
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]Role of Sclerotherapy in the management of aneurysmal bone cyst and it’s advantages over conventional surgical curettage in smaller lesions.
Case Report | Volume 11 | Issue 1 | JOCR January 2021 | Page 1-4 | Kapil Bansal, Swarnesh Baskaran, Anshul Dahuja, Nikhil Gupta. DOI: 10.13107/jocr.2021.v11.i01.1940
Authors: Kapil Bansal[1], Swarnesh Baskaran[1], Anshul Dahuja[1], Nikhil Gupta[1]
[1]Department of Orthopaedics, Guru Gobind Singh Medical College Hospital, Faridkot, Punjab, India.
Address of Correspondence:
Dr. Swarnesh Baskaran,
Room No. 23, PG Hostel, Guru Gobind Singh Medical College, Faridkot – 151 203, Punjab, India.
E-mail: swarnesh1193@gmail.com
Abstract
Introduction: Aneurysmal bone cyst (ABC) is an intraosseous arteriovenous malformation, usually treated by surgical excision but with higher recurrence rates. The occurrence of this lesion in navicular bone is a rare entity. Repetitive sclerotherapy using 3% polidocanol is a minimally invasive, safer method of treatment for ABCs.
Methods: A patient of ABC of the navicular bone precisely diagnosed through X-ray, MRI, and biopsy was given periodic injections of 4 ml of 3% polidocanol under aseptic precautions from April 2018 to July 2018. A total of four injections given at an interval of 1 month.
Results: Regular follow-up done for 1 year. At the end of all the four injections, the lesion healed completely with a relief in presenting symptoms. No complications were reported. At 3 months post-therapy, the patient was able to walk without pain. After 1 year of follow-up, the patient was symptom-free with no signs of recurrence.
Conclusion: Surgical resection/curettage has higher chances of recurrence; therefore, usage of intralesional sclerotherapy agent polidocanol should be considered the treatment of choice in the lesions smaller than 5 cm.
Keywords: Aneurysmal bone cyst, sclerotherapy, polidocanol.
Introduction
An aneurysmal bone cyst (ABC) is neither a cyst nor a neoplasm. The current theory is that the lesion is an intraosseous arteriovenous malformation [1]. Thus, it is a benign blood-filled lesion with a cyst-like wall predominantly of fibrous tissue and surrounded by a thin layer of periosteal new bone [2, 3, 4, 5]. The foot is a relatively uncommon location for an ABC. To the best of our knowledge, no previous case of ABC has been reported in the navicular bone. In the case reported here, an extensive lesion in the navicular was treated with an intralesional sclerotherapy agent polidocanol. Repetitive sclerotherapy using polidocanol is a minimally invasive, safer method of treatment for ABCs as compared with intralesional excision and bone grafting [6].
