
Early diagnosis of tuberculosis dactilytis is key factor in preventing major finger deformity. Sarcoidosis can be a misleading diagnosis that can retard adequate therapy.
Dr. Mohamad K Moussa,
Department of Orthopedic Surgery, Zahraa Hospital, University Medical Center. Beirut – Lebanon.
E-mail: mhamadmoussa71976798@gmail.com
Introduction: Skeletal tuberculosis is a rare form of extrapulmonary Mycobacterium tuberculosis infection. When tubular bones are affected, it is called tuberculous dactylitis (TD). This rare entity can be seen in the hand or foot and has been mentioned in a handful of case reports.
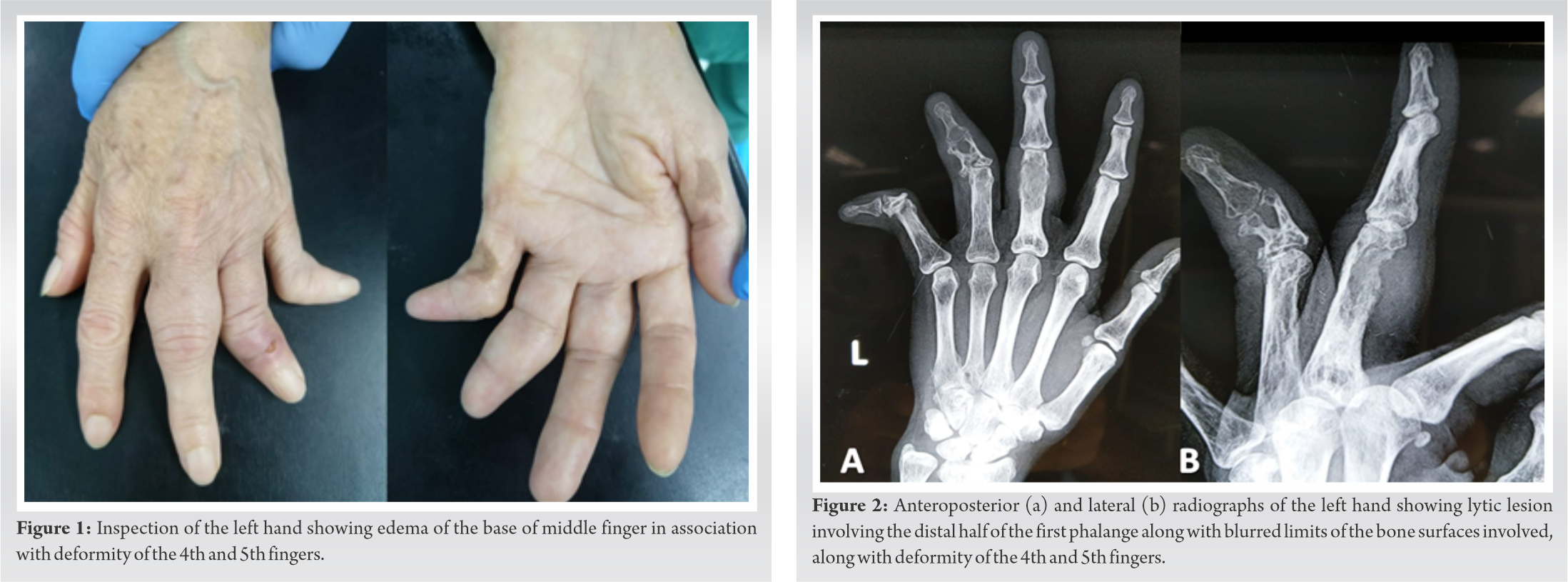
Case Report: A 56-year-old female patient presented to our clinic for left hand middle finger swelling and pain of 1-year duration. Her medical history was relevant for 15 years history of progressive 4th and 5th fingers malformations that were attributed to “sarcoidosis,” and for which she was treated with anti-inflammatory and low dose steroids therapy. At our clinic, physical examination was consistent with a swelling of the base of the middle finger associated with tenderness and decreased range of motion. Radiographs of the hand showed a lytic lesion involving the distal half of the first phalanx, along with blurred limits of the bone surfaces involved. An magnetic resonance imaging was ordered and showed hyper-intense signal of the first phalanx, along with subcutaneous enclosed collections on both sides of the phalanx. Surgical debridement with open biopsy and culture was done. Pathology results showed caseating granulomas, and cultures confirmed the diagnosis of TD. A computed tomography scan of the chest was done postoperatively; where few calcified nodules were noted. She also received a 9-months course of anti-tuberculous drugs and had complete cure by 9 months postoperatively.
