
Technical consideration of hardware placement is of utmost importance for the outcome of reverse shoulder replacement.
Dr. Yogesh Soni,
Department of Orthopaedics, Fortis Hospital, Mohali, Punjab, India.
E-mail: yogesh1989.1989@rediffmail.com
Introduction: Reverse shoulder replacement (RSR) has been accepted as the treatment of choice for glenohumeral arthritis with irreparable rotator cuff tear. Dislocation has been a potential complication of RSR but glenosphere disengagement is a rare complication itself. There have been only few published reports of this complication in the literature.
Case Report: In this case report, we have presented a case of repeated disengagement of glenoid sphere post-RSR in a 72-year-old male retired army personnel operated with Zimmer Biomet comprehensive RSR design.
Conclusion: In our case scenario, we postulate that soft-tissue interposition was the reason for disengagement during first episode and was successfully relocated after removal. However, the subsequent disengagement was due to improper seating of sphere due to large central screw. Revision to a smaller central screw size appears to be the definitive solution in such case.
Keywords: Reverse shoulder replacement, glenosphere disengagement, glenohumeral arthritis, irreparable rotator cuff tear.
Reverse shoulder replacement (RSR) is accepted as the best treatment option for glenohumeral arthritis associated with an irreparable tear of the rotator cuff. Its indications and use have expanded in recent years fuelled by better outcome studies. With the increase in total number of shoulder replacements being performed nowadays, an increase in complication rates have been noted significantly.
The incidence of glenohumeral dislocation after RSR has been reported to range from 2.4% to 31% [1, 2, 3] but disengagement of the glenoid sphere is a very rare event reported in literature with incidence of 3%–5% [4, 5, 6]. Factors affecting the degree of stability are the soft-tissue balance, glenoid component inclination and coupling, and the version of the humeral component. Common factors associated with higher dislocation rates include body mass index >30, males, subscapularis deficiency, previous surgery, surgical approach, bone deficiency, and previous trauma. Soft-tissue tension, glenosphere diameter, humeral socket constraint, center of rotation (COR) offset, mechanical impingement, bony deficiency, erroneous version, and axillary nerve dysfunction should all be evaluated in patients with a dislocating prosthesis [4, 5]. Newer prosthesis has semi-constrained design which reduces these complications by a significant rate.
We present a case of repeated glenosphere dissociation mimicking instability in the immediate post-operative setting of a RSR.
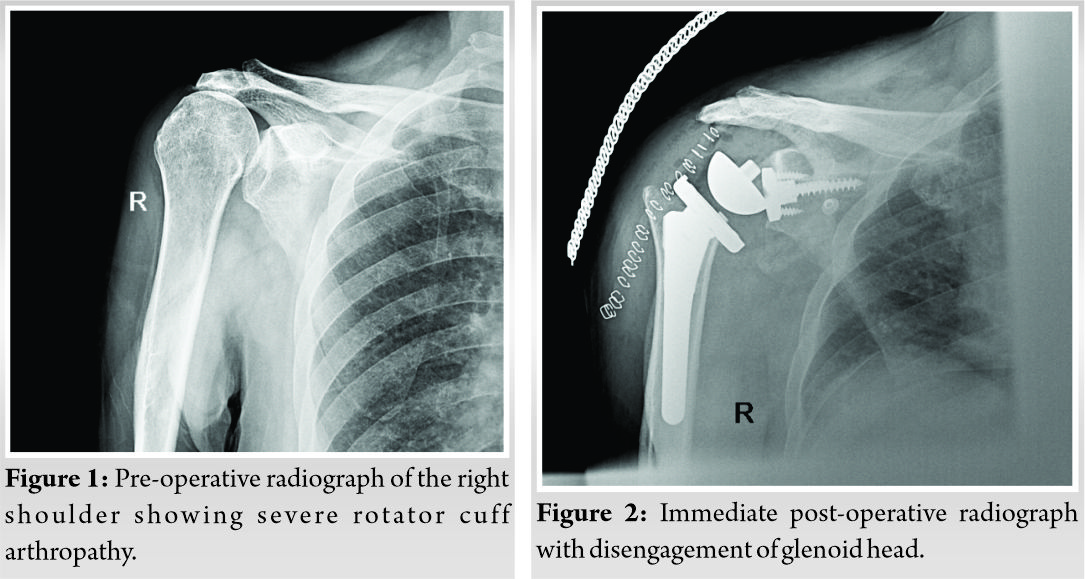
A 75-year-old male retired army person, with no significant medical history presented to our outpatient department with painful right shoulder for the past 1 year. On shoulder examination, range of motion (ROM) was severely restricted with active abduction of 30°, active forward flexion up to 45°, and restricted rotations. Job’s empty can test for supraspinatus muscle which was positive with marked weakness. Plain radiograph and magnetic resonance imaging of shoulder were suggestive of severe rotator cuff arthropathy with advanced glenohumeral arthritis (Fig. 1).
