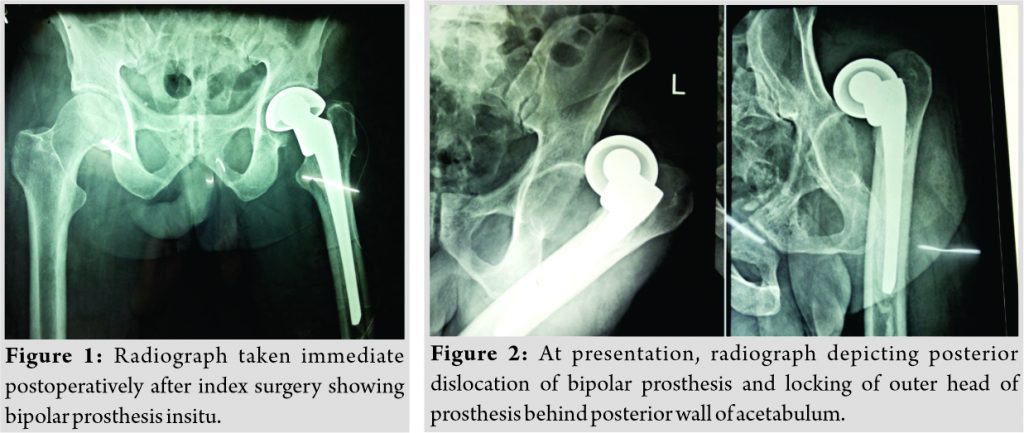
The hip joint was approached from posterolateral approach utilizing the previous surgical scar. The short external rotators and capsule were found to be torn. The prosthesis (INOR Inc., Mumbai, India) outer headliner assembly, which was floating posterior to acetabulum, retrieved and examined. There was no sign of erosion of polyethylene liner or damage to locking mechanism at outer head (Fig. 4). The inner head found to be intact but the stem found to be loose as there was debonding of cement at bone-cement interface. The anteversion of stem found to be around 10° though there was no fracture around acetabulum or proximal femur.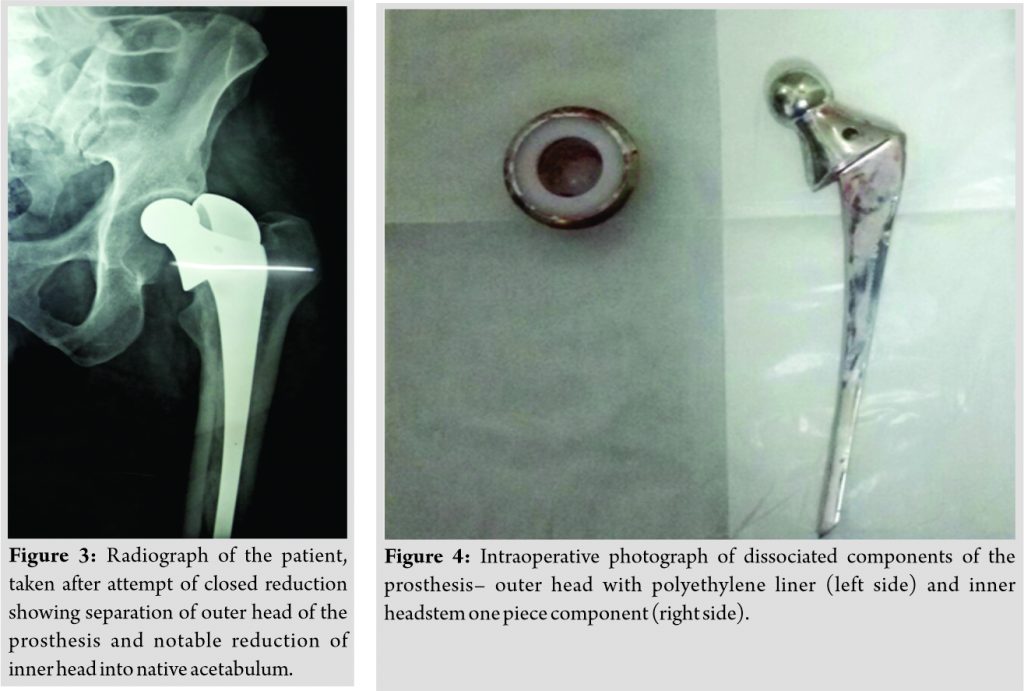
We noticed that there were focal cartilage loss and inferior osteophyte in acetabulum; hence, a decision of total hip joint arthroplasty was done. The bipolar stem was removed and total hip arthroplasty was done with cemented acetabular ZCA cup (Zimmer Inc., Warsaw IN, USA) and cemented femoral components with CPT stem (Zimmer Inc., Warsaw IN, USA).We used extended offset femoral stem to restore adequate tension in hip joint abductors and increased femoral anteversion to 15°and kept acetabular cup anteversion around 20°making combined anteversion angle around 35°. We repaired joint capsule and short external rotators meticulously for the prevention of recurrent dislocation. Post-operative radiographs were satisfactory (Fig. 5).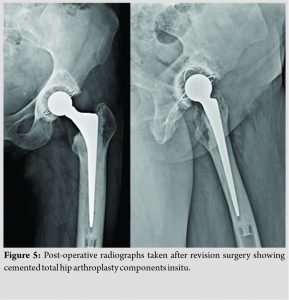
The patient was mobilized full weight-bearing on the 2ndpost-operative day and advised to use hip abduction brace at rest for 8 weeks post-surgery. The patient was followed up at 6 weeks, 3 months, at 6 months and 1 year post-surgery and had no complication in meantime.
