
A high index of clinical suspicion and early detection can identify associated injury combination with tarsal navicular bone fracture.
Dr. Ankur Singh,
Rhythm Medical Center, A-321, Sector 47, Noida, Uttar Pradesh – 201 304, India. E-mail: ankursingh240984@gmail.com
Introduction: Fractures of tarsal navicular bone are a rare injury. A navicular fracture can occur either in isolation or associated with other bony or ligamentous injuries, depending on the severity and mechanism of trauma at the time of impact. We report a previously undescribed injury combination of navicular fracture with tear of the lateral ankle ligament complex.
Case Report: An 18-year-old professional long jump athlete presented with a history of twisting injury immediately before taking off, while attempting a jump. A detailed clinical examination and radiological assessment with computed tomography (CT) and magnetic resonance imaging (MRI) scan were performed. She was diagnosed to have a navicular body fracture with complete rupture of anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL). Acute fixation of navicular body fracture along with primary repair of ATFL and CFL was done. The final outcome of the patient was good with return to unrestricted physical activities after 4 months.
Conclusion: A new injury combination of navicular fracture along with lateral ankle ligament complex tear is reported in a professional athlete. A high index of clinical suspicion and early detection using CT and MRI scan can identify this rare injury combination. Surgical treatment can result in favorable outcomes.
Keywords: Tarsal navicular bone, fracture, anterior talofibular ligament, calcaneofibular ligament, computed tomography scan, magnetic resonance imaging scan.
Fracture of tarsal navicular bone is a rare injury [1] and its diagnosis can be delayed and often misdiagnosed as a mid-foot sprain. This injury often occurs by the same mechanism of plantar flexion with excessive inversion or eversion force, which also causes ankle sprains. A low index of suspicion often misses the diagnosis [2, 3]. The navicular bone is the keystone of medial longitudinal arch and bears majority of the load applied to the foot [4]. A navicular fracture can occur either in isolation or associated with other injuries, depending upon severity and mechanism of injury at the time of impact. The navicular has a complex vascular supply and delay in diagnosis may lead to long-term functional impairment [2]. There are numerous classification systems for navicular fractures [5, 6, 7]. A recent classification proposed by Petrie et al. is based upon the mechanism of injury and associated injuries [8]. It classifies this injury into five types, ranging from simple avulsions to severe bicolumnar injuries. Associated lateral column injuries in their series were reported in 87 out of 285 enrolled patients, with a combined frequency of 31%. Most common mechanism of injury causing combined navicular and lateral column injuries was axial loading along with either forefoot abduction/adduction or mid-foot extension [8]. We report a case of tarsal navicular bone fracture with lateral ankle ligament complex injury in a professional long jump athlete. The aim of this case report is to highlight the occurrence of this injury pattern and importance of timely detection of such injuries with the use of three-dimensional (3D) reconstruction of computed tomography (CT) and magnetic resonance imaging (MRI) scans to evaluate complete nature of injury and formulate its treatment plan.
