
Atypical large-sized tuberous and tendinous xanthomas can co-exist due to some underlying metabolic lipid derangement and a cardiology workup to stratify future cardiac risk is a must in such patients.
Dr. Jagandeep S. Virk,
Department of Orthopaedic Oncology, Room No. E4-B2, Paras Hospitals, Panchkula, Haryana, India.
E-mail: jaganvirk_09@yahoo.co.in
Introduction: Xanthomas are defined as benign lesions characterized by an accumulation of lipid-laden macrophages that develop in the cutis and subcutaneous tissue. Xanthomas are classified as eruptive, tuberous, tendinous, or planar depending on their location and clinical appearance. Co-existence of both tuberous and tendinous forms in an atypical large-sized pattern is a rarity and presented herewith.
Case Presentation: A 48-year-old male patient presented with multiple large masses in his elbows, knees, Achilles tendons, feet, and hands. The largest swellings measured 12 cm × 10 cm in dimensions. The blood workup of the patient showed an elevated level of low-density lipoprotein cholesterol and was subsequently diagnosed with Type IIa familial hypercholesterolemia and multiple large co-existing tuberous and tendinous xanthomas which is a rare clinical presentation. Local surgical excision was performed to remove the symptomatic massive xanthomas from the elbows, knees, and feet. Histological analysis of the surgical specimens confirmed the clinical diagnosis of xanthomas.
Conclusion: Tuberous and tendinous xanthomas can co-exist in the same patient, including atypical large-sized forms. Usually, patients with xanthomas have some underlying metabolic lipid derangement and a cardiology workup to detect future cardiac risk is warranted. Intervention at an early stage can prevent the formation of disfiguring xanthomas in patients with underlying lipid disorder. The case also highlights a multi-disciplinary approach to such rare clinical presentations.
Keywords: Xanthomas, Familial Hypercholesterolemia, Giant, Tuberous.
Xanthomas are defined as benign plaques, papules, or nodules characterized by an accumulation of lipid-laden macrophages that develop in the cutis and subcutaneous tissue [1]. Xanthomas can be further classified as eruptive, tuberous, tendinous, or planar depending on their location and clinical appearance. Tuberous xanthomas are firm painless yellow-red nodules most commonly seen over extensor aspects of limbs and buttocks [2]. Tendon xanthomas are another clinical variant of xanthomas which appear as papules or subcutaneous nodules attached to tendons, fascia, or periosteum. Tendon xanthomas commonly affect the tendons of the dorsal surface of the hands and the Achilles tendon. Both tuberous and tendinous xanthomas are usually indicative of derangement in lipoprotein metabolism, in particular, Familial Hypercholesterolemia (FH) and are usually not larger than 2 cm [3]. Recently a patient presented to us with multiple large swellings varying from 2 to 12 cm on different parts of his body. Orthopedic intervention was sought to remove the symptomatic swellings. On histopathological examination, these were revealed to be an atypical presentation of giant tuberous and tendinous xanthomas. Co-existence of both forms of atypical large-sized xanthomas is a rarity and presented herewith [4, 5, 6].
A 48-year-old man presented to the orthopedic oncology outpatient department with multiple large soft-tissue swellings over the dorsum of hands, extensor aspects of his elbows, knees, and feet (Fig. 1). The swellings were also present over his heels overlying the Achilles tendons. The swellings started when the patient was 26 years of age and gradually kept on increasing in size to their present-day form. These swellings varied in size from 2 cm × 2 cm of few swellings over the dorsum of hands to 12 cm × 10 cm over the dorsum of feet. On examination, these swellings were firm, non-tender, mobile, and few swellings had developed overlying skin changes in the form of reddish-yellow discoloration and stretched-out appearance. The family history was unremarkable. Blood investigations (hemogram, serum electrolytes, liver enzymes, renal function, and blood glucose) and chest radiographs which the patient was carrying were completely normal. A dermatology consult was sought and based on the clinical history and appearance of the swellings; a provisional diagnosis of Multiple Xanthomas was considered. The lipid profile of the patient was got done and it revealed very high serum cholesterol and serum LDL (Low-density lipoproteins) levels. His lipid profile was as follows: Total cholesterol: 476 mg/dL; low-density lipoprotein (LDL): 361 mg/dL; triglyceride (TG): 103 mg/dL; very LDL (VLDL): 24 mg/dL; and high-density lipoprotein (HDL): 50 mg/dL. The lipid profile derangement pattern was suggestive of Type IIa FH.

