
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Intramedullary tibial nails in high level athletes are a viable surgical treatment option for stress fractures.
Case Report | Volume 10 | Issue 9 | JOCR December 2020 | Page 114-117 | Devin W Collins, David P Antekeier. DOI: 10.13107/jocr.2020.v10.i09.1928
Authors: Devin W Collins[1], David P Antekeier[1]
[1]Department of Orthopaedics, Jack Hughston Memorial Hospital, The Hughston Clinic 4401 River Chase Drive, Phenix City, AL 36867, United States.
Address of Correspondence:
Dr. Devin W Collins,
D.O., Jack Hughston Memorial Hospital, The Hughston Clinic, 4401 River Chase Drive, Phenix City, AL 36867, United States.
E-mail: devinCollins71@gmail.com
Abstract
Introduction: Mid-diaphyseal anterior tibial stress fractures can be debilitating injuries. They have been described occurring in athletes due to repetitive lower extremity trauma. The purpose of our study was to highlight a case of an athlete sustaining a tibial stress fracture with multiple cortical defects.
Case Report: We present an 18-year-old collegiate bound athlete who sustained a tibial stress fracture with multiple cortical defects. The clinical decision, after failure of conservative treatment, was made to treat the patient with tibial intramedullary nailing. She was able to return to full unrestricted activities, including high-level sports participation. Our case report specifically describes a case of a high-level athlete with multiple anterior tibial linear cortical defects from a chronic stress fracture.
Conclusion: When conservative management for mid-diaphyseal anterior stress fractures fails, the utilization of prophylactic tibial nailing is a viable option. The decision for surgical intervention is dependent on many factors including patient’s activity level and characteristics, failure of conservative management, and radiographic evidence of non-healing stress fractures.
Keywords: Tibial, stress fractures, sports medicine, trauma, intramedullary nail..
Introduction
Mid-diaphyseal anterior tibial stress fractures are uncommon. Burrows first described anterior tibial stress fractures in 1956. Most often these occur in athletes due to repetitive lower extremity activities. Patients will typically present complaining of prolonged anterior leg pain. On physical examination, these patients will have diffuse tenderness along the anterior aspect of the tibia. Acutely, radiographs are not always diagnostic but chronically, they will demonstrate a thickened anterior cortex, narrowing of the medullary canal and a linear cortical fracture line sometimes referred to as the “dreaded black line” [1]. Cases describing the utilization of intramedullary nailing in anterior tibial stress fractures have previously been described [1, 2, 3, 4]. We review the clinical decision to employ prophylactic intramedullary tibial nailing in an athlete with chronic stress fractures recalcitrant to conservative treatment. Previous case reports have described single, linear anterior tibial stress fractures treated with intramedullary tibial nails. Here, we present a rare case of a collegiate high-level athlete with multiple tibial stress fractures treated with a reamed, locked intramedullary tibial nail and describe the clinical indications and outcome.
Case Report
An 18-year-old female presented for orthopedic evaluation on referral from her pediatrician due to increasing pain in her right leg. The patient was a high school volleyball player who most recently participated in a tournament 3 weeks prior. Following this tournament, she was unable to participate in further competition due to increasing pain where ice and ibuprofen had not helped during this time period. On further questioning, she described having pain in both her right and left legs for more than a year but currently her right was more problematic. Physical examination revealed that she was tender along the middle anterior border of her right lower leg. She remained motor, sensory, and vascular intact with a mild limp. Radiographs (Fig. 1) of the right leg demonstrated changes consistent with chronic stress fractures along the anterior mid-diaphyseal tibia. Thickening of the cortex was noted with narrowing of the medullary canal and at least six linear cortical defects of varying sizes were seen. An in-depth discussion of management options was discussed with the patient. On further investigation, it was discovered that the patient was on a scholarship track to a major Division I university. Since the patient had previously failed conservative management and the current severity of chronic stress fractures limiting her activities, prophylactic tibial nailing was determined to be the most viable option for the patient. Procedure performed was an antegrade remade statically locked intramedullary tibial nail.