Discussion
Hemiarthroplasty of hip joint has been standard of care for neck femur fracture in elderly patients due to its predictable pain relief, immediate function resumption, and lower needs for revision surgery. Short- to medium-term studies comparing unipolar prosthesis with bipolar showed no difference in terms of mortality and functional outcome though; the later ones lead to lesser revision rates as compared to the former. The bipolar prosthesis poses two bearing surfaces, one between outer head (OH) and acetabulum and another between inner head (IH) and polyethylene liner integrated with outer head. In monoblock (non-modular) bipolar prosthesis, the entire assembly is locked by locking mechanism at outer margin of polyethylene in liner OH composite which prevents its dissociation from rest of prosthesis, that is, inner head stem part.
Dislocation of prosthetic hip joint is still a major concern, incidences of which reported to be around 3–4% and in some series it’s been as high as 16%[5], [6]. Disassembly or dissociation of components of a bipolar prosthesis is a phenomenon in which there is separation of components of prosthesis commonly seen between outer head and inner hand of prosthesis. There are only few cases described in the literature on dissociation of monoblock bipolar components and most of them are result of failure of locking mechanism at outer head.
Star et al. first described iatrogenic dissociation of modular bipolar components following attempt of closed reduction necessitating subsequent surgery [7]. The patient was a 38-year-old female who had a fall following 9 months of index surgery and subsequent posterior dislocation. The complication was managed by revision hemiarthroplasty using higher offset stem component.
Hasegawa et al. reported a series of seven cases of dissociation of bipolar prosthesis [8]. All dissociations occurred secondary to failure of locking mechanism of self-centering prosthesis. The mechanism of failure was attributed to fixed varus position of outer head, increased friction between acetabulum and outer head due to wear and osteophytes, severe abrasion at polyethylene rim due to neck impingement followed by deformity of locking ring. Revision surgeries in above cases were done with cementless total hip prosthesis.
In 2006, Georgiou et al. reviewed the available literature about bipolar disassembly and published a series of five different cases of component dissociation [2]. Two cases out of the five disassembled during closed reduction maneuver while two cases of dissociation happened due to failure of locking mechanism while in one case reduced acetabular coverage and mechanical failure of polyethylene was responsible for disassembly.
In our case, the first post-operative radiograph (Fig. 1) after index surgery showed shortening of the left lower limb and reduced offset which might be the reason for early dislocation. While attempting closed reduction, the outer head of bipolar prosthesis locked behind posterior acetabular wall while application of standard reduction maneuver with traction to the limb leads to separation of components of prosthesis. The above mechanism was described as “Bottle opener effect” in the previous studies [2, 3, 4].
Guo et al. classified the disassembly of bipolar prosthesis in the following types [9]:
Type I is also known as iatrogenic dissociation and it occurs following attempted closed reduction in a locked outer head of bipolar prosthesis behind acetabulum also known as bottle opener effect. These cases present typically after few weeks to months after index surgery.
Type II dissociation occurs in cases where polyethylene liner of prosthesis undergoes wear and fixed varus position of outer head of prosthesis leads to damage and subsequent failure of locking mechanism resulting into separation of components between polyethylene and inner head.
TypeIII also known as spontaneous type is a very rare and caused by failure of locking mechanism resulting into intra-acetabulardislocation. In this type, inner head dislocates posteriorly while outer head remains in position. This typically happens when the patient remains in leaning forward position.
Uruç et al. described five cases of early dissociation of bipolar process in 2017 [4]. Out of five, two cases were iatrogenic type,that is, following closed reduction attempt. The author attributed the disassembly for attempting closed reduction without using general anesthesia and no fluoroscopic control.
