
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Surgical approach should be changed to the classic Henry’s approach when the surgeon observes anatomical anomalies in distal volar forearm.
Case Report | Volume 11 | Issue 3 | JOCR March 2021 | Page 42-44 | Dharmesh Patel, Rajeev Vohra, Avtar Singh . DOI: 10.13107/jocr.2021.v11.i03.2080
Authors: Dharmesh Patel[1], Rajeev Vohra[1], Avtar Singh[1]
[1]Department of Orthopaedic, Amandeep Hospital, G.T. Road, Near Model Town, Amritsar. Punjab. India.
Address of Correspondence:
Dr. Dharmesh Patel,
Amandeep Hospital, G.T. Road, Near Model Town, Amritsar. Punjab – 143 001, India.
E-mail: dharmesh_19872003@yahoo.co.in
Abstract
Introduction: Volar locking plate fixation of distal radius fractures is commonly performed because of its good clinical outcomes. The flexor carpi radialis (FCR) approach is one of the most popular approaches to dissecting the volar side of the distal radius because of its simplicity and safety. We describe an extremely rare case of an absent FCR identified during a volar approach for fixation of a distal radius fracture.
Case Report: A 40-year-old male with comminuted distal radius fracture underwent surgery using the usual FCR approach and volar locking plate. We could not identify the absence of the FCR tendon preoperatively because of severe swelling of the distal forearm. At first, we wrongly identified the palmaris longus (PL) tendon as the FCR because it was the tendinous structure at the most radial location of the volar distal forearm. When we found the median nerve just radial to the PL tendon, we were then able to identify the anatomical abnormality in this case. To avoid iatrogenic neurovascular injuries, we changed the approach to the classic Henry’s approach.
Conclusion: Although the FCR approach is commonly used for fixation of distal radius fractures because of its simplicity and safety, this is the first report of complete absence of the FCR during the commonly performed volar approach for fixation of a distal radius fracture, to our knowledge. Because the FCR is designated as a favorable landmark because of its superficially palpable location, strong and thick structure, and rare anatomical variations, there is the possibility of iatrogenic complications in cases of the absence of the FCR. We suggest that surgeons should have a detailed knowledge of the range of possible anomalies to complete the fixation of a distal radius fracture safely.
Keywords: Flexor carpi radialis, Anomaly, Distal radius fracture, Volar approach, Flexor carpi radialis approach.
Introduction
Volar approach is commonly used for fractures for surgical management involving the lower end radius, some carpal bone fractures, and pathologies involving the lower end radius and wrist. Flexor carpi radialis (FCR) is an important landmark utilized for planning the incision as well as performing the superficial dissection. Volar locking plate fixation of distal radius fractures is commonly performed because of its good clinical outcomes [1, 2]. The FCR approach is one of the most popular approaches to fixing distal radius fractures from the volar side because of its simplicity and safety [2, 3]. However, surgeons have reported various types of anatomical variation and anomalies of the distal volar forearm structures including, among others, bifurcation of the median nerve, an anomalous course of the palmar cutaneous branch (PCB) of the median nerve, the accessory muscles of the flexor tendon, and have warned about consequent iatrogenic injuries during surgery [4, 5]. Here, we describe an extremely rare case of the absence of the FCR, identified during the volar approach for fixation of a distal radius fracture.