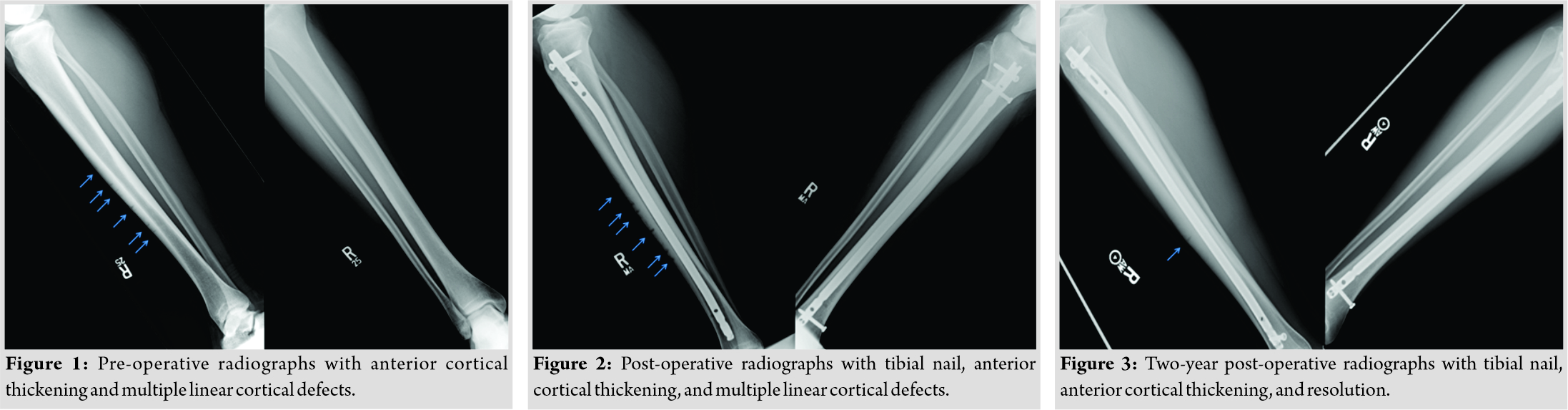 The patient was taken to the operative theater, placed supine, and draped in sterile fashion. A 4 cm incision was made over the proximal tibia with the tendon split in line with its’ fibers. An anterior guide wire was placed and confirmed with fluoroscopy in the lateral and anteroposterior views. A decompression hole was placed on the anteromedial aspect of the distal tibia. Following sequential reaming, a 10 mm by 375 mm tibial nail was placed. One distal locking screw was placed statically at this time with backslap technique performed. Following this, two proximal locking screws were placed. Radiographs confirmed placement of the nail and locking screws. She was placed into a CAM boot, made weight-bearing as tolerated with crutches. Post-operative radiographs were obtained demonstrating good placement of the intramedullary tibial nail. At the 2 weeks post-operative visit, she had weaned herself to the use of one crutch. Her pain was well controlled and she had no acute complaints. Sutures were removed at this time. Her gross motor and sensory examination remained intact. She was to continue with physical therapy working on range of motion, strength, and gait training. Six weeks postoperatively, she had progressed to full weight-bearing without assistive devices. On gait examination, she maintained a mild antalgic limp to her operative leg, but her motor examination and sensory examination remained intact. Repeat radiographs (Fig. 2) were obtained at this time demonstrating intact hardware. Prior cortical lines remained visible, more pronounced in the lateral radiograph. The patient was then lost to follow up secondary to moving out of the state. At 2 years after her surgery, the patient presented for follow-up. She reported having returned to full unrestricted high-level athletic activities without pain. She was able to perform at a collegiate level in volleyball. On physical examination, there was no pain throughout the lower leg and full muscle strength. Radiographs were obtained at this time (Fig. 3) demonstrating intact tibial intramedullary nail with resolution of all but one residual cortical defect as seen on the lateral radiograph.