Case Report
An 18-year-old man in otherwise good health presented complaining of the right midfoot pain and swelling for 7 months, worsening over the preceding 3 months. He stated that he could walk, but this was associated with pain. A 2 × 3 cm firm, tender mass was palpated on the medial aspect of his right midfoot (Fig. 1).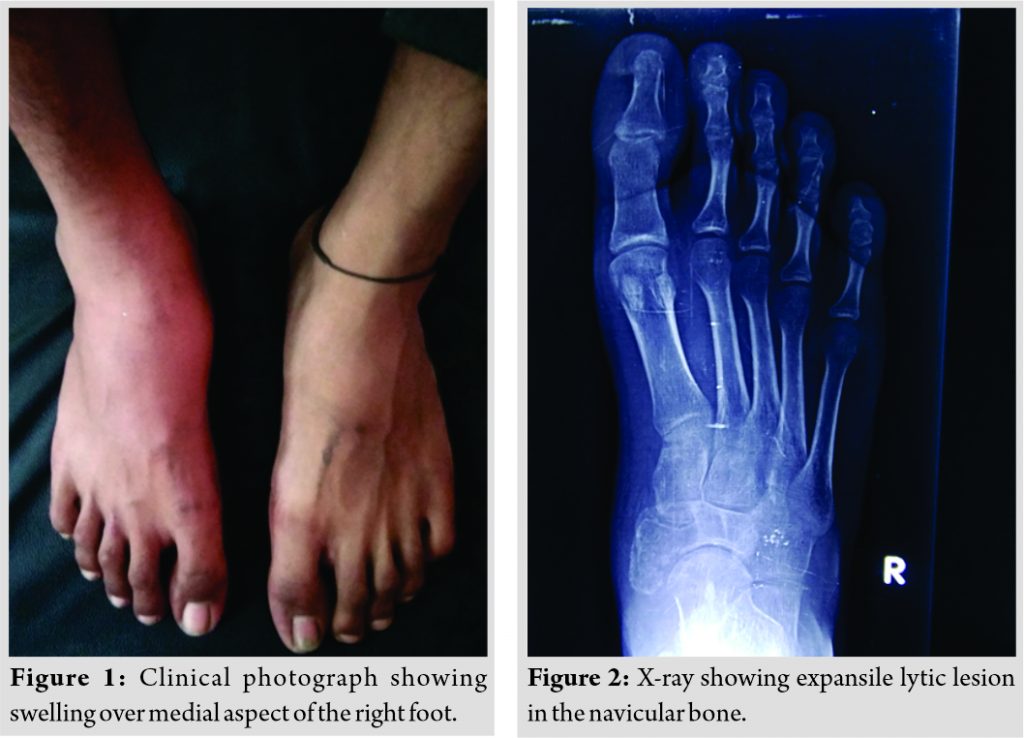
He had full range of motion at his ankle and limited inversion and eversion secondary to pain. A roentgenogram (Fig. 2) showed an expansile, lytic lesion in the navicular bone. Magnetic resonance imaging (Fig. 3-5) shows altered signal intensity over navicular bone of size 2.1 × 2.8 cm with mild edema and infiltration over surrounding soft tissues.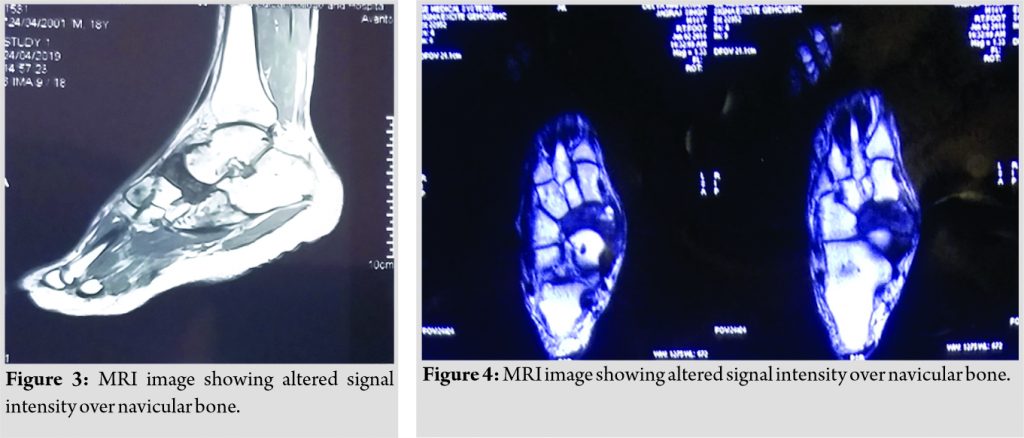
No other associated lesions were seen. Under strict aseptic precautions, biopsy was taken, it was a thick column of blood aspirate, and results (Fig. 6) were consistent with ABC. In view of high recurrence rate after curettage of ABC, the primary procedure of intralesional sclerotherapy was planned. Under the aseptic condition, hypodermic needle inserted into the lesion with the help of image intensifier, aspirated to confirm the site followed by intralesional injection of polidocanol, a sclerotherapy agent at a dosage of 2 mg/kg, with the patient being 60 kg a total of 120 mg, was given. It was performed as a daycare procedure and carried out under local anesthesia. Early rehabilitation was performed with no mode of immobilization. Four such doses were given periodically at an interval of 1 month under aseptic precautions using the same aspiration and injection technique. The response was regularly observed with roentgenograms in each visit. The outcome seems to be markedly appreciable since the first injection and at the end of all the four injections, lesion found to be remitted completely and the patient improved greatly in view of symptoms. No complications were reported. At 3 months post-therapy (Fig. 7, 8), roentgenogram was done and the patient was able to walk without pain and range of movements was full and painless in ankle and subtalar joint.
