If a fracture of CoC bearing couple in THA is suspected in an asymptomatic patient, a CT scan should be performed as soon as possible and the failed bearing should be replaced with CoC or CoP and not to MoP, because of the risk for metallosis and further revision operations.
Dr. Matevž Topolovec,
Department of Physical and Organic Chemistry, Jožef Stefan Institute, Jamova 39, 1000 Ljubljana, Slovenia.
E-mail: matevz.topolovec@ob-valdoltra.si
Introduction: Revisions due to the fracture of ceramic-on-ceramic (CoC) bearing are rare, however when they occur, they represent a major challenge to an orthopedic surgeon for ensuring safe and long-term survival of the replaced bearing.
Case Report: We present a case of fractured ceramic liner of total hip prosthesis that underwent revision to a metal-on-polyethylene (MoP) bearing couple, with consequent huge periprosthetic metallosis. Shortly after, the second revision operation followed using the third bearing couple of ceramic-on-polyethylene (CoP). At 10 years follow-up after the operation due to ceramic fracture, the patient is now pain free with full range of motion of the revised hip.
Conclusion: Establishment of diagnostic routes and recommended protocols for CoC bearing fracture would allow easier recognition of potential fracture and diminish its consequences for the patients.
Keywords: Tribology, Revision Hip Arthroplasty, Ceramic Bearing Fracture.
Alumina ceramic-on-ceramic (CoC) bearing couple has been introduced in the 1970s as an alternative for younger and more active patients, based on the lower wear rates [1, 2]. Unfortunately, the favorable wear properties of CoC have been largely suppressed by the brittleness of the material, which resulted in occasional fractures of the bearing couple [3]. Despite the fact that the fracture rate of the fourth-generation (Biolox delta®) ceramic significantly decreased compared with the third generation ceramic [4], the fear how to cope with the revision operation for ensuring the long-term survival of a new bearing couple remains.
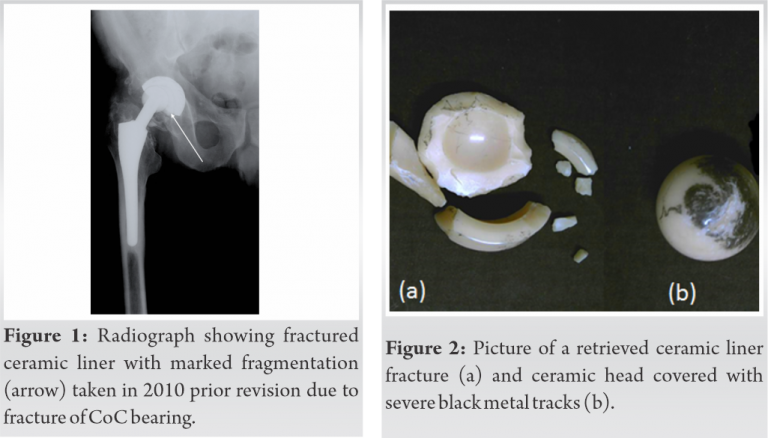
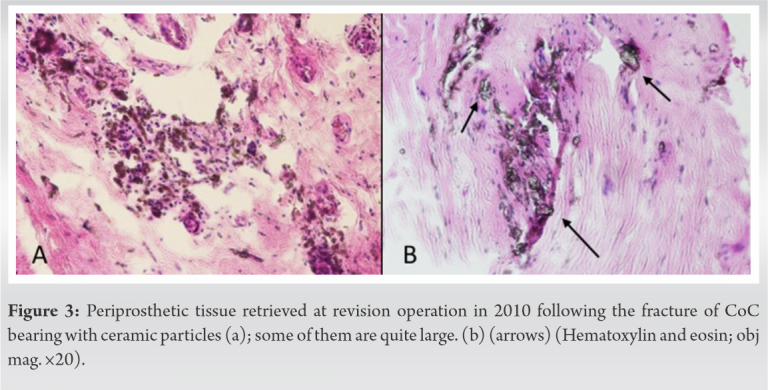