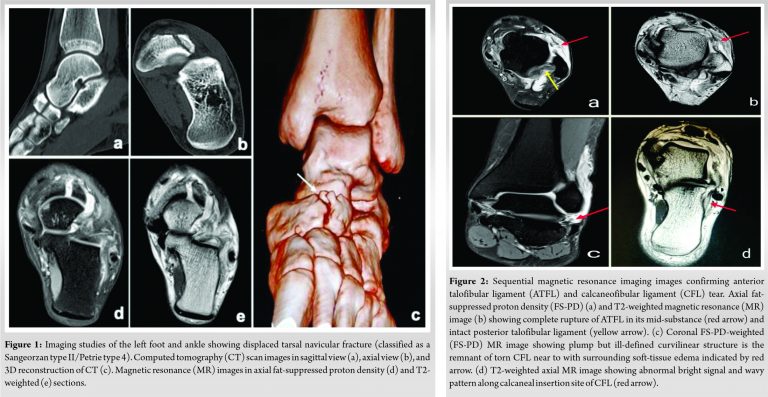
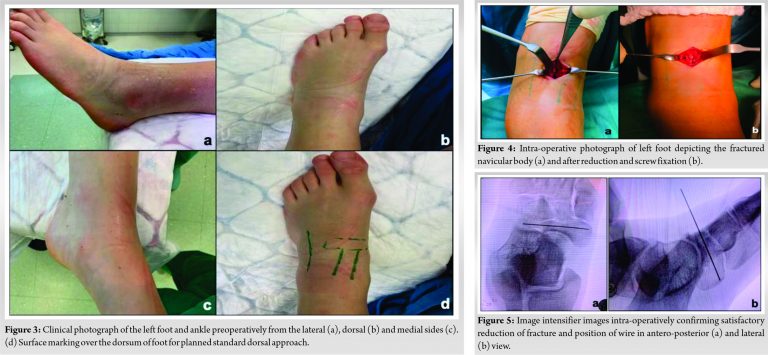
An 18-year-old female, professional long jump athlete with no prior relevant medical history, presented to our emergency department after sustaining a twisting injury to her ankle. The injury occurred just before taking off while attempting a long jump. She complained of pain and swelling in her right ankle and foot and was unable to bear weight on the affected limb. There was prominent soft-tissue edema over the lateral aspect foot with point tenderness along the mid-foot and lateral aspect of ankle, just below lateral malleolus. The neurovascular examination showed that no impairment and compartment syndrome was were excluded. Plain radiographs of foot and ankle in anteroposterior, lateral, and Myerson 30o medial oblique views were obtained [9]. The radiographs showed a displaced tarsal navicular fracture with loss of height of the medial arch and shortening of the medial column of the foot (classified as a Sangeorzan type II/Petrie type 4) [6, 8]. There was no other bony injury as confirmed by multiaxial and 3D reconstruction of CT imaging. A non-contrast 3T MRI scan confirmed the displaced navicular fracture along with complete tear of anterior talofibular ligament (ATFL) at its mid substance and calcaneofibular ligament (CFL) near its calcaneum attachment site (Fig.1, 2).
The patient was counseled about the need for surgical treatment. She was scheduled for the navicular fracture fixation and concomitant ligament repair within 24 h of sustaining the injury. The surgery was performed under general anesthesia. The patient was placed in the supine position and a thigh tourniquet was applied (Fig. 3). The navicular fracture was approached through standard dorsal approach between the tibialis anterior and extensor hallucis longus tendons. The neurovascular bundle was identified and retracted laterally. Overlying joint capsule was found to be disrupted, and careful deeper dissection was done to preserve as much periosteum as possible. Primary reduction was achieved by direct manipulation and stabilized temporarily with a 1.5 mm Kirschner wire under fluoroscopy guidance. Satisfactory reduction of fracture and position of wire were confirmed, and definitive fixation was done with a 2.5-mm headless compression screw (Fig. 4, 5).
The lateral ankle ligaments were approached through a standard lateral approach, taking care to protect the sural and superficial peroneal nerves. Careful deeper dissection was done to identify the inferior extensor retinaculum and it was separated from underlying talocrural capsule, which was found to be disrupted. The torn ends of ATFL were found at its mid substance and CFL near its calcaneum attachment site. Primary end-to-end repair of ATFL was done using No. 0 Vicryl suture in a modified Bunnell fashion. The calcaneum attachment site of CFL was identified, and a 1.4-mm Jugger Knot Soft Anchor (Biomet Inc., Warsaw, IN, USA) was inserted after preparation of bone bed and each suture limb passed through the torn ends of ligament to repair the ligament. Repair of ATFL and CFL was performed keeping the ankle and foot in neutral position. Sutures from the anchor were also used for concomitant tightening of joint capsule (Fig. 6).
