
Management strategy to be adopted for treating a neglected obturator variety of anterior hip dislocation should be based on the duration of neglect, ease of reduction and maintenance, and the subsequent needs of the patient with minimal operative interference to preserve what is natural with minimal complications.
Dr. Spandan R Koshire,
Department of Orthopaedics,
Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital,
Mumbai, Maharashtra, India.
E-mail: spndnkoshire11@gmail.com
Introduction: Among all the traumatic hip dislocations, anterior hip dislocation is a rarity in which the obturator inferior variety is one of the rarest to be documented [1]. Here we present to you the case of our patient, a 35-year-old male with a six month neglected obturator variety of anterior hip dislocation treated by salvage procedure of open reduction without the need for intertrochanteric osteotomy and resultant preserved natural hip for ambulation as an intermediary procedure.
Case Report: Mr. SH a 35-year-old male had a fall from 15 feet in his village and was treated by a local quack, Meanwhile the patient continued to experience pain and difficulty walking and after an ordeal of nearly 6 months during the lockdown period in coronavirus disease pandemic, showed up in our emergency room and was diagnosed with an obturator type anterior hip dislocation for which we carried out open reduction aided with Murphys skid through an anterolateral approach and stabilization using two Steinman pins and further immobilization by Thomas splint for a period of 15 days, which was done after confirmation of intact head vascularity under general anesthesia after which gradual mobilization was initiated. 3 months post operative, now patient is ambulatory with stick support with no deformity, no pain and with early radiological features of avascular necrosis (AVN) for which Total Hip Replacement (THR) is planned at a later date.
Conclusion: Utilisation of salvage procedures and moreover those with minimal operative complications will result in better, natural long-term intermediary measure outcome with a resultant delay in joint replacement procedure which is in the better interest of the patient.
Keywords: Anterior hip dislocation, open reduction, obturator inferior type, neglected dislocation, Anterolateral approach.
There has been a rising trend of hip dislocations but it is mostly posterior majorly due to road traffic accidents and fall from heights, whereas anterior dislocations constitute upto 18 percent in total among which obturator variety accounts for only 4% [2]. Historically a study by Thompson and Epstein documented 204 cases of dislocation out of which only 18 were anterior. Old unreduced anterior type dislocations are extremely rare and seen in acute settings of unavailable orthopedic help in rural areas [3]. In developing countries, it is common for patients to attend alternate therapy before turning up at the hospitals after many days of trauma. It becomes cumbersome to manage such cases as the time progresses. The fibrous tissue gets filled up in the acetabulum making closed reduction impossible [4]. Finding a suitable intermediary measure so as to suit the patients needs and ambulatory functions along with the provision of a more natural hip for later dated final measure joint replacement is of utmost importance. We report one such case which came to us after almost 6 months of neglect.
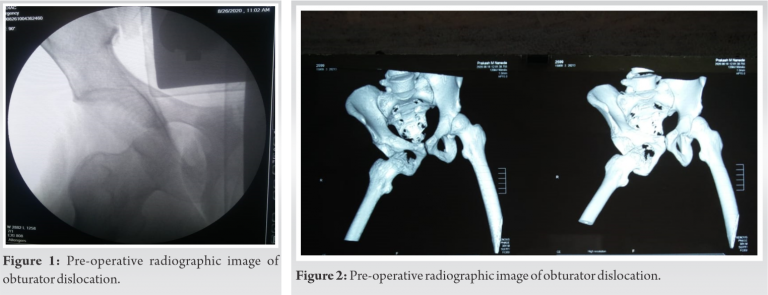
Mr. SH, A 35-year-old male patient presented to us with a history of fall from a height of 15 feet after which he was unable to bear weight on right lower limb. He was treated by a local quack in his village. He continued to experience pain for the next 6 months after which he presented to our emergency department with an antalgic gait. On clinical examination, he had a right lower limb abduction and external rotation deformity with painful restricted movements. Radiological imaging confirmed the clinical suspicion of anterior hip dislocation of obturator variety (Fig. 1, 2).
