
When presented with a case of osteochondroma of the distal radius in children, carpal tunnel syndrome can also occur.
Dr. Rohit Mahesh Sane,
Department of Orthopaedics, D Y Patil University School of Medicine, Navi-Mumbai, Maharashtra. India.
E-mail: dr.sanerohit@gmail.com
Introduction: An exostosis is a benign growth of bone, which when capped with cartilage is called osteochondroma, which can appear as solitary or multiple, mostly affecting the long bones, pelvis, and shoulder region. The prevalence of known solitary exostosis is 1–2% in the general population. They are slow growing lesions with rare malignant transformation. In patients with a solitary exostosis, the chance of developing a chondrosarcoma out of an exostosis is around 1%.
Case Report: A 12-year-old boy presented to our outpatient department with complaints of pain, and swelling at the right wrist since 1 year and tingling numbness on and around palmar aspect of index and middle finger since 6 months. The swelling was of size 3 cm × 2 cm, Tinel’s sign was positive. His blood parameters were normal. X-ray showed exostoses. Magnetic resonance imaging was suggestive of osteochondroma. Nerve conduction study was normal. Excision biopsy confirmed the diagnosis and also relieved all symptoms.
Conclusion: Our case report is unique in its own way as it reminds us that when presented with a case of osteochondroma of the distal radius in children, carpal tunnel syndrome can also occur.
Keywords: Osteochondroma, carpal tunnel syndrome, exostosis.
An exostosis is a benign growth of bone, which when capped with cartilage, is called osteocartilaginous exostoses (osteochondroma) [1]. Osteochondromas can appear as solitary or multiple, mostly affecting the long bones, pelvis, and shoulder region [1]. The prevalence of known solitary exostosis is 1–2% in the general population [2]. Osteochondromas are slow growing lesions with rare malignant transformation but can raise cosmetic concerns and impinge on local structures, including nerves, vessels and tendons, and leading to symptomatology [3, 4, 5]. In patients with a solitary exostosis, the chance of developing a chondrosarcoma out of an exostosis is around 1% [6, 7, 8]. Single resection of the exostosis with or without further treatment for deformity is the treatment of choice [9, 10, 11]. Here, we present a case report of a 12-year-old boy, with a solitary, mass (exostoses), present on the volar aspect of distal radius, presenting clinically with carpal tunnel syndrome. Surgical intervention led to complete resolution of the patient’s symptoms. The current case report was written according to the published SCARE criteria [12].
A 12-year-old boy with his mother presented to our outpatient department with complaints of pain, and swelling at the right wrist since 1 year. Patient also had complaints of tingling numbness on and around palmar aspect of index and middle finger since 6 months. Patient had no history of trauma/fall on the affected wrist. Patient was apparently alright 1 year back, when he started complaining of pain and started noticing a firm swelling on the volar aspect of his right wrist. Pain was insidious in onset, dull aching in character, not associated with any other symptoms, aggravated by movements and reduced by rest. Swelling was initially the size of a small pea (1 cm × 1 cm), which later increased to the current size of 3 cm × 2 cm. Patient also companied of finding it difficult to hold a pencil/pen for long, as he would then start experiencing tingling numbness on and around palmar aspect of index and middle. Patient had no associated symptoms and family history was non-significant.

On examination of the right wrist joint, swelling (3 cm × 2 cm) was noted on the volar aspect of distal radius (Fig. 1). Skin over the swelling was normal and pinchable. Patient had localized tenderness over and around the swelling. Swelling was firm and bony in consistency. Swelling was non-translucent and non-mobile. Patient had a restricted range of flexion due to pain. Tinel’s sign was positive. Phalen’s test could not be elicited due to pain. Radial pulse was regular, normal in volume, rhythm, and consistency. On investigating, his blood counts were within normal limits, erythrocyte sedimentation rate and C-reactive protein too were within normal limits. X-ray showed an exostosis of 3 cm × 2 cm on the volar aspect, arising from the metaphysio-diaphyseal area of the wrist (Fig. 2). Magnetic resonance imaging showed a well-defined, bony excrescence (3 cm × 2 cm × 2 cm) with a STIR hyperintense cartilaginous cap of maximum thickness of 4 mm involving the antero-medial aspect of radial diaphysis (Fig. 3). Growing away from the joint, indenting the posterior aspect of flexor digitorum superficialis and flexor carpi radialis. The lesion was also minimally displacing the neurovascular bundle on the radial side. The distance between the cartilaginous cap and the neurovascular bundle was around 1.5 mm. The findings were suggestive of osteochondroma. Electromyogram nerve conduction study revealed a normal study.