The patient was taken to the operative theater, placed supine, and draped in sterile fashion. A 4 cm incision was made over the proximal tibia with the tendon split in line with its’ fibers. An anterior guide wire was placed and confirmed with fluoroscopy in the lateral and anteroposterior views. A decompression hole was placed on the anteromedial aspect of the distal tibia. Following sequential reaming, a 10 mm by 375 mm tibial nail was placed. One distal locking screw was placed statically at this time with backslap technique performed. Following this, two proximal locking screws were placed. Radiographs confirmed placement of the nail and locking screws. She was placed into a CAM boot, made weight-bearing as tolerated with crutches. Post-operative radiographs were obtained demonstrating good placement of the intramedullary tibial nail. At the 2 weeks post-operative visit, she had weaned herself to the use of one crutch. Her pain was well controlled and she had no acute complaints. Sutures were removed at this time. Her gross motor and sensory examination remained intact. She was to continue with physical therapy working on range of motion, strength, and gait training. Six weeks postoperatively, she had progressed to full weight-bearing without assistive devices. On gait examination, she maintained a mild antalgic limp to her operative leg, but her motor examination and sensory examination remained intact. Repeat radiographs (Fig. 2) were obtained at this time demonstrating intact hardware. Prior cortical lines remained visible, more pronounced in the lateral radiograph. The patient was then lost to follow up secondary to moving out of the state. At 2 years after her surgery, the patient presented for follow-up. She reported having returned to full unrestricted high-level athletic activities without pain. She was able to perform at a collegiate level in volleyball. On physical examination, there was no pain throughout the lower leg and full muscle strength. Radiographs were obtained at this time (Fig. 3) demonstrating intact tibial intramedullary nail with resolution of all but one residual cortical defect as seen on the lateral radiograph.
Discussion
Stress fractures occur throughout the body with an incidence in athletes ranging from 1% to 2.6% [1, 5]. Tibial stress fractures are most common among athletes with one review demonstrating an incidence of 49% [5]. Tibial stress fractures have been described in athletes, malnourished individuals, and military recruits [1, 2, 3, 4, 5, 6, 7]. Risk factors for stress fractures include intrinsic and extrinsic factors. These intrinsic or extrinsic factors include malnourished individuals, nutritional deficiencies, metabolic disorders, repetitive submaximal stresses, and a narrow tibial width [1, 8]. Prevention of stress fractures may require training alterations such as a decrease in training intensity, use of proper shoe wear, and rest days for athletes and education among female athletes on nutritional wellness 1. Typically, these fractures can be managed non-operatively with activity modification or a course of immobilization for weeks to months may be necessary [1, 2, 3, 4, 5, 6, 7]. When conservative therapy fails for tibial shaft stress fracture and patients clinically have pain over the anterior tibia and limitations of activities with radiographic changes, it may be necessary to move forward with surgical intervention. Stress fractures result from an imbalance of bone formation and resorption secondary to repetitive loads [1]. When excessive stresses are placed onto the bone after muscle fatigue and other factors, stress fractures may develop. Early stages of tibial stress fractures often present normal radiographically [2]. Anterior tibial stress fractures are often described as being unstable fractures secondary to their low healing capacity [3]. Pain relief and excellent functional outcomes after tibial intramedullary nailing have been described [1, 2, 3, 4, 9]. Stress fractures of the anterior tibial cortex may result in complete fracture if left untreated [1, 10]. A case report of a ballet dancer that underwent tibial intramedullary nailing after sustaining a complete fracture secondary to a tibial stress fracture was described. The patient had failed conservative treatments of activity modification, rest, and bone stimulation. She then had transcortical drilling with bone grafting. After failing these modalities, the patient sustained a complete fracture, at which time they performed an intramedullary tibial nail. The patient had an excellent functional outcome and was able to return to their prior activity level [3]. Orava et al. described drilling and bone grafting with immobilization of athletes for 6 months. Rehabilitation in his cohort lasted 4–6 months after immobilization for a total post-operative course of approximately 1 year [3]. Electromagnetic stimulation has been described as a treatment modality for anterior tibial stress fractures. In one series, seven of the eight patients treated had complete healing at 8.7 months with one patient requiring a bone grafting procedure [1]. A case series by Chang and Harris described five patients who underwent intramedullary nailing for recalcitrant tibial stress fractures. Each patient presented with a narrowed medullary canal, thickened anterior cortex, and a single linear unicortical fracture line. All patients failed a course of non-operative management for 1 year. Following reamed, unlocked tibial nailing, all patients reported good or excellent functional outcomes [3]. A recent systematic review for surgically treated anterior stress fractures in athletes demonstrated a complication rate exceeding 25% among all treatment options over a 25-year period. Of the cohort, close to 88% had symptom resolution after surgical treatment. The most commonly performed procedure was compression plating with 15 of the 115 patients undergoing intramedullary tibial nailing. Close to 95% of patients were able to return to athletic activity following surgical intervention among all surgical procedures performed [11].