In December 1999, a 50-year-old man with post-traumatic painful right hip arthrosis underwent a cementless total hip arthroplasty with a third generation alumina CoC bearing couple (Biolox Forte®). The implants used were Cremascoli Ortho with ANCA-FIT acetabular cup and ANCA-FIT modular femoral stem. The patient had good clinical results until March 2007, when he experienced little pain and crepitus noise. After 3 months, the operating surgeon examined him. The hip was pain free with full range of motion; however, a radiograph indicated some small calcinations which could also represent fractured ceramic particles. A hip arthrography excluded aseptic loosening or an infection. However, after 3 years since the patient experienced the first symptoms in 2007, he was in October 2010 presented with more pain, more crepitus noises and limited hip motion, all characteristics of ceramic fracture. A radiographic image taken (Fig. 1) now clearly revealed a ceramic liner fracture (Fig. 2a). The ceramic head was not fractured but covered with severe black metal tracks (Fig. 2b); these originated from the action of sharp ceramic debris against metal parts of the implant. Metal particles thus formed became embedded within the articulating surface of the fractured CoC bearing. The patient underwent revision surgery in November 2010. A direct lateral approach true the primary scar was used. The ceramic fragments were removed, a polyethylene liner was inserted and the ceramic head was replaced with a CoCr femoral head. Therefore, metal-on-polyethylene (MoP) bearing was introduced. An extensive synovectomy was done. Only manual tissue rinsing was done, because of the absence of pulsatile lavage system. Periprosthetic tissue samples were sent for histological analysis, where numerous ceramic particles, some even quite large, were found (Fig. 3). After revision, the patient fully recovered without any pain and discomfort in the hip.
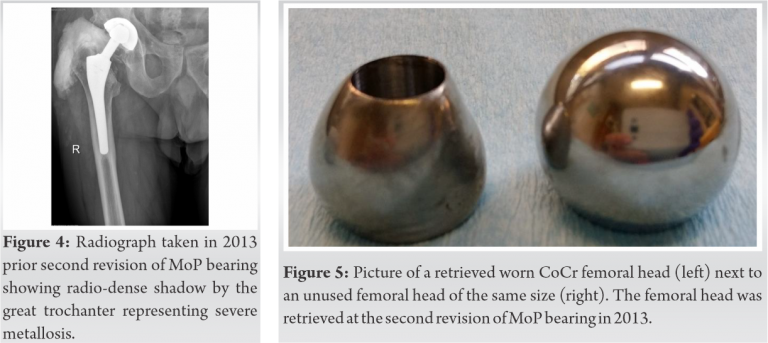
At a regularly post-operative check-up about 3 years later (July 2013) a radiograph revealed a worn metal head with a radio-dense shadow by the great trochanter (Fig. 4).
The patient underwent a second revision in October 2013. The same operative approach and skin scar were used as in the first two operations. The black-stained pseudocapsule was removed together with the black periprosthetic tissue. There was an obvious infiltration of the muscles with metallosis; however, no clear necrotic sections were seen, so an extensive necrectomy was not necessary. The worn CoCr femoral head (Fig. 5) was replaced with a 4th-generation ceramic head (Biolox delta) with titanium sleeve. Furthermore, we removed the acetabular cup, although well fixed, and replaced it for a cemented Durasul cup with a cross-linked polyethylene liner.