Conclusion: TD of the hand is a very rare entity of the spectrum of extrapulmonary M. tuberculosis infection. Clinicians should have a high index of suspicion concerning this pathology not to delay the diagnosis, which could lead to permanent deformity. Early diagnosis and treatment can significantly improve outcomes.
Keywords: Tuberculous dactylitis, finger deformity, bone cancer, hand infection.
Skeletal tuberculosis is a rare form of Mycobacterium tuberculosis infection representing 1–3% of all extrapulmonary tuberculosis. Of which, the spine is the most common skeletal site of involvement [1]. The hand is affected in only 1% of cases [1]. When tubular bones are affected (such as metacarpal bones and phalanges), the disease is given the name of tuberculous dactylitis (TD) [2]. The rarity of this condition and its subtle clinical course can delay the diagnosis and make resulting complications more severe. This challenge can affect the patient’s quality of life because neglected osteoarticular tuberculosis can lead to joint destruction and permanent malformation of the joints [2]. We present herein, a rare case of TD of the middle finger in a patient having a long history of misdiagnosed tuberculous infection that lead to permanent deformity of the neglected 4th and 5th fingers.
A 56-year-old female patient presented to our clinic for left hand middle finger edema and pain of 1-year duration. Her medical history was relevant for 15 years of progressive 4th and 5th fingers malformations that were attributed to sarcoidosis, and for which she was treated with anti-inflammatory and low dose steroids therapy; she stated that the malformation started in the form of pain and edema 15 years before achieving this neglected form. One year before presentation, the patient started noticing left middle finger edema and swelling associated with severe pain and a mass-like structure over the 1st phalanx. This was preceded by few days of weakness and fatigue. She sought medical advice at multiple clinics where the new mass was first diagnosed as bone cancer. At our clinic, physical examination was consistent with a swelling at the base of the middle finger (Fig. 1) associated with tenderness and decreased range of motion. Laboratory tests were within normal limits, except for elevated C-reactive protein, and erythrocyte sedimentation rate. Purified protein derivative test was negative. Radiographs of the hand showed a lytic lesion involving the distal half of the first phalanx, along with blurred limits of the bone surfaces involved (Fig. 2). An magnetic resonance imaging was ordered and showed hyper-intense signal of the first phalanx, along with subcutaneous enclosed collections on both sides of the phalanx (Fig. 3).
The decision was made for surgical debridement and biopsy. The patient was taken to the operating room, and using a dorsal approach to the middle finger, we identified two collections on both sides of the 1st phalanx; these collections were debrided and sent for culture.