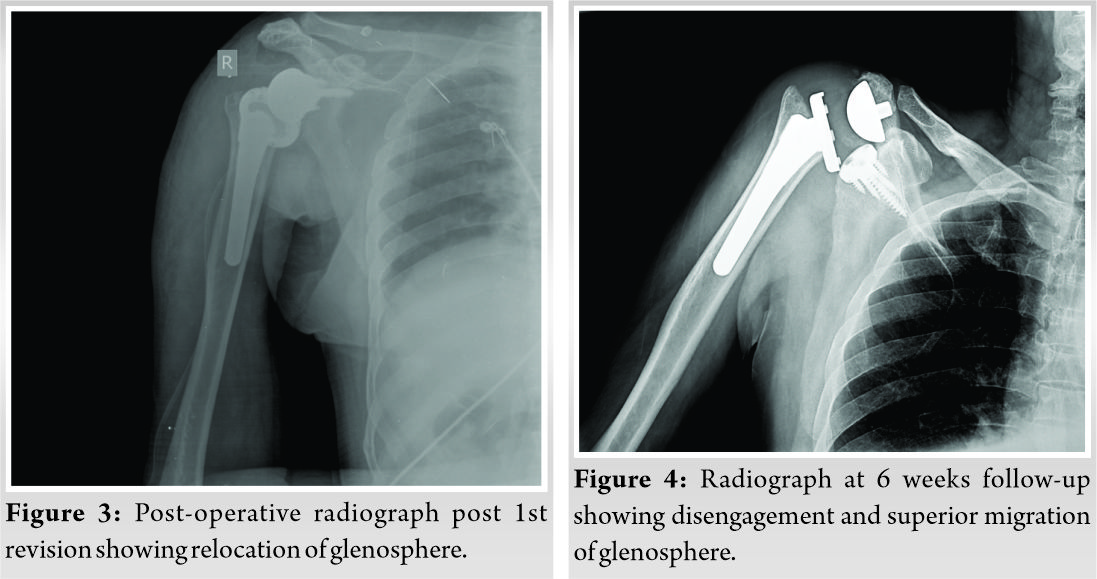
Considering patient’s clinical and radiological condition, RSR was planned. The patient underwent the procedure of standard uncemented RSR (ZIMMER-BIOMET) with deep dish polyethylene liner. The surgery was uncomplicated, and no apparent complication was encountered during glenosphere positioning and fixation to the baseplate. Immediate post-operative radiograph showed glenosphere disengagement (Fig. 2); hence, an emergency surgery was performed to relocate the sphere. Intraoperatively, some soft-tissue interposition was noticed between the glenosphere and the baseplate which was removed and component repositioning was done. Intraoperative fluoroscopy was used to ensure complete seating of the glenosphere. Immediate postoperative X-ray showed good alignment with proper component positioning (Fig. 3). Two weeks and 4 weeks follow-up were uneventful with good active ROM till 60° of forward flexion and abduction.