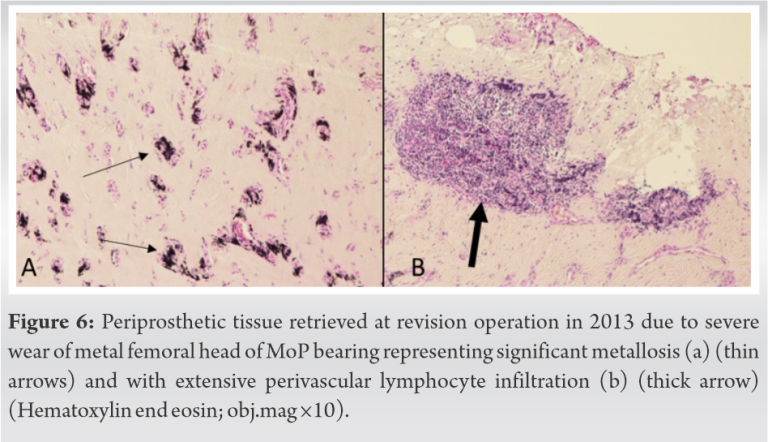
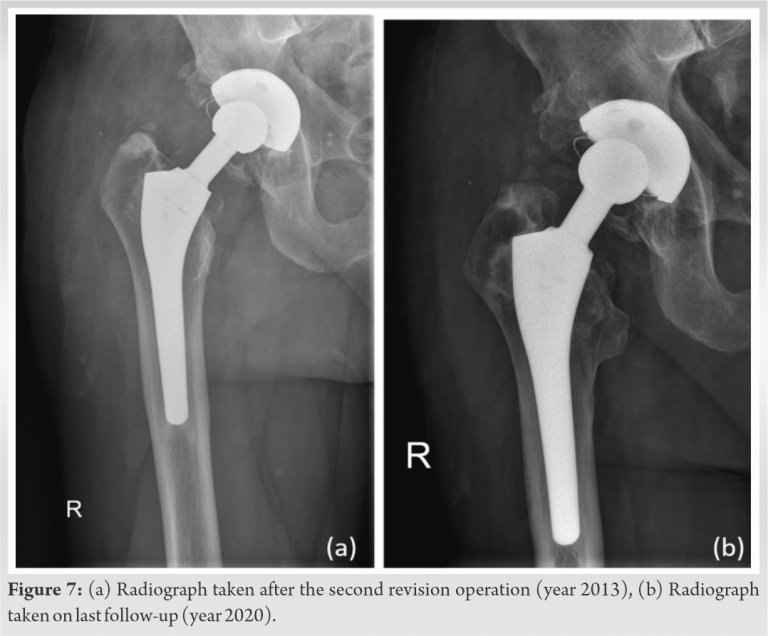
The femoral component was also well fixed and the femoral taper was intact so we decided to leave it in. Periprosthetic tissue samples were once again sent for histological investigation with slides now demonstrating significant metallosis with lymphocyte infiltration (Fig. 6). At approximately 10 years after the first and 7 years after the second revision operation the patient is doing fine and fully returned to normal daily activities. A control radiograph (Fig. 7a) taken just after the second revision and a follow-up radiograph (Fig. 7b) taken in July 2020 revealed no osteolytic changes or evidence of complication. Harris hip score [1, 2] for the patients on a last control was 73.
Fracture of a ceramic component in CoC bearing couple can represent a major problem for long-term outcomes after revision of THA [3, 4, 5]. The first problem is the prompt diagnostics of a ceramic fracture component. Namely, we know that a non-displaced ceramic linear fracture can be asymptomatic [6]. In our case, it took more than 3 years (first symptoms March 2007, confirmed ceramic fracture November 2010) to reach an obvious clinical and radiological presentation. In the meantime, consequences of a long delay can lead to material deterioration and extensive destruction of bone and tissues [4] and can cause pelvic discontinuity [7]. On this basis, if suspicion of a ceramic bearing is suggested, computed tomography rather than plain radiographs should be used [8], because small fragments can be mistaken for a heterotopic ossification [9]. In our case, no CT diagnostic or component alignment radiographic studies were done. This would surly helped in the rapid diagnosis of our asymptomatic patient (3 years before the severe symptoms accrued) and the revision operation would be much easier, especially in the regard struggling of removing all ceramic particles and debris. CT imaging was also not done before the second revision operation because of fear of stale image due to huge metallosis.