Recently, in a case series by Bian et al., the author described four cases of posterior dislocation of bipolar prosthesis [10]. While treating these patients with trial of traditional closed reduction maneuver, three hip prostheses got disassembled. While managing the fourth case, the author adopted a novel method of closed reduction by pushing the lower limb in axial direction proximally followed by internal rotation and then conventional traction maneuver. Thus, unlocking the prosthesis first and then traction described as “Push-turnover-pull” maneuver. The technique needs closed fluoroscopic control and has to be attempted under anesthesia only. This technique, though sounds promising, is yet to get tested widely in clinical circumstances before adopting it as standard practice for the prevention of disassembly during closed reduction of bipolar prosthesis.
Conclusion
Closed reduction following posterior dislocation of bipolar prosthesis (modular or monoblock) is technically challenging and one should keep in mind of possible disassembly of components during reduction maneuver. The procedure must be scrutinized under fluoroscopic control and performed under general anesthesia. If closed reduction fails, revision surgery in form of hemi or total joint arthroplasty should be warranted with emphasis on examination of retrieved components as well as acetabular cartilage, restoration of horizontal and vertical offset, restoration of proper anteversion of acetabular cup/femoral stem, repair of capsule, and short external rotators for the prevention of future dislocation.
Clinical Message
Disassembly of hip prosthesis is rare but challenging clinical scenario which should be managed to address the failure in primary construct. It is vital to understand and classify the problem according to the chronicity, mechanism of failure, implant status, bone, and soft tissue loss for proper management. One must be very watchful and gentle while attempting closed reduction of dislocated hip prosthesis and should have high index of suspicion for possible disassembly of prosthesis through “Bottle opener effect.”
References
1. Inngul C, Hedbeck CJ, Blomfeldt R, Lapidus G, Ponzer S, Enocson A. Unipolar hemiarthroplasty versus bipolar hemiarthroplasty in patients with displaced femoral neck fractures: A four-year follow-up of a randomised controlled trial. Int Orthop 2013;37:2457-64.
2. Georgiou G, Siapkara A, Dimitrakopoulou A, Provelengios S, Dounis E. Dissociation of bipolar hemiarthroplasty of the hip after dislocation. A report of five different cases and review of literature. Injury 2006;37:162-8.
3. Chang JJ, Pan RY, Lin LC. Dissociation of bipolar prostheses with hip subluxation: A case report and literature review. J Med Sci 2014;34:214-6.
4. Uruç V, Özden R, Duman İG, Kalacı A. Five cases of early dissociation between the bipolar hip endoprosthesis cup components; either spontaneously or during reduction maneuvers. Acta Orthop Traumatol Turc 2017;51:172-6.
5. Kim Y, Kim JK, Joo IH, Hwang KT, Kim YH. Risk factors associated with dislocation after bipolar hemiarthroplasty in elderly patients with femoral neck fracture. Hip Pelvis 2016;28:104-11.
6. Pajarinen J, Savolainen V, Tulikoura I, Lindahl J, Hirvensalo E. Factors predisposing to dislocation of the Thompson hemiarthroplasty: 22 dislocations in 338 patients. Acta Orthop Scand 2003;74:45-8.
7. Star MJ, Colwell CW Jr., Donaldson WF 3rd, Walker RH. Dissociation of modular hip arthroplasty components after dislocation. A report of three cases at differing dissociation levels. Clin Orthop Relat Res 1992;278:111-5.
8. Hasegawa M, Sudo A, Uchida A. Disassembly of bipolar cup with self-centering system: A report of seven cases. Clin Orthop Relat Res 2004;425:163-7.
9. Guo JJ, Yang H, Yang T, Tang T. Disassembly of cemented bipolar prothesis of the hip. Orthopedics 2008;31:813.
10. Bian YY, Wang LC, Xiao K, Jin J, Zhang BZ, Weng XS. Hip dislocation and femoral component disassembly after bipolar hemiarthroplasty: A report of four cases and introduction of new reduction maneuvers. Chin Med J (Engl) 2019;132:370-2.
 |
 |
 |
| Dr. Mukesh Kumar Saini | Dr. Neelam Ramana Reddy | Dr. Pera Jayavardhan Reddy |
| How to Cite This Article: Saini MK, Reddy NR, Reddy PJ. Disassembly of components of a monoblock bipolar hip prosthesis following dislocation: A case report and review on “Bottle Opener Effect”. Journal of Orthopaedic Case Reports 2020 December;10(9): 90-93. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