Case Report
A 40-year-old dominant right-handed male working in private insurance company with no significant medical history suffered a distal radius fracture of the left hand due to road traffic accident (Fig. 1).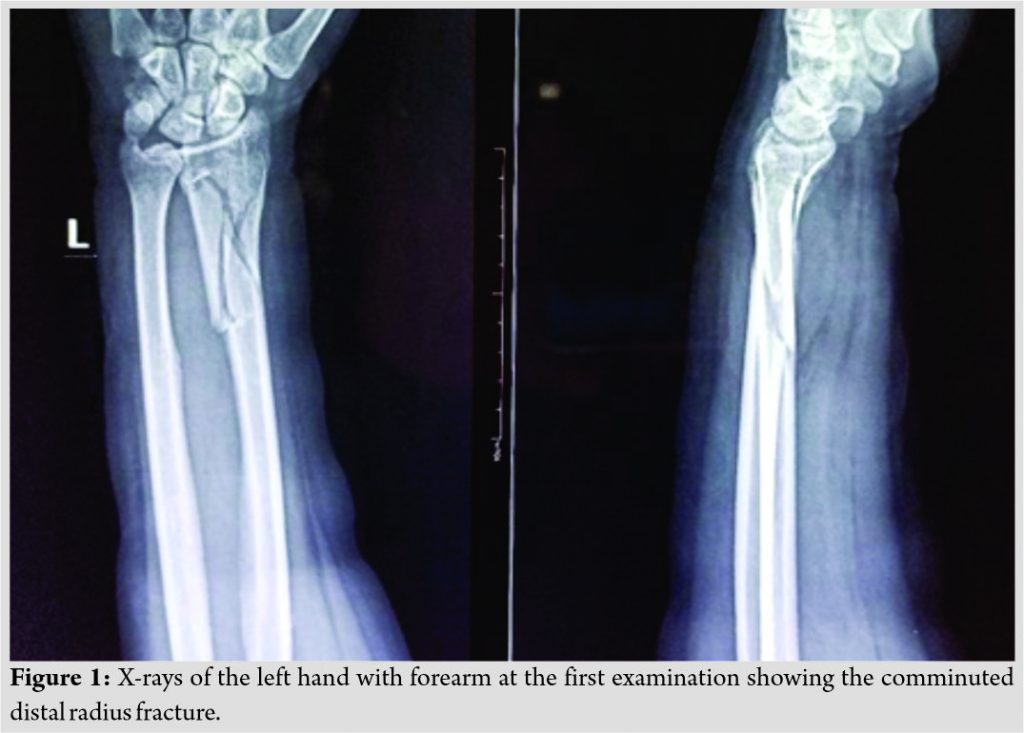 On clinical examination, he could move the fingers of the hand and there was no evidence of any neurovascular deficit distal to the injury. Crepitus could be felt in the distal part of the radius just proximal to wrist joint and movements around the wrist were painful and limited. There were no other associated injuries, and medical history was not significant for any medical illness. A clinical diagnosis of the fracture of lower end radius was made and radiographs were consistent with the clinical diagnosis. Radiographs showed a comminuted fracture of the distal third radius with intra-articular extension for which open reduction and internal fixation through a volar FCR approach was planned. He underwent the definitive treatment of open reduction and internal fixation of the fractures distal radius under regional anesthesia. We had planned to fix the distal radius fracture using the usual FCR approach using 3.5 mm distal end radius locking plate. We could not identify the absence of the FCR tendon preoperatively because of severe swelling of the distal forearm. The incision was made at its usual location and we identified one tendon in the superficial plane which we thought was FCR, but when we traced the tendon proximally it started thinning without any muscle belly and when traced distally to its attachment, it was confirmed to be tendon of palmaris longus (PL). We could not find any tendon between PL and the traced radial artery. At that stage, we realized that FCRL was absent in that patient.
On clinical examination, he could move the fingers of the hand and there was no evidence of any neurovascular deficit distal to the injury. Crepitus could be felt in the distal part of the radius just proximal to wrist joint and movements around the wrist were painful and limited. There were no other associated injuries, and medical history was not significant for any medical illness. A clinical diagnosis of the fracture of lower end radius was made and radiographs were consistent with the clinical diagnosis. Radiographs showed a comminuted fracture of the distal third radius with intra-articular extension for which open reduction and internal fixation through a volar FCR approach was planned. He underwent the definitive treatment of open reduction and internal fixation of the fractures distal radius under regional anesthesia. We had planned to fix the distal radius fracture using the usual FCR approach using 3.5 mm distal end radius locking plate. We could not identify the absence of the FCR tendon preoperatively because of severe swelling of the distal forearm. The incision was made at its usual location and we identified one tendon in the superficial plane which we thought was FCR, but when we traced the tendon proximally it started thinning without any muscle belly and when traced distally to its attachment, it was confirmed to be tendon of palmaris longus (PL). We could not find any tendon between PL and the traced radial artery. At that stage, we realized that FCRL was absent in that patient.