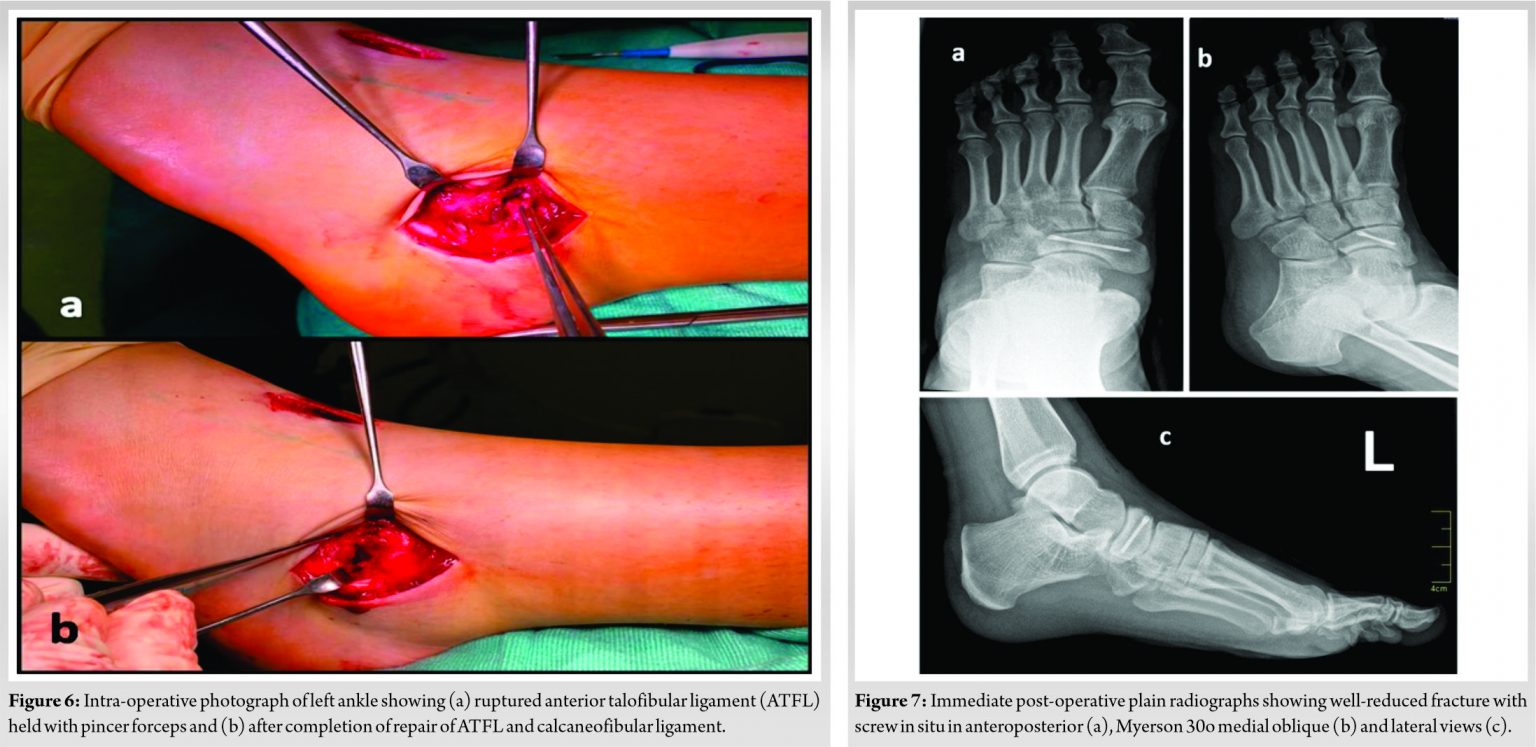
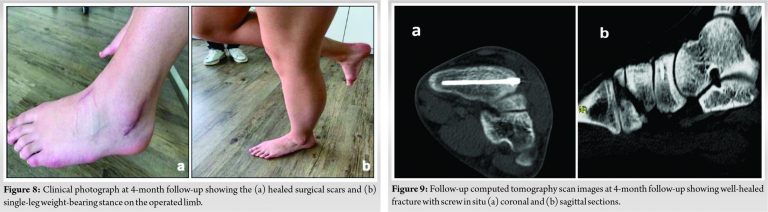
Post-operatively, the patient was kept in an ankle immobilizer for 8 weeks. Gradual weight bearing as per tolerance was allowed after 3 weeks and full weight bearing allowed at 6 weeks. Post-operative radiographs were obtained immediately following surgery and at 6 and 16 weeks after surgery (Fig. 7). CT scan to assess fracture healing was done at 6- and 16-week interval. Sequential clinical and radiological assessment showed fracture union with the American Orthopedic Foot and Ankle Score (88/100 points) at 16 weeks follow-up (Fig. 8, 9). The patient was satisfied with the final outcome with complaints of mild pain occasionally. She was allowed to resume her physical activity including running and jumping without any restrictions after 4 months.