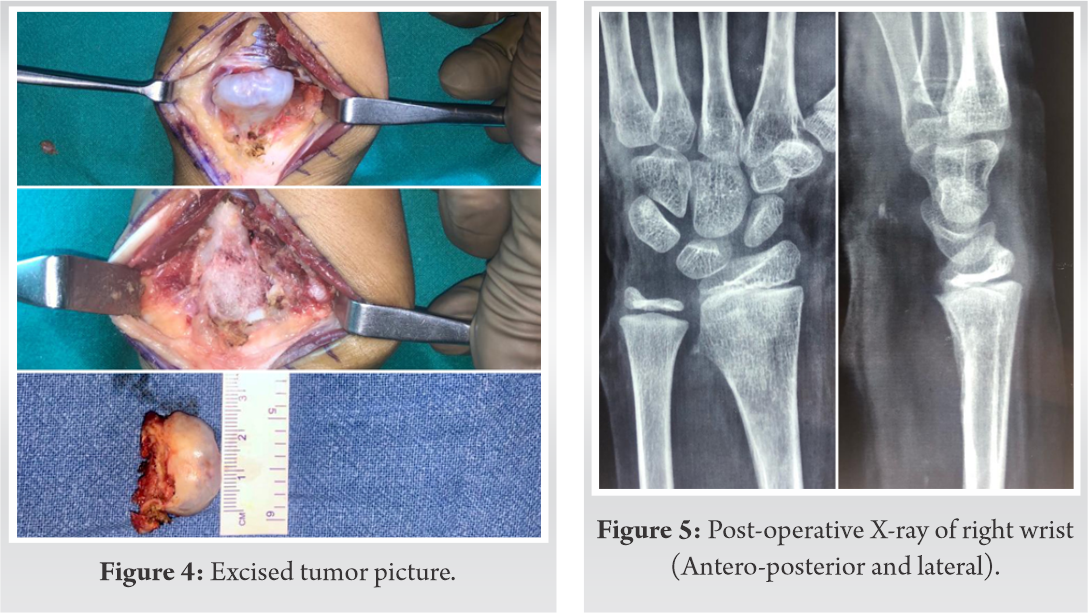
An excision biopsy was planned. The whole mass was excised leaving behind fresh healthy bone, which was sent for histopathology (Fig. 4). Carpal tunnel release and median nerve decompression were done. Post-surgery, the tumor was cleared off the bone (Fig. 5). Histopathology confirmed the diagnosis of osteochondroma. Post-operative management was as regular and the patient was discharged on post-operative day 5. Postoperatively wrist range of motion (ROM) was started on day 1 and continued throughout the stay. Patient’s symptoms of pain and tingling numbness disappeared after surgery. Patient was then followed up at 1 month with full wrist ROM, showing no recurrence.
Osteochondroma can appear as a solitary or multiple exostoses, mostly affecting the long bones, pelvis, and shoulder region, with a prevalence of 1–2% in the general population [1]. Osteochondroma generally originates from the metaphysis of longitudinally growing bones as the site of defects in the periosteum and/or tendon insertion [13]. Osteochondroma first appears during the growth period. Symptoms related to the tumor have been reported in patients aged from their teens to around 50 years who seem to use their hand and fingers excessively [5]. A cartilaginous cap protruding into tendons and joints can be exposed to various kinds of mechanical forces such as tendon gliding and/or joint movement, which can lead to fracture and/or deformation [14]. Osteochondroma of the distal radius, which causes carpal tunnel syndrome, is extremely rare. In our literature research, only three cases have been noted so far. The first was described by Nather and Chong in 1986 [15], when a 47-year-old woman presented with a visible volar lump associated with shooting pain in her thumb and index finger. Intraoperatively, the authors described a ganglion cyst originating from the flexor pollicis longus tendon’s synovial lining; within the cyst, a bony lump was excised and was pathologically consistent with a tendon sheath osteochondroma [15]. In the second case, Hofmann et al. described a 75 year-old diabetic patient who presented with carpal tunnel syndrome and a palpable hardening on the volar distal radius [16]. Moreover, in the third case described by Wong et al., a 78-year-old female presenting with clinically carpal tunnel syndrome and a volar mass over the carpal bones [17]. Moreover, presentation of carpal tunnel syndrome in children is extremely rare, with most of them presenting due to a genetic causes leading to lysosomal storage diseases [18]. In our case report, the patient had no symptoms until a year back, and his symptoms were due to compressive causes rather than organic causes. Carpal tunnel syndrome has presented in a case of osteochondroma of the distal radius, of a 12-year-old boy without any evidence on nerve conduction studies, which makes this report rare.