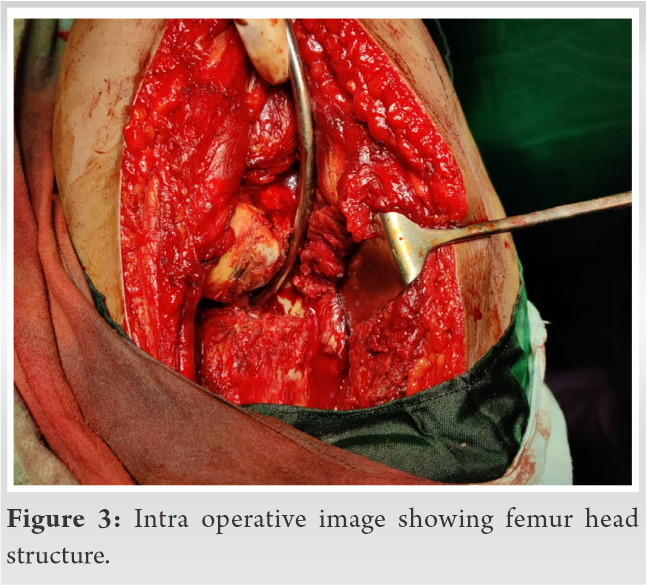
No associated fractures and intact distal neurovascular status were observed. An open reduction and internal fixation of the joint through an anterolateral approach was planned. After opening the hip joint, the head was visualized in the obturator foramen with findings of a dent and irregularity on the surface at the posterosuperior margin, absence of cartilage was noted, but intact vascularity confirmed by drill hole blood oozing (Fig. 3).
At this point reduction was successful with Murphy’s skid technique alone, post-reduction radiographs showed concentric and congruent reduction and stabilization achieved with two Steinman pins across the hip joint (Fig. 4).
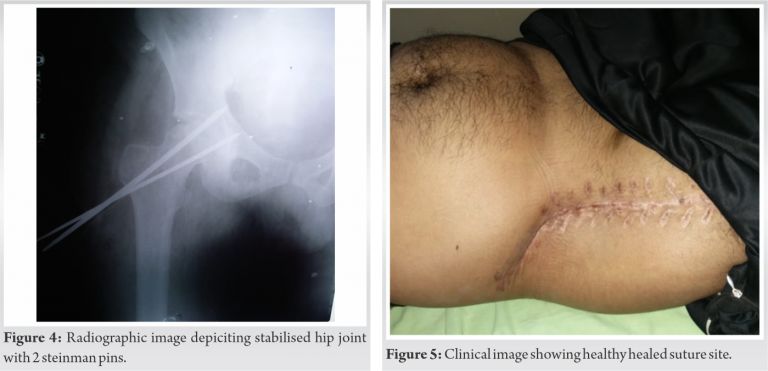
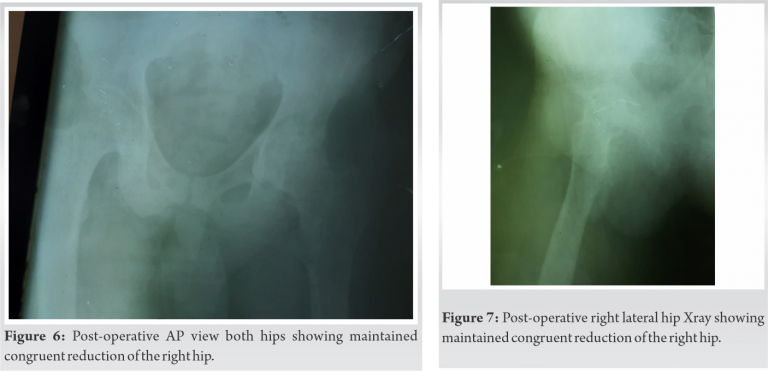
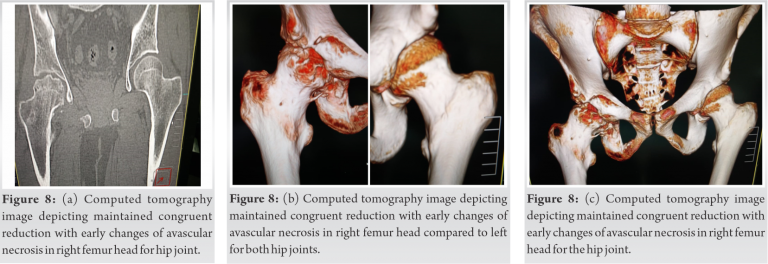
Steinman pins and sutures removed after 15 days, but the hip joint continued to be kept immobilized in Thomas Splint for 3 weeks postoperative after which gradual mobilization started (Fig. 5). Patient went discharge thereafter and returned back to his village but failed to follow-up at 6 weeks due to financial issues in addition to the restrictive travel conditions in the lockdown, now at 3 months postoperative the patient has painfree ambulation with stick support with early signs avascular necrosis (AVN) of the femoral head as seen on the X-ray and computed tomography scan (Fig. 6-8).