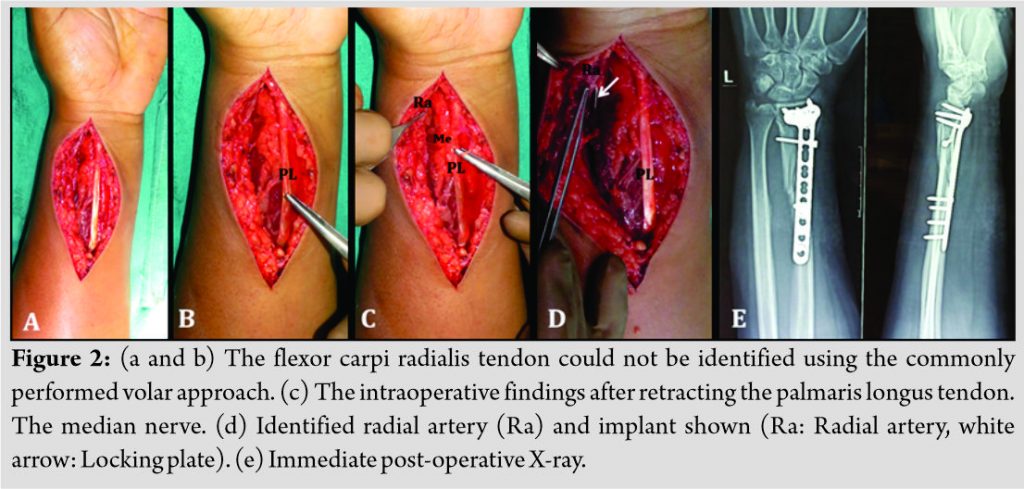 We wrongly identified the PL tendon as the FCR because it was the tendinous structure at the most radial location of the volar distal forearm. When we found the median nerve just radial to the PL tendon, we were then able to identify the anatomical abnormality described in this case and immediate post-operative X-ray (Fig. 2a-e). Therefore, we changed the approach to the classic Henry’s approach after we had identified and gently protected the PCB. When we exposed and protected the radial artery through the same incision, we exposed the flexor pollicis longus (FPL), this must be retracted ulnarly, after the FPL is bluntly retracted, the pronator quadratus (PQ) is seen and incise the radial and distal borders of the PQ, elevating the muscle off the volar radius and fixed the fracture rigidly using a 3.5 mm distal end radius locking plate Nebula (stainless steel), Amritsar, Punjab, India. Four months after the operation, the patient had no pain or neurologic problems and complete bone union of the distal radius fracture. The patient returned to his work without any disability. We checked for the existence of an FCR tendon in the opposite forearm and could identify the thick FCR tendon by palpation.
We wrongly identified the PL tendon as the FCR because it was the tendinous structure at the most radial location of the volar distal forearm. When we found the median nerve just radial to the PL tendon, we were then able to identify the anatomical abnormality described in this case and immediate post-operative X-ray (Fig. 2a-e). Therefore, we changed the approach to the classic Henry’s approach after we had identified and gently protected the PCB. When we exposed and protected the radial artery through the same incision, we exposed the flexor pollicis longus (FPL), this must be retracted ulnarly, after the FPL is bluntly retracted, the pronator quadratus (PQ) is seen and incise the radial and distal borders of the PQ, elevating the muscle off the volar radius and fixed the fracture rigidly using a 3.5 mm distal end radius locking plate Nebula (stainless steel), Amritsar, Punjab, India. Four months after the operation, the patient had no pain or neurologic problems and complete bone union of the distal radius fracture. The patient returned to his work without any disability. We checked for the existence of an FCR tendon in the opposite forearm and could identify the thick FCR tendon by palpation.