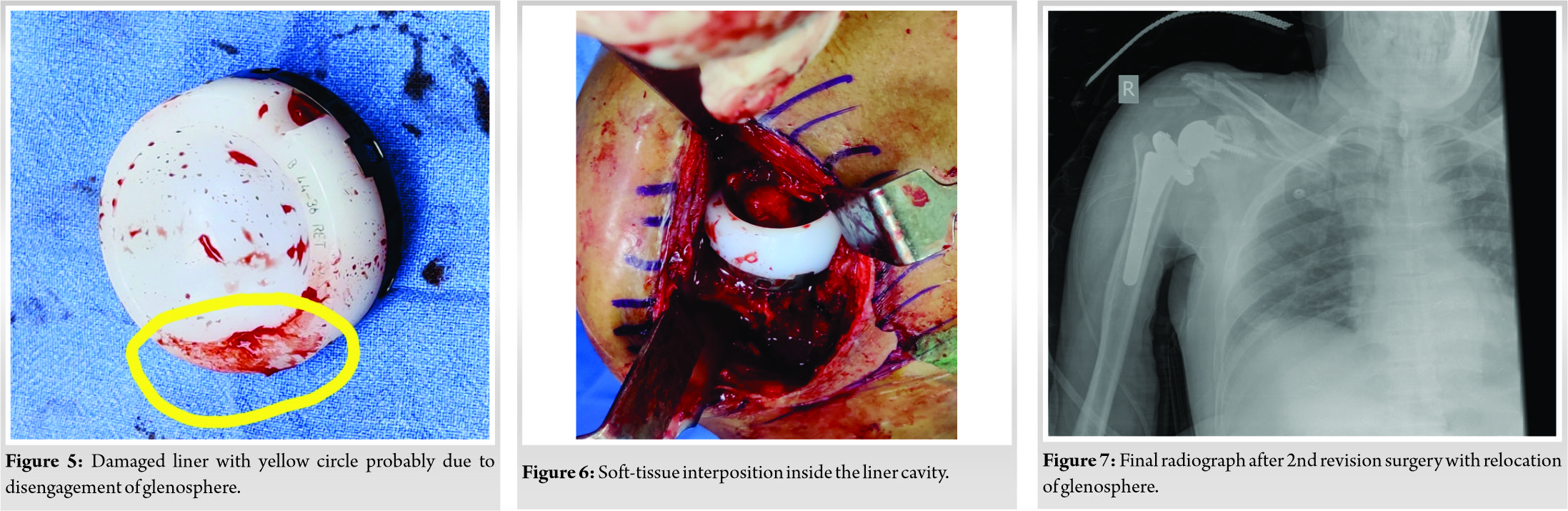
At 6 weeks follow-up, the patient complained of decreased ROM and loss of shoulder contour. A radiograph was done and glenoid sphere was found out be disengaged again with superior positioning of the component (Fig. 4), a revision surgery was hence performed. Intraoperatively superior placed glenoid sphere was removed and liner was found to be damaged (Fig. 5) likely at the time of disengagement of the glenoid and subsequent notching of the deep dish liner. Significant soft tissues were present in each of the baseplate holes overlying the screws as well as in the liner (Fig. 6).
On checking the coupling of glenoid components, we felt that the central screw length was a bit longer and may have been the triggering factor for disengagement. Hence, it was replaced with a one size smaller screw. Fresh glenoid sphere with 3 mm increased offset over the old liner and a new polyethylene liner of equal offset without deep dish design was inserted. Stability was checked and image intensifier was used to check the movements (Fig. 7). On follow-up, since then, the patient has been improving in ROM and glenosphere remains well fixed.
Instability is a common complication following RSR with high dislocation rates as mentioned above. The causes of instability are multifactorial. From a clinical point of view, it is important to exclude the following parameters in any case of post-operative instability: Soft-tissue tension, glenosphere diameter, humeral socket constraint, COR offset, mechanical impingement, bony deficiency, erroneous version, and axillary nerve dysfunction [4, 5]. Certain pre-operative factors also increase the risk of instability and should be a part of the pre-operative workup of a reverse shoulder candidate. These include body mass index >30, males, subscapularis deficiency, previous surgery, surgical approach, bone deficiency, and previous trauma. In our case, all the above factors which could have caused instability were scrutinized and excluded. Intraoperative finding of prosthesis design mismatch was the underlying cause for the recurrent instability.
Prosthesis design has evolved to combat the high dislocation rates. The older design of RSR had many complications and glenoid component failure was one of that. Unscrewing of the glenoid sphere to baseplate primarily occurred in older prostheses and resulted in a change in the prosthetic design in 1995 to a Morse taper design with central screw fixation [7, 8, 9, 10]. Mole et al. [5], in a French multicenter study, reported one patient with glenoid disengagement in 2001 as a result of improper impaction of the Morse taper.
Middernacht et al. [4] first determined the incidence of glenoid sphere disengagement and clinical outcomes in a comparative series of 479 RSR (468 Delta III & 11 Aequalis prosthesis). In this study, 16 cases of 479 shoulders (3.2%) had this complication. In 13 patients, the disengagement was partial and was not associated with a poor functional outcome as reflected by good constant score. In 3 patients (0.62%), the disengagement led to a fracture of the central screw and complete disengagement of the glenoid sphere from the baseplate requiring revision surgery. The RSR prosthesis used in these cases had Morse taper design with a central locking screw spanning from glenoid sphere to glenoid. The possible explanation provided was improper seating of the glenoid sphere leading to potential instability and interposition of bone or soft tissue between the glenoid sphere and the baseplate at the time of impaction.