In 1989, Sangeorzan et al. classified fractures of the navicular into tuberosity, capsular avulsion, stress, and body fractures. Sub-classification of body fractures was done into three types based on direction of fracture line, direction of displacement of forefoot and mid-foot, and associated joint disruption [6]. Petrie et al. proposed their classification in 2018 based on the mechanism of injury and due consideration was given to associated injuries along the mid-foot region, including lateral column avulsion and crush injuries. These fractures were broadly classified into avulsion, tuberosity, Lisfranc variant, body, and fractures of navicular along with lateral column injuries. Lateral column injuries were subclassified into crush, avulsion, and crush injuries of both medial and lateral column [8]. Due to the rare occurrence of navicular fractures, most classification systems have primarily focused on the configuration of navicular fractures, and much less emphasis was given to the associated injuries along the mid-foot, hind-foot, and ankle region. The classification system proposed by Petrie et al. was the first to consider associated lateral column injuries and Lisfranc variant [8]. Clinical presentation of a navicular fracture can vary depending upon the extent of primary impact, such as low energy due to simple twisting force or high energy seen in sports injuries, fall from height, or motor vehicle collision. Extent of associated injuries in the mid-foot region was found in 87 of 285 patients in Petrie’s series and in 15 of 24 patients in Evans’s series [8, 10]. Initial evaluation of these fractures must include a full series of foot and ankle radiographs and CT scan with 3D reconstruction and suppression of the talus and the calcaneus to identify lateral plantar fragment attached to plantar calcaneonavicular ligament highlighted by Cronier et al. [11]. The use of MRI imaging protocol is not standardized for acute foot and ankle injuries, and more emphasis has been laid on offering a scan in case of persistent symptoms or vague chronic presentation as in navicular stress injuries [12]. This report highlights the advantage of MRI scan in an acute situation which detected an associated ATFL and CFL ligament complex injury. This provided objective evidence of the presence and severity of this injury which allowed concomitant repair of ligaments along with fracture fixation. The management of navicular fractures depends largely on the fracture pattern. The aim is to restore the articular congruity of talonavicular and naviculocuneiform joints and to address associated injuries simultaneously. Surgical management is often necessary in high-energy injuries causing displaced navicular body fractures and displaced tuberosity fractures. Recommended indications for surgery include joint incongruity of >1 mm, shortening of the medial column by >2–3 mm, open fracture, compromised soft tissue condition, and complications such as compartment syndrome [13]. Fixation options for navicular fracture depend upon the extent of comminution and associated lateral column injuries. These include lag screw fixation for two-part body fractures or locking plates, mini plates, and external fixator application with supplementary K wire fixation for comminuted fractures [13]. A headless compression screw fixation was used in our patient and that achieved adequate stability to the fracture. ATFL injuries were reported in 75% of patients after acute inversion ankle sprain with a combined ATFL and CFL injuries in 41% of patients in a retrospective MRI study done by Khor et al on 64 patients. Isolated lateral ligament injury was found in 22% patients with 53% having concomitant pathologies. Bone bruising was seen in 50% of patients and 22% had associated fractures, of which navicular fracture was reported in only one patient. An avulsion fracture of the lateral malleolus was the most common site of occult fracture [12]. The treatment of acute injuries of the lateral ligaments of the ankle injury is still controversial. Some advocate early surgical repair using suture anchors for the treatment of high-grade injuries to prevent chronic ankle instability and achieve better functional outcomes, especially in high-demand patients [14, 15]. Kerkhoffs et al. reviewed 2562 cases from 20 randomized or quasi-randomized controlled trials comparing surgical with conservative interventions for treating ankle sprains in adults. Their results were in favor of surgical intervention with the outcome parameters being return to previous sporting activity, recurrence, residual pain, objective and functional instability, and swelling [15].