Our case report is unique in its own way as it reminds us that when presented with a case of osteochondroma of the distal radius in children, carpal tunnel syndrome can also occur.
When presented with a case of osteochondroma of the distal radius in children, carpal tunnel syndrome can also occur. The latter is a possibility and should be looked into in spite of investigations like nerve conduction study being normal.
References
- 1.Aerts BR, Van Heeswijk EJ, Beumer A. Reconstruction of the DRUJ in a young adult after resection of a large exostosis of the distal radius. Strategies Trauma Limb Reconstr 2015;10:123-7. [Google Scholar]
- 2.Trebicz-Geffen M, Robinson D, Evron Z, Glaser T, Fridkin M, Kollander Y, et al. The molecular and cellular basis of exostosis formation in hereditary multiple exostoses. Int J Exp Pathol 2008;89:321-31. [Google Scholar]
- 3.Saglik Y, Altay M, Unai VS, Basari K, Yildiz Y. Manifestations and management of osteochondromas: A retrospective analysis of 382 patients. Acta Orthop Belg 2006;72:748-55. [Google Scholar]
- 4.Lee K, Davies A, Cassar-Pullicino V. Imaging the complications of osteocondromas. Clin Radiol 2002;57:18-28. [Google Scholar]
- 5.Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar]
- 6.Wicklund CL, Pauli RM, Johnston D, Hecht JT. Natural history study of hereditary multiple exostoses. Am J Med Genet 1995;55:43-6. [Google Scholar]
- 7.Verhaar J. Orthopedie. Houten: Bohn Stafleu Van Loghum; 2008. [Google Scholar]
- 8.Roehl HH, Pacifici M. Shop talk: Sugars, bones, and a disease called multiple hereditary exostoses. Dev Dyn 2010;239:1901-4. [Google Scholar]
- 9.Hill RA, Ibrahim T, Mann HA, Siapkara A. Forearm lengthening by distraction osteogenesis in children: A report of 22 cases. J Bone Joint Surg Br 2011;93:1550-5. [Google Scholar]
- 10.Matsubara H, Tsuchiya H, Sakurakichi K, Yamashiro T, Watanabe K, Tomita K. Correction and lengthening for deformities of the forearm in multiple cartilaginous exostoses. J Orthop Sci 2006;11:459-66. [Google Scholar]
- 11.Ip D, Li YH, Chow W, Leong JC. Reconstruction of forearm deformities in multiple cartilaginous exostoses. J Pediatr Orthop B 2003;12:17-21. [Google Scholar]
- 12.Agha RA, Fowler AJ, Saetta A, Barai I, Rajmohan S, Orgill DP. For the SCARE group. The SCARE statement: Consensus-based surgical case report guidelines. Int J Surg 2016;34:180-6. [Google Scholar]
- 13.Motomiya M, Sakazaki T, Iwasaki N. Atypical osteochondroma of the hamate that presented clinically as carpal tunnel syndrome: Report of an extremely rare case and literature review. BMC Musculoskelet Disord 2020;21:231. [Google Scholar]
- 14.Carpintero P, Leon F, Zafra M, Montero M, Berral FJ. Fractures of osteochondroma during physical exercise. Am J Sports Med 2003;31:1003-6. [Google Scholar]
- 15.Nather A, Chong PY. A rare case of carpal tunnel syndrome due to tenosynovial osteochondroma. J Hand Surg Br 1986;11:478-80. [Google Scholar]
- 16.Hofmann AK, Wustner MC, Spier W. Compression neuropathy of the median nerve at the wrist joint caused by chondroma. Handchi Mikrochir Plast Chir 1990;22:96-8. [Google Scholar]
- 17.Wong A, Watson S, Bakula A, Ashmead D. Carpal tunnel syndrome caused by a large osteochondroma. Hand (N Y) 2012;7:438-1. [Google Scholar]
- 18.Meir VN, Smet DL. Carpal tunnel syndrome in children. Acta Orthop Belg 2003;69:387-95. [Google Scholar]