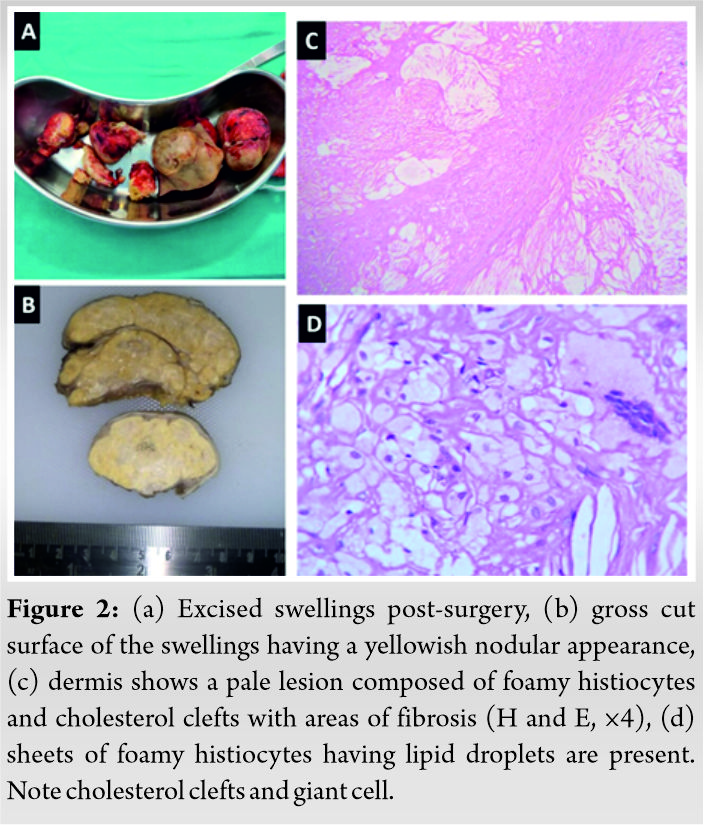
Since, the patient had extremely large swellings at certain regions, due to which he experienced trouble in kneeling and walking, a surgical plan to excise the symptomatic swellings – over the elbow, over the patellar region, and over the heel was made. The excised swellings were sent for histopathological examination. The gross cut surface of the swellings was reported to be firm with yellowish to orangish nodular appearance. On microscopy, all soft-tissue swellings had a similar morphological appearance consisting of nodules composed of sheets of foamy histiocytes, numerous cholesterol clefts, and giant cells in dermis and subcutis (Fig. 2). The final histopathological report was consistent with a diagnosis of xanthomas. The patient recovered uneventfully following the surgery.
Since the patient was diagnosed with hypercholesterolemia, the patient was started on lipid-lowering medications including high dose statins with niacin. He also underwent a cardiac evaluation to see for systemic manifestations of hypercholesterolemia including atherosclerosis and coronary artery disease. The patient was strongly positive for exercise-induced ischemia on treadmill exercise stress test and subsequently started on appropriate cardiac medications. At the last follow-up with us, the patient reported improvement in his lipid profile and a generalized global reduction of the size of the remaining xanthomas, with no development of any new lesions.
Xanthomas are palpable masses typically found within the skin or subcutaneous tissue. They consist of cholesterol, cholesterol esters, triglycerides, phospholipids, and numerous lipid-laden foamy macrophages [1]. Xanthomas are commonly caused by a disturbance in lipoprotein metabolism and commonly occur in patients with FH [7, 8, 9]. The pathology behind the formation of cutaneous xanthomas is not fully understood and may differ based on the etiology and type of xanthoma. The hypothesis behind the occurrence of xanthomas secondary to hyperlipidemia is that, since serum levels of lipoproteins are substantially elevated, extravasations of lipoproteins through dermal capillary blood vessels with subsequent engulfment by macrophages leads to the formation of xanthomas [10, 11]. Histopathologically, xanthomas are characterized by the presence of vacuolated macrophages filled with lipid droplets in the dermis. Tendon, tuberous and plane xanthomas are some clinical variants of xanthomas seen in FH TypeIIa, as were seen in our case.
Tuberous xanthomas typically appear as reddish-yellow papulonodular lesions of the skin. They are most commonly found over pressure areas such as extensor aspects of knees, elbows, and buttocks [2]. Tuberous xanthomas are rarely larger than a few centimeters in size; however, in our patient, they ranged up to 12 cm × 10 cm in size. Tendon xanthomas are cholesterol deposits in tendons. They commonly affect the tendons of the dorsal surface of the hands and the Achilles tendon. Co-existence of both forms of atypical large-sized xanthomas is a rarity with not many cases reported in the literature [4, 5, 6]. The existence of large-sized xanthomas of both tuberous and tendinous nature was most likely because of the delayed presentation of the patient before seeking medical or surgical intervention. The underlying cause of the different types of xanthomas is most likely explained by the nature of tissues where lipid deposition takes place because of the deranged lipid metabolism in the body. The production of heat, movement, and friction increases capillary leakage of LDL which explains and influences the location of tuberous and tendinous xanthomas [7]. The recent significant increase in the size of the swellings causing disfigurement and difficulty in routine activities because of their location over extensor aspect of the joints, made the patient seek our intervention.