Fuller et al. [6] did retrospective analysis of 40 patients (Equinoxe system) and reported two cases of glenosphere disengagement. One patient had complete and one partial disengagement. Both the patients were operated again and subsequently improved. The incidence rate of this study was calculated as 5%. The RSR prosthesis used in these cases had non-Morse taper design with a central post cage on the baseplate for bone graft. The explanation provided was of bony ingrowth inside the central post cage which led to glenosphere disengagement as being a non-Morse taper design, there is less interface stability and more chances of disengagement. Contrastingly, Crosby et al. [11] had attributed their failure to incorrect on table assembly of the glenosphere.
In our case scenario, we postulate that soft-tissue interposition was the reason for disengagement during the first episode and was successfully relocated after removal. However, the subsequent disengagement was due to improper seating of sphere because of longer central screw. On the depth gauge, reading in the initial surgery was 28 mm and hence we had opted for a 30 mm screw which we changed to a 25 mm screw in the revision. Damaged sphere and polyethylene liner were changed and it was impacted properly. Till now, the patient is doing fine and implant is positioned properly. This problem appears to be unique to the Zimmer Biomet prosthesis design and hence is different from the previous study findings. Revision to a smaller central screw size appears to be the definitive solution in such case.
Difficulty with participation in post-operative rehab, difficulty with movements and post-operative ongoing pain should alert the clinician to the possibility of glenosphere dissociation with timely imaging and intervention being key to management.
References
- 1.Cheung E, Willis M, Walker M, Clark R, Frankle MA. Complications in reverse total shoulder arthroplasty. J Am Acad Orthop Surg 2011;19:439-49. [Google Scholar]
- 2.Chalmers PN, Rahman Z, Romeo AA, Nicholson GP. Early dislocation after reverse total shoulder arthroplasty. J Shoulder Elbow Surg 2014;23:737-44. [Google Scholar]
- 3.Clark JC, Ritchie J, Song FS, Kissenberth MJ, Tolan SJ, Hart ND, et al. Complication rates, dislocation, pain, and postoperative range of motion after reverse shoulder arthroplasty in patients with and without repair of the subscapularis. J Shoulder Elbow Surg 2012;21:36-41. [Google Scholar]
- 4.Middernacht B, de Wilde L, Molé D, Favard L, Debeer P. Glenosphere disengagement: A potentially serious default in reverse shoulder surgery. Clin Orthop Relat Res 2008;466:892-8. [Google Scholar]
- 5.Mole D, Navez P, Garaud P. Reverse shoulder prosthesis: Problems related to the glenoid. In: Walch G, Boileau P, Mole D, Favard L, Levigne C, Sirveau F, editors. Reverse Shoulder Arthroplasty: Clinical Results, Complications, Revision. Montpellier, France: Sauramps Medical; 2006. p. 289-301. [Google Scholar]
- 6.Fuller CB, Gregorius SF, Lim EK. Glenosphere disengagement in a reverse total shoulder arthroplasty with a non-Morse taper design. Int Orthop 2015;39:305-8. [Google Scholar]
- 7.Boileau P, Watkinson DJ, Hatzidakis AM, Balg F. Grammont reverse prosthesis: Design, rationale, and biomechanics. J Shoulder Elbow Surg 2005;14 Suppl 1:147S-61S. [Google Scholar]
- 8.Delloye C, Joris D, Colette A, Eudier A, Dubuc JE. Mechanical complications of total shoulder inverted prosthesis. Rev Chir Orthop Reparatrice Appar Mot 2002;88:410-4. [Google Scholar]
- 9.Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Mole D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff: Results of a multicentre study of 80 shoulders. J Bone Joint Surg Br 2004;86:388-95. [Google Scholar]
- 10.Flatow EL, Harrison AK. A history of reverse total shoulder arthroplasty. Clin Orthop Relat Res 2011;469:2432-9. [Google Scholar]
- 11.Crosby L, Flurin PH, Wright T, Zuckerman JD. Response to: Fuller et al., “Glenosphere disengagement in a reverse total shoulder arthroplasty with a non-Morse taper design”. Int Orthop 2015;39:1453-4. [Google Scholar]