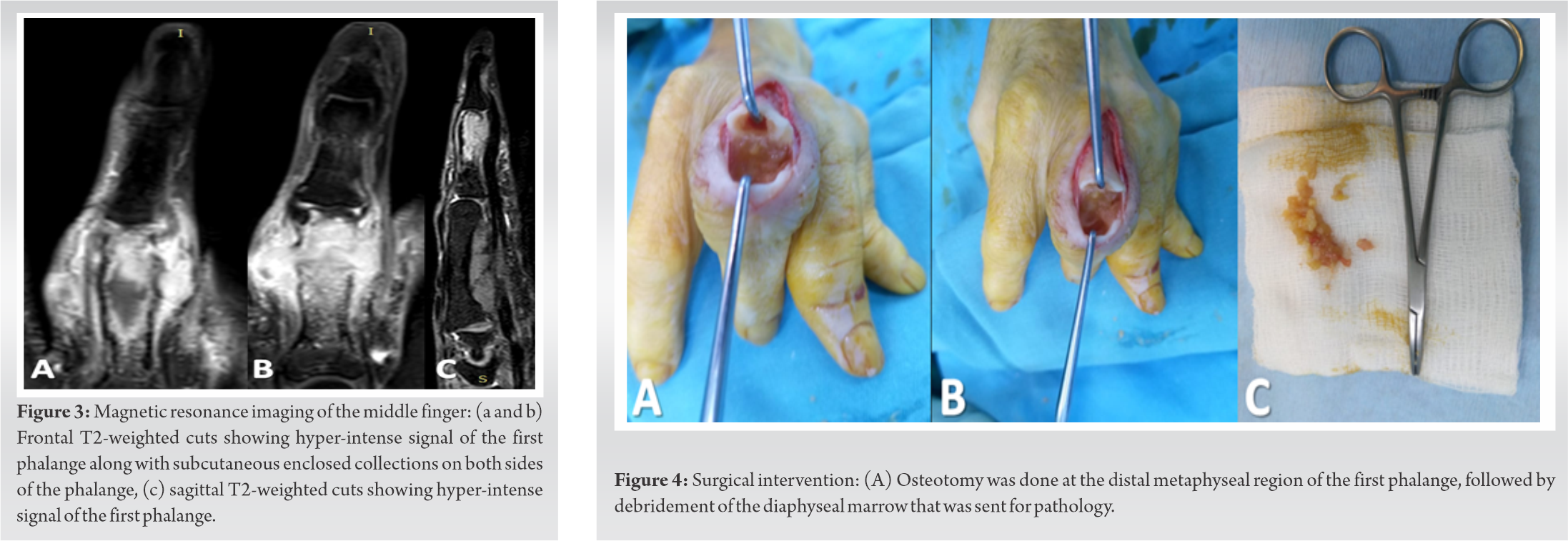
Then, an osteotomy was done at the distal metaphyseal region of the first phalanx, followed by debridement of the diaphyseal marrow (Fig. 4) that was sent for pathology. The osteotomy was reduced and fixed using 2 k-wires. Post-operative radiographs are shown in Fig. 5.
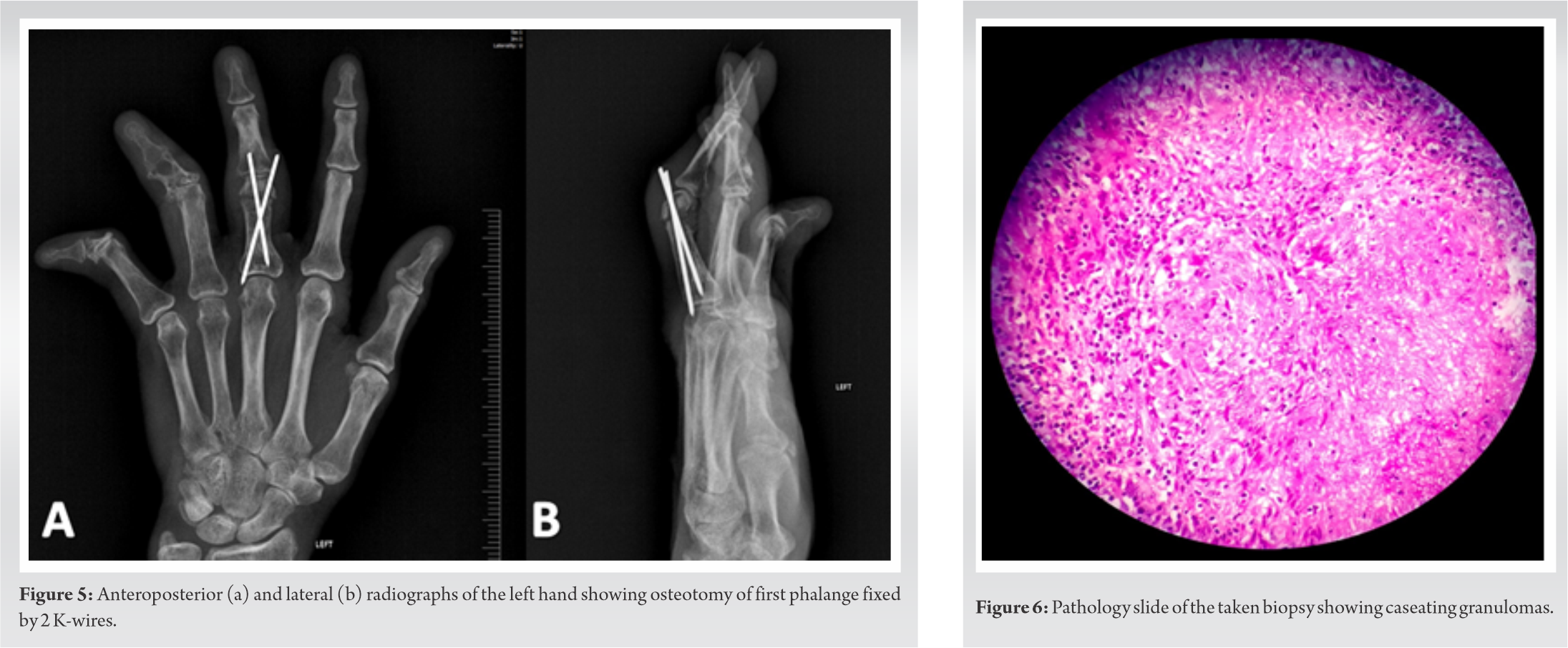
Pathology results showed caseating granulomas (Fig. 6), and culture confirmed the diagnosis of TD. A computed tomography scan of the chest was done postoperatively, where few calcified nodules suggestive of healed TB were noted (Fig. 7).
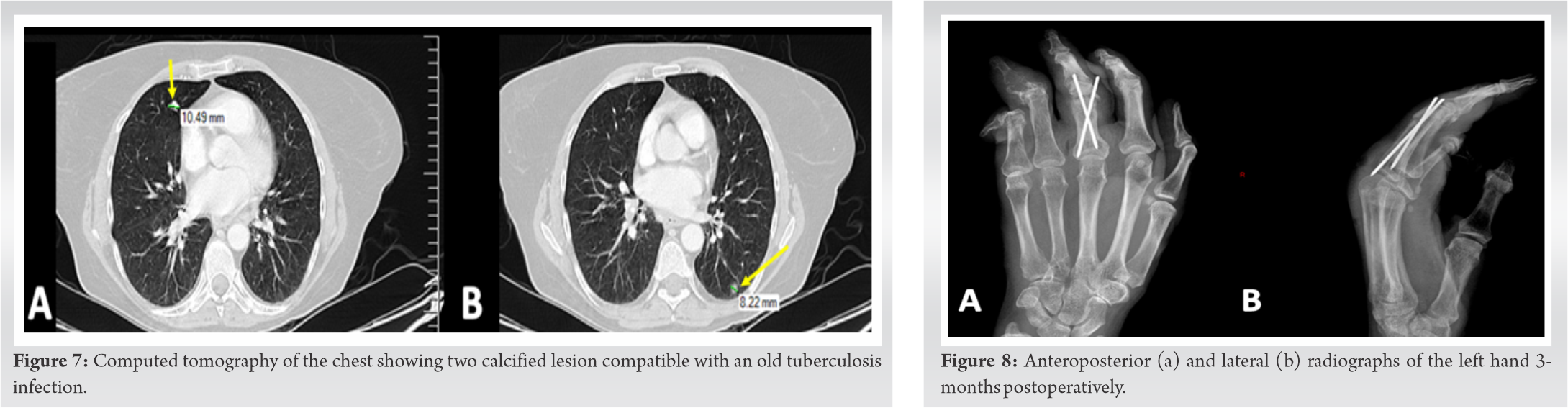
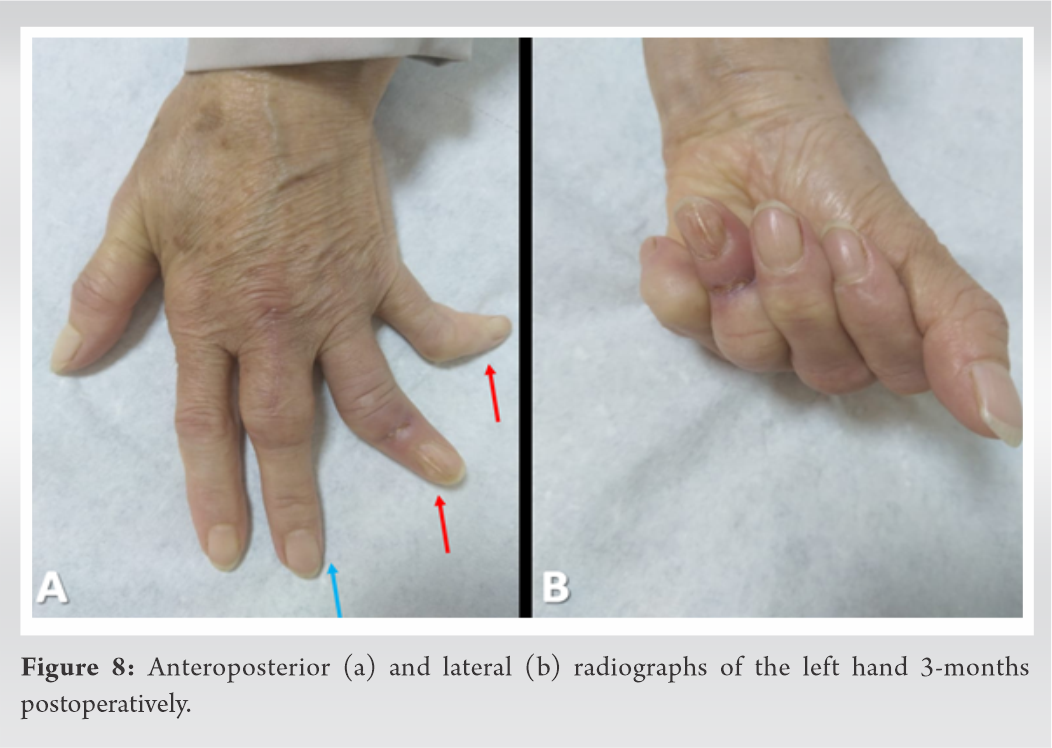
The patient had a complete union at 3 months postoperatively (Fig. 8), and the wires were removed. She also received a 9-months course of anti-tuberculous drugs. At 9-months follow-up, she was free of symptoms, finger swelling had decreased significantly, and she had full range of motion of the operated finger (Fig. 9).
TD is very uncommon. It only represents 1% of skeletal tuberculosis [2]. It is even more uncommon in adults, as it is typically a disease of patients less than 6 years old [3]. This rare presentation and the many pitfalls encountered during the workup of TD lead in most cases to a delay in the diagnosis by 9-12 months [3, 4]. This was the case in our patient where the diagnosis was delayed for up to 1 year since the last reactivation of the tuberculosis infection. Furthermore, our patient’s primary infection was misdiagnosed and she was treated for sarcoidosis for more than 10 years without significant improvement of the disease’s