A new injury combination of navicular fracture along with lateral ankle ligament complex tear is reported in a professional athlete. A high index of clinical suspicion and early detection and evaluation using CT and MRI scan can identify this rare injury combination. Surgical treatment for fixation of the navicular fracture and primary repair of torn ankle ligaments can result in favorable outcomes.
Fracture of the navicular bone is a rare injury and its clinical presentation can vary depending upon the extent of primary injury and its mechanism. A high index of suspicion for associated injuries while analyzing this fracture and advanced imaging may help prevent missed diagnosis. Surgical treatment especially in high-demand patients can aid them to return to pre-injury state rapidly.
References
- 1.Schildhauer TA, Coulibaly MO, Hoffmann MF. Fractures and dislocations of the midfoot and forefoot. In: Court-Brown C, Heckman JD, McKee M, McQueen MM, Ricci W, Tornetta P 3rd, editors. Rockwood and Green’s Fractures in Adults. 8th ed. Philadelphia, PA: Wolters Kluwer; 2015. p. 2689. [Google Scholar]
- 2.Eichenholtz SN, Levine DB. Fractures of the tarsal navicular bone. Clin Orthop Relat Res 1964;34:142-57. [Google Scholar]
- 3.Freed HA, Shields NN. Most frequently overlooked radiographically apparent fractures in a teaching hospital emergency department. Ann Emerg Med 1984;13:900-4. [Google Scholar]
- 4.Sarrafian SK. Functional characteristics of the foot and plantar aponeurosis under tibiotalar loading. Foot Ankle 1987;8:4-18. [Google Scholar]
- 5.Main, B, Jowett, RL. Injuries of the midtarsal joint. J Bone Joint Surg Br 1975;57:89-97. [Google Scholar]
- 6.Sangeorzan, BJ, Benirschke, SK, Mosca, V, Mayo, KA, Hansen, ST. Displaced intraarticular fractures of the tarsal navicular. J Bone Joint Surg Am 1989;71:1504-10. [Google Scholar]
- 7.Fracture and dislocation compendium. Orthopaedic Trauma Association Committee for Coding and Classification. J Orthop Trauma 1996;10 Suppl 1:5-9, 1-154. [Google Scholar]
- 8.Petrie MJ, Blakey CM, Chadwick C, Davies HG, Blundell CM, Davies MB. A new and reliable classification system for fractures of the navicular and associated injuries to the midfoot. Bone Joint J 2018;100-B:176-82. [Google Scholar]
- 9.Myerson M. Foot and Ankle Disorders. Philadelphia, PA: Saunders; 2000. [Google Scholar]
- 10.Evans J, Beingessner DM, Agel J, Benirschke SK. Minifragment plate fixation of high-energy navicular body fractures. Foot Ankle Int 2011;32:485-92. [Google Scholar]
- 11.Cronier P, Frin JM, Steiger V, Bigorre N, Talha A. Internal fixation of complex fractures of the tarsal navicular with locking plates. A report of 10 cases. OrthopTraumatol Surg Res 2013;99 Suppl 4:S241-9. [Google Scholar]
- 12.Khor YP, Tan KJ. The anatomic pattern of injuries in acute inversion ankle sprains: A magnetic resonance imaging study. Orthop J Sports Med. 2013 Dec 20;1(7);1: [Google Scholar]
- 13.DiGiovanni CW. Fractures of the navicular. Foot Ankle Clin 2004;9:25-63. [Google Scholar]
- 14.Liu XF, Fang Y, Cao ZH, Li GF, Yang GQ. Repair of acute injuries of the lateral ligament complex of the ankle by suture anchors. Int J Clin Exp Med 2015;8:21796-801. [Google Scholar]
- 15.Kerkhoffs GM, Handoll HH, de Bie R, Rowe BH, Struijs PA. Surgical versus conservative treatment for acute injuries of the lateral ligament complex of the ankle in adults. Cochrane Database Syst Rev 2007;2:CD000380. [Google Scholar]