The response was regularly observed with roentgenograms in each visit. The outcome seems to be markedly appreciable since the first injection and at the end of all the four injections, lesion found to be remitted completely and the patient improved greatly in view of symptoms. No complications were reported. At 3 months post-therapy (Fig. 7, 8), roentgenogram was done and the patient was able to walk without pain and range of movements was full and painless in ankle and subtalar joint.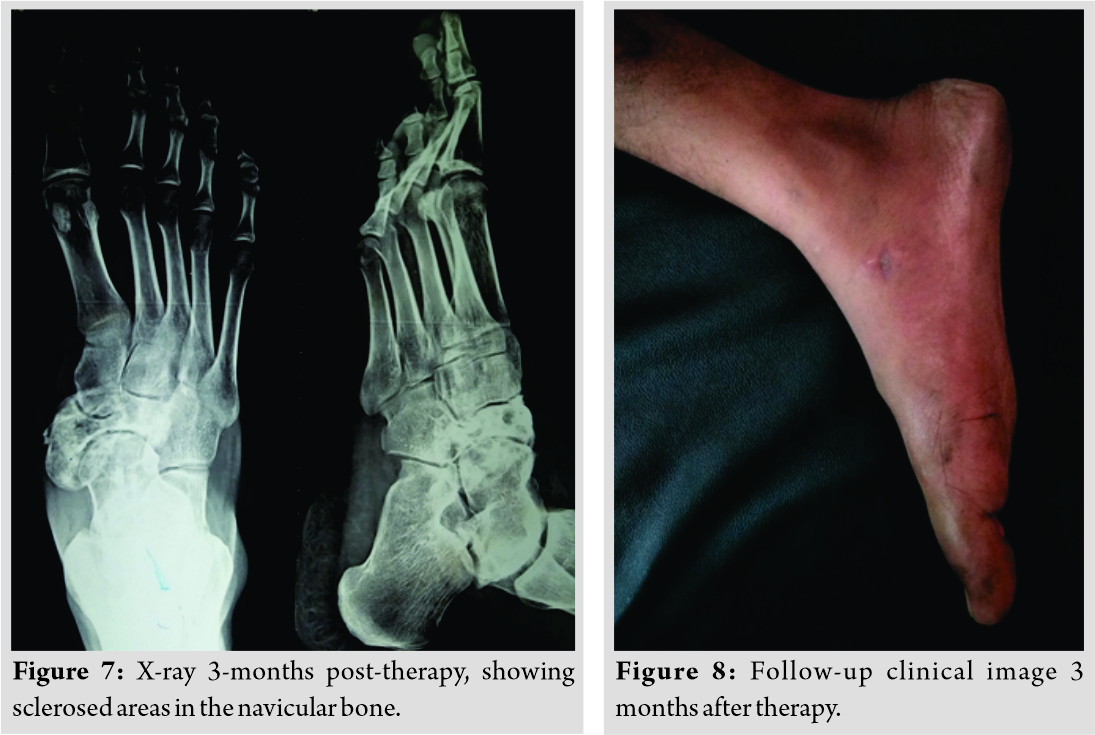 The patient is symptom-free and shows no signs of recurrence at 1-year follow-up (Fig. 9).