Patient has been planned for a total hip replacement (THR) at a later date as currently patient can ambulate to his satisfaction and there is no hindrance in his daily routine activities.
Old unreduced obturator variety of anterior hip dislocation is a rare entity. If the dislocation is identified early in the course it can be managed by closed reduction and immobilization alone with satisfactory results. In the case report by Kulambi et al. they were able to close reduce by Ali’s maneuver and maintain reduction of a rare anterior hip dislocation of obturator inferior type which came to their emergency within 2 h, whereas in our case the dislocation was neglected for a period of more than 5 months [1]. Gupta and Shravat (1977) utilized “heavy traction” with 10–18 kg skeletal traction and sedation of seven patients for around 20 days, and achieved reduction in 6 of the patients. The successful reductions were in patients with dislocations that were <3 months old [4]. If the neglect is more than 3 months old as which was in our case of around 6 months, the open reduction becomes a difficult option, and preferred treatment approaches mentioned in the literature include THR, modified girdle stone procedure by Nagi and trochanteric osteotomy [5, 6]. In a case report study by Young and Banza of a 4-month-old neglected anterior pubic dislocation the surgeons managed reduction with modified excision arthroplasty as recommended by Nagi et al. At follow-up approximately 3 months after surgery, the patient was using two crutches and had pain and instability of the hip when he tried to walk without support. The patient was lost to follow-up [4]. By opting for a less aggressive approach we were able to conserve the natural hip even though the disloation being 6 month old and making the patient ambulatory. In another study by Alva et al., they managed a case of 5-month-old unreduced anterior dislocation by performing girdle stone arthroplasty and at 3-year follow-up the patient had a “fairly stable hip” but with 2.5 cm shortening [7]. In our case, as we preserved the natural hip for the final outcome surgery of THR, we prevented the shortening and gait abnormality which occurs with girdle stone procedure and the patient was able to ambulate sufficiently without any gait challenges. Aggarwal and Singh (1967) reported an anterior pubic dislocation which was neglected for around 13 months and managed by arthroplasty. Shaving of articular cartilage of femoral head with covering of fascia lata and reduction into acetabulum was done but after 1 year of follow-up AVN was confirmed [8]. It is advocated that neglected anterior dislocations be better treated by THR so as to provide a stable hip, but as is our case we sought for an intermediary option of preservation until the time for established AVN so as to then proceed with THR at a later date. Intraoperative head viability assessment is an important determinant for treatment modality with nonviable head being better treated with excisional arthroplasty or THR and if otherwise, then open reduction can be attempted and is aided by trochanteric flip osteotomy [7, 8]. This view point is better supported by the case report study done by Young et al. in which they mention to follow Bernese trochanteric flip osteotomy as this preserves the blood supply to the head and allows removal of scar tissue with ample exposure of the acetabulum. The main short-term concern in cases of conservative management strategies as is in our case, in order to preserve the natural head is AVN development at a later stage [9]. In our case after confirmation of head viability reduction was done using Murphys skid technique instead of opting for trochanteric osteotomy with avoidance of resultant complications such as trochanteric bursitis, migration, and persistent localized trochanteric pain [10]. Thus, we were able to maintain the natural abductor function undisturbed. By preserving the head we gave the patient a chance to ambulate with a natural hip without perfoming unnecessary osteotomies and excisions. And when the AVN is established at a later date, it will be easier to proceed in this case with THR as minimal procedures would have been carried out on the hip planned for replacement. In a resource-poor setting when the patient is unable to bear the cost for the replacement at the initial sitting and is reluctant for replacing the joint, It becomes impossible to opt for replacement as a primary measure, our method of management will serve as an intermediary for the time being with quick recovery after the procedure with which the patient will be able to function naturally and with a stable hip and in a better suitable anatomical condition for THR at a later date as compared to traditional approaches as that of flip osteotomies or excisional arthroplasties.