Tendinous and tuberous xanthomas may indicate FH and increased cardiovascular risk, as xanthomas are associated with elevated plasma concentrations of LDL. The presence of xanthomas increases the risk of cardiovascular disease in patients with FH by as much as three-fold, indicating that xanthomas and atherosclerosis may share a certain etiology [12, 13]. Dietary modification and treatment with the statin group of drugs are recommended. Cardiac evaluation, as was done in our case, is recommended in cases presenting late to stratify the risk for any future cardiovascular event and take appropriate intervention accordingly.
Tuberous and tendinous xanthomas can co-exist in the same patient, including atypical large-sized tuberous xanthomas. Usually, patients with xanthomas have some form of underlying metabolic lipid derangement and a cardiology workup to detect future cardiac risk is warranted. Early intervention can prevent the formation of disfiguring xanthomas in patients with underlying lipid disorder. A multidisciplinary approach to such lesions including inputs from dermatology, pathology, and oncology is a must for correct diagnosis and appropriate treatment.
The clinical appearance of xanthomas is typical and a high index of suspicion of the possibility of this condition should be maintained on the clinical appearance itself. The same should be correlated on histopathology. Usually, xanthomas have some form of underlying metabolic lipid disorder and the presence of atypical large-sized xanthomas warrants a thorough cardiac evaluation besides treating this condition to prevent any future cardiac complication.
References
- 1.Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol 1985;13:1. [Google Scholar]
- 2.Mohan KK, Kumar KD, Ramachandra BV. Tuberous xanthomas in Type II a hyperlipoproteinemia. Indian J Dermatol Venereol Leprol 2002;68:105-6. [Google Scholar]
- 3.Cruz PD Jr., East C, Bergstresser PR. Dermal, subcutaneous, and tendon xanthomas: Diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988;19:95-111. [Google Scholar]
- 4.Zhao C, Kong M, Cao L, Zhang Q, Fang Y, Ruan W, et al. Multiple large xanthomas: A case report. Oncol Lett 2016;12:4327-32. [Google Scholar]
- 5.Tummidi S, Kothari K, Rojekar A, Tiwari A. Multiple tuberous and tendinous xanthomas diagnosed on fine-needle aspiration cytology-report of a rare case. Diagn Cytopathol 2019;47:939-42. [Google Scholar]
- 6.Kong MX, Zhang Q, Cao L, Zhao C, Ru GQ, Bi Q. Familial hypercholesterolaemia with tuberous and tendinous xanthomas: Case report and mutation analysis. Clin Exp Dermatol 2015;40:765-9. [Google Scholar]
- 7.White LE. Xanthomatoses and lipoprotein disorders. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick’s Dermatology in General Medicine. 7th ed. New York: McGraw-Hill; 2008. p. 1272-81. [Google Scholar]
- 8.Murphy GF, Sellheyer K, Mihm MC. The skin. In: Kumar V, Abbas AK, Fausto N, editors. Robbins and Cotran Pathologic Basis of Disease. 7th ed. Philadelphia, PA: Elsevier; 2004. p. 1248. [Google Scholar]
- 9.Zak A, Zeman M, Slaby A, Vecka M. Xanthomas: Clinical and pathophysiological relations. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2014;158:181-8. [Google Scholar]
- 10.Smellie WS. Hypertriglyceridaemia in diabetes. BMJ 2006;333:1257-60. [Google Scholar]
- 11.Wheeler DC, Bernard DB. Lipid abnormalities in the nephrotic syndrome: Causes, consequences, and treatment. Am J Kidney Dis 1994;23:331-46. [Google Scholar]
- 12.Yamashita S, Hbujo H, Arai H, Harada-Shiba M, Matsui S, Fukushima M, et al. Long-term probucol treatment prevents secondary cardiovascular events: A cohort study of patients with heterozygous familial hypercholesterolemia in Japan. J Atheroscler Thromb 2008;15:292-303. [Google Scholar]
- 13.Civeira F, Castillo S, Alonso R, Meriño-Ibarra E, Cenarro A, Artied M, et al. Spanish familial hypercholesterolemia group: Tendon xanthomas in familial hypercholesterolemia are associated with cardiovascular risk independently of the low-density lipoprotein receptor gene mutation. Arterioscler Thromb Vasc Biol 2005;25:1960-5. [Google Scholar]