Conclusion
Our case describes a high-level collegiate bound athlete with multiple cortical defects throughout the anterior tibial cortex. Prior reports describe singular cortical defects, and this case offers a rare glimpse into the management of multiple stress fractures of the anterior tibial cortex and her clinical sequela following surgery. Our patient failed non-operative management and underwent intramedullary tibial nailing. At over 2 years postoperatively, the patient had no pain, full function and had returned to collegiate athletics with an excellent outcome. Intramedullary tibial nailing is a viable option for surgical treatment in athletes failing conservative therapy for anterior tibial stress fractures, offering pain relief and good outcomes.
Clinical Message
Tibial stress fractures can be difficult to manage, especially in the high-level athlete, due to high demands and return to sport. When conservative therapy fails, surgical intervention may be necessary. There have been many described techniques with varying outcomes. Intramedullary tibial nailing in tibial stress fractures offers patients the ability to immediately weight bear, decrease pain, and return to their prior activity level.
References
1. Boden BP, Osbahr DC. High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-53.
2. Chang PS, Harris RM. Intramedullary nailing for chronic tibial stress fractures. A review of five cases. Am J Sports Med 1996;24:688-92.
3. Plasschaert VF, Johansson CG, Micheli LJ. Anterior tibial stress fracture treated with intramedullary nailing: A case report. Clin J Sports Med 1995;5:58-61.
4. Varner KE, Younas SA, Lintner DM, Marymont JV. Chronic anterior midtibial stress fractures in athletes treated with reamed intramedullary nailing. Am J Sports Med 2005;33:1071-6.
5. Snyder RA, Koester MC, Dunn WR. Epidemiology of stress fractures. Clin Sports Med 2006;25:37-52.
6. Milner CE, Ferber R, Pollard CD, Hamill J, Davis IS. Biomechanical factors associated with tibial stress fracture in female runners. Med Sci Sports Exerc 2006;38:323-8.
7. Kahanov L, Eberman LE, Games KE, Wasik M. Diagnosis, treatment, and rehabilitation of stress fractures in the lower extremity in runners. Open Access J Sports Med 2015;6:87-95.
8. Giladi M, Milgrom C, Simkin A, Stein M, Kashtan H, Margulies J, et al. Stress fractures and tibial bone width. A risk factor. J Bone Joint Surg Br 1987;69:326-9.
9. Dailey SK, Archdeacon MT. Chronic bilateral tibial stress fractures with valgus treated with bilateral intramedullary nailing: A case report. J Orthop Case Rep 2014;4:39-43.
10. Pandya NK, Webner D, Sennett B, Huffman GR. Recurrent fracture after operative treatment for a tibial stress fracture. Clin Orthop Relat Res 2006;456:254-8.
11. Chaudhry ZS, Raikin SM, Harwood MI, Bishop ME, Ciccotti MG, Hammoud S. Outcomes of surgical treatment for anterior tibial stress fractures in athletes: A systematic review. Am J Sports Med 2019;47:232-40.
 |
 |
| Dr. Devin Collins | Dr. David Antekeier |
| How to Cite This Article: Collins DW, Antekeier DP. The use a prophylactic intramedullary tibial nail for a stress fracture in a high-level athlete. Journal of Orthopaedic Case Reports 2020 December;10(9): 114-117. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