The patient is symptom-free and shows no signs of recurrence at 1-year follow-up (Fig. 9).
Discussion
Pain and/or swelling are the most common symptoms of an ABC on presentation [7]. Patients notice this increase in size due to both the lesion increasing in size as well as associated swelling. The vast majority (~80%) of patients with primary ABCs are younger than 20 years old. Women are affected slightly more often than men. ABC shows an evident predilection for the vertebral column and long bones – particularly the femur, humerus, tibia, and fibula [8]. The feet account for approximately 4% of ABCs [9]. The natural history is characterized by a benign lesion that does not metastasize yet can be difficult to eradicate with simple curettage. The greatest clinical problem associated with the ABCs is local recurrence. As reported for two large series, the factors associated with a higher recurrence rate in ABC seemed to be young age and/or the size of the cyst. In addition, Tillman et al. noted that cysts localized in the major limb bones had a higher recurrence rate. The cause of ABCs remains unclear, although several theories have been suggested. One theory by Lichtenstein proposes that the lesion originates as a circulatory disturbance, for instance, in response to increased intraosseous venous pressure. This engorged vascular bed then causes resorption of spongy bone, erosion of cortical bone, and expansion of the lesion. A second theory proposes that the cyst appears as a dilated arteriovenous shunt. A third theory by Bernier and Bhaskar proposes that the ABC begins as a focus of intramedullary hemorrhage and that the lesion represents an unusual reparative response to hemorrhage. The fourth theory by Biesecker et al. proposes that ABCs occur secondary to intraosseous hemodynamic changes in an antecedent lesion. The association of an ABC with other lesions 50% of the time supports this theory. The associated lesions have included non-ossifying fibroma, chondroblastoma, solitary bone cyst, giant cell tumor of bone, osteoblastoma, giant cell reparative granuloma, fibrous dysplasia, fibromyxoma, and osteosarcoma. An ABC has been described as evolving through four radiologic stages: Initial, active, stabilization, and healing. In the initial phase, the lesion is characterized by a well-defined area of osteolysis with the discrete elevation of the periosteum. This is followed by an active growth phase, in which the lesion grows rapidly with progressive destruction of bone and development of the characteristic “blown out” radiologic appearance. The growth phase is succeeded by a period of stabilization, in which the characteristic “soap-bubble” appearance develops, as a result of maturation of the bony shell. Finally, healing results in progressive calcification and ossification, with the lesion transformed into a dense, bony mass. Radiographs typically will show an eccentric, lytic lesion with an expanded, remodeled “blown-out” or “ballooned” bony contour of the host bone [10, 11, 12, 13, 14]. A definitive diagnosis of ABC can be made only by its microscopic features. The lesion is a pseudocyst composed of blood pools of variable sizes, lined not by endothelium but by spindle-shaped cells and multinucleated giant cells. The stroma is composed of giant cells, fibroblasts, capillaries, extravasated blood cells, and hemosiderin. The walls of the blood pools do not contain elastic elements or smooth muscle and, thus, do not mimic blood vessels. Before any therapy can be considered, it must be determined whether the ABC is associated with another condition. If a more aggressive lesion is present, treatment must be directed toward the more aggressive component. Conventional treatment has been directed toward the surgical removal of the entire lesion, or of as much as possible, followed by packing with bone graft. This common method of treatment is usually curative. Incomplete surgical removal is the most important factor in recurrence. Recurrence rates range from 10% to 44%, with 90% recurring within 2 years [5, 7, 10, 15]. Sequential percutaneous administration of polidocanol is a safe, simple procedure with an excellent cure rate for ABC. The use of polidocanol is a definite advancement over previous sclerotherapy regimens that relied on alcoholic zein solutions, which were more toxic and had serious adverse effects after spill-out into nearby tissues [16, 17]. Being a daycare procedure of negligible risk of morbidity and no scar formation with efficacy exceeding 90%, it outweighs the disadvantage of multiple injections and prolonged treatment.