In our case, with a 6-month-old neglected obturator variety of anterior hip dislocation we present a management strategy as an intermediary step for a definitive replacement during which the patient in a resource-poor setting will have a swift recovery and be able to naturally ambulate and function to earn his daily livelihood and earning. Moreover, achieving a stable reduction without the need for trochanteric osteotomy we thus persevered to preserve the already precarious blood supply to the head and provided with a natural hip for ambulation by avoiding girdle stone procedure. Even though with the setting in of early AVN changes, he will still have a better functioning and a more normal anatomical hip after our intermediary salvage procedure suitable for a later date THR or arthrodesis.
Management strategy to be adopted for treating a neglected obturator variety of anterior hip dislocation should be based on the duration of neglect, ease of reduction and maintenance, and the subsequent needs of the patient. It is always better to opt for salvage procedures with minimal operative interference to preserve what is natural for better long-term outcomes with minimal complications so as to aid further operative interventions if required at a later date.
References
- 1.Kulambi V, Chaudhari K, Pethapara V. Anterior hip dislocation in young patient obturator (inferior) type: A rare case report. Int J Res Orthop 2018;4:523-6. [Google Scholar]
- 2.Hani R, Kharmaz M, Berrada MS. Traumatic obturator dislocation of the hip joint: A case report and review of the literature. Pan Afr Med J 2015;21:55. [Google Scholar]
- 3.Dawson I, van Rijn AB. Traumatic anterior dislocation of the hip. Arch Orthop Trauma Surg 1989;108:55-7. [Google Scholar]
- 4.Young S, Banza L. Neglected traumatic anterior dislocation of the hip. Open reduction using the Bernese trochanter flip approach-a case report. Acta Orthop 2017;88:348-50. [Google Scholar]
- 5.Mirovsky Y, Fischer S, Hendel D, Halperin N. Traumatic anterior dislocation of the hip joint with fracture of the acetabulum: A case report. J Trauma 1988;28:1597-9. [Google Scholar]
- 6.Kumar S, Dahuja A, Narula MS, Garg S, Kaur R. Neglected hip dislocation: An unusual presentation, its management and review of the literature. Strategies Trauma Limb Reconstr 2017;12:189-92. [Google Scholar]
- 7.Alva A, Shetty M, Kumar V. Old unreduced traumatic anterior dislocation of the hip. BMJ Case Rep 2013;2013:bcr2012008068. [Google Scholar]
- 8.Sultan A, Dar TA, Wani MI, Wani MM, Shafi S. Bilateral simultaneous anterior obturator dislocation of the hip by an unusual mechanism-a case report. Ulus Travma Acil Cerrahi Derg 2012;18:455-7. [Google Scholar]
- 9.Aprato A, Baroni C, Massè A. Should trochanteric osteotomy be always avoided during safe hip dislocation? Ann Transl Med 2016;4 Suppl 1:S36. [Google Scholar]
- 10.Nagi ON, Dhillon MS, Gill SS. Chronically unreduced traumatic anterior dislocation of the hip: A report of four cases. J Orthop Trauma 1992;6:433-6. [Google Scholar]