course at the level of her 4th and 5th finger. Tb dactylitis can resemble many pathologies both clinically and radiologically. Non-specific symptoms such as pain, swelling, and decreased range of motion are the most commonly reported. In addition, TB dactylitis can be present as a primary isolated lesion without any systemic symptoms or pulmonary manifestations of TB [5]. Radigraphically, a lytic lesion from bone destruction and sequestration is the most common presentation, which lead to naming this disease “Spina ventosa.” However, the differential diagnosis of a lytic lesion in the hand is very wide and includes primary bone tumors, pyogenic or fungal infections, syphilitic dactylitis, sarcoidosis, hemoglobinopathies, hyperparathyroidism, and leukemia [6]. Moreover, calcifications can evoke a chondroma, and a well demarcated lytic lesion surrounded by sclerosis can point to an osteoma. Absence of periosteal reaction is indicative of TB osteitis [4]. In laboratory investigations, a negative intradermal tuberculin reaction test or normal ESR levels do not exclude the diagnosis of TD. In fact, this has been reported in many cases in the literature [6, 7]. Isolation of Mycobacterium tuberculi in the culture with positive Ziehl-Neelsen staining for acid-fast bacilli remains the golden standard for accurate diagnosis. The role of surgery in the management of TD is obtaining an open biopsy for culture and histopathologic studies. Cultures may be negative as TD is a paucibacillary lesion [1]. Therefore, identifying the classic image of caseating granulomas surrounded by epithelioid histiocytes and multinucleated