Discussion
The FCR originates from the medial epicondyle of the humerus and inserts into the trapezius, the second metacarpal, and the third metacarpal bones, and functionally contributes to the motion in flexion and the radial deviation of the wrist joint [6]. Although there have been reports of anatomical variations in its origin, insertion, and the presence of additional slips, complete absence of the FCR is an extremely rare anomaly that has been reported only twice in English language reports [7, 8]. Rumball et al. [7] reported the absence of the FCR in a young boy undergoing tendon transfer for the reconstruction of posterior interosseous nerve palsy, and Sofos et al. [8] reported the anomaly in a case of ligament reconstruction and tendon interposition arthroplasty for thumb carpometacarpal joint arthritis. Both reports focused on the need to avoid using a donor tendon in cases of absent FCR. However, the FCR also plays a very important role as a landmark in the distal forearm, and most surgery on the distal volar forearm is likely to be performed based on the location of the FCR [3, 9]. To the best of our knowledge, this is the first report of an absent FCR identified during the commonly performed volar approach for fixation of a distal radius fracture. Because important neurovascular structures exist close together in the distal volar forearm, there have been many complications reported for volar plating of distal radius fractures, including injuries to the median nerve, the PCB of the median nerve, and the radial artery [4, 10]. The FCR is designated as a favorable landmark because of its superficially palpable location, strong and thick structure, and rare anatomical variations. To avoid iatrogenic neurovascular injuries, detailed anatomical studies of the distal volar forearm have been based on the FCR [3, 9]. However, in rare cases, where the FCR is absent, there is the possibility of misidentifying the PL as the FCR based on its most radial location in the distal volar forearm, especially under conditions of soft-tissue swelling around the distal forearm resulting from high-energy force. We suggest that the surgical approach should be changed to the classic Henry’s approach when the surgeon observes serious anatomical anomalies in the distal volar forearm [4]. Although the FCR approach is commonly used for fixation of distal radius fractures because of its simplicity and safety, various types of anatomical variations and anomalies of the distal volar forearm structures including the median nerve, the PCB of the median nerve, and the flexor tendon have been reported. Because the FCR is designated as a favorable landmark because of its superficially palpable location, strong and thick structure, and rare anatomical variations, there is the possibility of iatrogenic complications in cases where the FCR is absent. We suggest that surgeons should have a detailed knowledge about the range of possible anomalies to complete the fixation of a distal radius fracture safely.
Conclusion
It is important for the operating surgeon to have a detailed knowledge of the possible anomalies in the distal forearm, and in cases with absent FCR, the surgical approach or plan may need to be altered during surgery. In our case, we went ahead with our surgical plan and fixation of the lower end of the radius was done. The congenital absence of FCR should be kept in mind when tendon transfer of FCR is planned or any ligament reconstruction using FCR is planned. The knowledge of this anomaly can prevent iatrogenic injuries to neurovascular structures during volar plating of the radius. We are not aware of any case where the absence of FCR has been reported during volar plating of distal end radius.
Clinical Message
While fixing distal end radius, fracture with volar approach always keep in mind may be absent of FCR tendon.
References
1. Koval KJ, Harrast JJ, Anglen JO, Weinstein JN. Fractures of the distal part of the radius. The evolution of practice over time. Where’s the evidence? J Bone Joint Surg Am 2008;90:1855-61.
2. Alluri RK, Hill JR, Ghiassi A. Distal radius fractures: Approaches, indications, and techniques. J Hand Surg Am 2016;41:845-54.
3. Conti Mica MA, Bindra R, Moran SL. Anatomic considerations when performing the modified Henry approach for exposure of distal radius fractures. J Orthop 2016;14:104-7.
4. Jones C, Beredjiklian P, Matzon JL, Kim N, Lutsky K. Incidence of an anomalous course of the palmar cutaneous branch of the median nerve during volar plate fixation of distal radius fractures. J Hand Surg Am 2016;41:841-4.
5. Lee YM, Song SW, Sur YJ, Ahn CY. Flexor carpi radialis brevis: An unusual anomalous muscle of the wrist. Clin Orthop Surg 2014;6:361-4.
6. Bishop AT, Gabel G, Carmichael SW. Flexor carpi radialis tendinitis. Part I: Operative anatomy. J Bone Joint Surg Am 1994;76:1009-14.
7. Rumball KM, Tonkin MA. Absence of flexor carpi radialis. J Hand Surg Br 1996;21:778.
8. Sofos SS, Riaz M. Absence of flexor carpi radialis during an elective carpo-metacarpal arthroplasty of the thumb: A rare anatomical variation. Case Rep Med 2016;2016:7853487.
9. McCann PA, Amirfeyz R, Wakeley C, Bhatia R. The volar anatomy of the distal radius-an MRI study of the FCR approach. Injury 2010;41:1012-4.
10. Davis DI, Baratz M. Soft tissue complications of distal radius fractures. Hand Clin 2010;26:229-35.
 |
 |
 |
| Dr. Dharmesh Patel | Dr. Rajeev Vohra | Dr. Avtar Singh |
| How to Cite This Article: Patel D, Vohra R, Singh A. Absence of Flexor Carpi Radialis Identified During Volar Approach for Fixation of Distal Radius Fracture: A Case Report. Journal of Orthopaedic Case Reports 2021 March;11(3): 42-44. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