The second problem represents the dilemma for choosing the appropriate bearing couple following the ceramic fracture. Although the debate for the most appropriate revision bearing couple is still going on [10, 11], more and more studies [5, 8, 11] suggest that the revision bearing couple should be CoC or ceramic-on-polyethylene (CoP), specifically because of the risk of third-body wear. Since revision of fractured CoC bearing for a MoP bearing may pose a potential high risk for metallosis and further cobalt toxicity it should be avoided. Despite the huge metallosis observed on X-ray image (Fig. 3) and the presence of metallic particles in histological periprosthetic tissue sections (Fig. 5), our patient did not experience any symptoms of systemic cobalt toxicity [12] leading to heavy consequences like heart failure. On the other hand, laboratory tests to determine the chromium and cobalt levels are not part of a routine clinical practice but this case indicates that their introduction should be taken into consideration to allow earlier alert. However, regular radiological and clinical follows-ups are now mandatory for this patient, because of a higher risk for aseptic loosening due to huge particle loads from two former bearing couples with two distinctive failure mechanisms – ceramic fracture and heavy metallosis.
Given that the decision of choice of a revision bearing couple after fracture of ceramic component is still at the discretion of the surgeon, this case-report emphasizes the need for establishment of diagnostic routes and recommended protocols, which would allow easier recognition of potential fracture and diminish its consequences.
Prompt diagnostic and quick revision operation of a non-displaced CoC bearing couple, together with the right choice of the revision bearing can deprive the patient of much suffering.
References
- 1.Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am 1969;51:737-55. [Google Scholar]
- 2.Shields RK, Enloe LJ, Evans RE, Smith KB, Steckel SD. Reliability, validity, and responsiveness of functional tests in patients with total joint replacement. Phys Ther 1995;75:169-76. [Google Scholar]
- 3.D’Antonio JA, Capello WN, Naughton M. Ceramic bearings for total hip arthroplasty have high survivorship at 10 years. Clin Orthop Relat Res 2012;470:373-81. [Google Scholar]
- 4.Hannouche D, Zaoui A, Zadegan F, Sedel L, Nizard R. Thirty years of experience with alumina-on-alumina bearings in total hip arthroplasty. Int Orthop 2011;35:207-13. [Google Scholar]
- 5.Trebše R, Mihelič A, Levašič V, Cör A, Milošev I. Results of revision of total hip arthroplasty for alumina ceramic-on-ceramic bearing fracture. Hip Int 2016;26:237-43. [Google Scholar]
- 6.Toni A, Traina F, Stea S, Sudanese A, Visentin M, Bordini B, et al. Early diagnosis of ceramic liner fracture. Guidelines based on a twelve-year clinical experience. J Bone Joint Surg Am 2006;88:55-63. [Google Scholar]
- 7.Winston BA, Kagan RP, Huff TW. Delayed diagnosis of catastrophic ceramic liner failure with resultant pelvic discontinuity and massive metallosis. Arthroplast Today 2017;3:77-82. [Google Scholar]
- 8.Traina F, Tassinari E, De Fine M, Bordini B, Toni A. Revision of ceramic hip replacements for fracture of a ceramic component: AAOS exhibit selection. J Bone Joint Surg Am 2011;93:e147. [Google Scholar]
- 9.Rambani R, Kepecs DM, Mäkinen TJ, Safir OA, Gross AE, Kuzyk PR. Revision total hip arthroplasty for fractured ceramic bearings: A review of best practices for revision cases. J Arthroplasty 2017;32:1959-64. [Google Scholar]
- 10.Traina F, De Fine M, Di Martino A, Faldini C. Fracture of ceramic bearing surfaces following total hip replacement: A systematic review. Biomed Res Int 2013:157247. [Google Scholar]
- 11.Allain J, Roudot-Thoraval F, Delecrin J, Anract P, Migaud H, Goutallier D. Revision total hip arthroplasty performed after fracture of a ceramic femoral head. A multicenter survivorship study. J Bone Joint Surg Am 2003;85:825-30. [Google Scholar]
- 12.Dahms K, Sharkova Y, Heitland P, Pankuweit S, Schaefer JR. Cobalt intoxication diagnosed with the help of Dr. House. Lancet 2014;383:574. [Google Scholar]