giant cells on pathology slides may aid greatly in diagnosing TD when cultures are negative, or confirm it when cultures are positive. Indeed, based on her radiographic studies suggestive of a tumor, negative intradermal tuberculin reaction test, and the absence of systemic or pulmonary TB symptomatology, our patient was first misdiagnosed with sarcoidosis of the 4th and 5th digit for a long period of time. She was then misdiagnosed with a primary bone tumor in the middle finger. Her workups in other facilities lacked an open biopsy, which could have led to devastating sequalae. The treatment is mainly non operative. It consists of a long course of anti-tubercular drugs. The initial phase includes a 2 months course of isoniazid, rifampin, pyrazinamide, and ethambutol followed by a 6-months regimen of isoniazid and rifampin [2, 8]. Good functional outcomes are generally reported following conservative treatment. Signs of remineralization, restoration of trabeculae, and decrease in osteoporosis found on radiography are indicative of a good response to antibiotherapy [4].
TD is a very rare presentation of musculoskeletal TB. It can mimic various other pathologies making the diagnosis very challenging. Orthopedic surgeons must keep vigilance for this condition when facing a lytic lesion of the metacarpals and phalanges, keeping in mind that it is not uncommon for TD to be present as a primary isolated lesion without a primary focus of infection being identified. Early diagnosis leads to favorable outcomes as TD responds very well to a long course of isoniazid, rifampin, pyrazinamide, and ethambutol, which can be evident both clinically and radiologically.