Conclusion
Surgical resection/curettage has higher chances of recurrence, and so usage of intralesional sclerotherapy agent polidocanol should be considered to be the treatment of choice in the lesions smaller than 5 cm, as was the case with the patient described in this report.
Clinical Message
Sclerotherapy possesses a great advantage of being minimally invasive technique and with less recurrence rates. Being a daycare procedure with early rehabilitation, it offers a comfortable and compliant mode of therapy for the patients.
References
1. Mirra JM. Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA: Lea and Febiger; 1989. p. 1233-4.
2. Jaffe HL. Aneurysmal bone cyst. Bull Hosp Joint Dis 1950;11:3-13.
3. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg 1942;44:1004-25.
4. Lichtenstein L. Aneurysmal bone cyst. A pathological entity commonly mistaken for giant‐cell tumor and occasionally for hemangioma and osteogenic sarcoma. Cancer 1950;3:279-89.
5. Lichtenstein L. Aneurysmal bone cyst; further observations. Cancer 1953;6:1228-37.
6. Varshney MK, Rastogi S, Khan SA, Trikha V. Is sclerotherapy better than intralesional excision for treating aneurysmal bone cysts? Clin Orthop Relat Res 2010;468:1649-59.
7. Vergel De Dios AM, Bond JR, Shives TC, McLeod RA, Unni KK. Aneurysmal bone cyst. A clinicopathologic study of 238 cases. Cancer 1992;69:2921-31.
8. Bansal K, Dahuja A, Kalia A. Two year follow up of giant aneurysmal bone cysts managed with an autologous non vascularized fibular strut graft. J Adv Med Dent Scie Res 2016;4:254-8.
9. Wold E. Atlas of Orthopaedic Pathology. Philadelphia, PA: W.B. Saunders; 1990. p. 232-3.
10. Dahlin DC, McLeod RA. Aneurysmal bone cyst and other nonneoplastic conditions. Skeletal Radiol 1982;8:243-50.
11. Donaldson WF Jr. Aneurysmal bone cyst. J Bone Joint Surg 1962;44:25-40.
12. Hudson TM. Fluid levels in aneurysmal bone cysts: A CT feature. AJR Am J Roentgenol 1984;142:1001-4.
13. Hudson TM. Radiologic-Pathologic Correlation of Musculoskeletal Lesions. Baltimore, MD: Lippincott Williams and Wilkins Company; 1987. p. 261-5.
14. Kransdorf MJ, Sweet DE. Aneurysmal bone cyst: Concept, controversy, clinical presentation, and imaging. AJR Am J Roentgenol 1995;164:573-80.
15. Ruiter DJ, Van Rijssel TG, Van der Velde EA. Aneurysmal bone cysts: A clinicopathological study of 105 cases. Cancer 1977;39:2231-9.
16. Falappa P, Fassari FM, Fanelli A, Genovese E, Ascani E, Crostelli M, et al. Aneurysmal bone cysts: Treatment with direct percutaneous Ethibloc injection: Long-term results. Cardiovasc Intervent Radiol 2002;25:282-90.
17. Adamsbaum C, Mascard E, Guinebretière JM, Kalifa G, Dubousset J. Intralesional Ethibloc injections in primary aneurysmal bone cysts: An efficient and safe treatment. Skeletal Radiol 2003;32:559-66.
 |
 |
 |
 |
| Dr. Kapil Bansal | Dr. Swarnesh Baskaran | Dr. Anshul Dahuja | Dr. Nikhil Gupta |
| How to Cite This Article: Bansal K, Baskaran S, Dahuja A, Gupta N. A Rare Case of Aneurysmal Bone Cyst – Navicular Bone Treated by Intralesional Sclerotherapy Agent Polidocanol. Journal of Orthopaedic Case Reports 2021 January;11(1):1-4. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