The diagnosis is based on the combination of several arguments: Clinical and radiological appearance, a positive intradermal tuberculin test, and laboratory investigations. In non-endemic regions, cultures positive of Mycobacterium tuberculosis and histopathology data remain mandatory.
References
- 1.Held MF, Hoppe S, Laubscher M, Mears S, Dix-Peek S, Zar HJ, et al. Epidemiology of musculoskeletal tuberculosis in an area with high disease prevalence. Asian Spine J 2017;11:405-11. [Google Scholar]
- 2.Fairag R, Hamdi A. Tuberculous dactylitis: Case presentation and functional outcome. J Orthop Case Rep 2016;6:22-4. [Google Scholar]
- 3.Sahli H, Roueched L, Sbai MA, Bachali A, Tekaya R. The epidemiology of tuberculous dactylitis: A case report and review of literature. Int J Mycobacteriol 2017;6:333-5. [Google Scholar]
- 4.Sbai MA, Benzarti S, Sahli H, Sbei F, Maalla R. Osteoarticular tuberculosis dactylitis: Four cases. Int J Mycobacteriol 2015;4:250-4. [Google Scholar]
- 5.Subasi M, Bukte Y, Kapukaya A, Gurkan F. Tuberculosis of the metacarpals and phalanges of the hand. Ann Plast Surg 2004;53:469-72. [Google Scholar]
- 6.Murphy MC, Murphy AN, Hughes H, McEneaney OJ, O’Keane C, Kavanagh E. Multimodal imaging of Spina Ventosa (TB Dactylitis) of the foot. Radiol Case Rep 2020;15:1373-6. [Google Scholar]
- 7.Martini M, Benkeddache Y, Medjani Y, Gottesman H. Tuberculosis of the upper limb joints. Int Orthop 1986;10:17-23. [Google Scholar]
- 8.Skoll PJ, Hudson DA. Tuberculosis of the upper extremity. Ann Plast Surg 1999;43:374-8. [Google Scholar]








