
Since it is a rare entity with a very less known genetic and molecular basis of inheritance, so every case deserves to be evaluated for a better understanding of the pathology and management.
Dr. Maneesh Verma,
Department of Orthopaedics, Government Medical College, Datia 462 046, Madhya Pradesh, India.
E-mail: drmaneeshortho@gmail.com
Introduction: Fibular aplasia, tibial campomelia, and oligosyndactyly (FATCO) syndrome is a rare disorder with unknown molecular basis. Since it is a rare disorder, so it is commendable to report the each case, due to its sporadic incidence and paucity of the standardized management protocol for their management.
Case Report: It is a case report of newly born male baby, whose anxious parents presented to the outpatient department with a deformity in the left lower limb. This resembled the FATCO syndrome. After clinico-radiological workup, it was categorized as a variant of FATCO syndrome.
Conclusion: ounseling of parents should be done and let them realize that what is inescapable with this syndrome and what is bound to happen during the treatment.
Keywords: Variant, FATCO, RARE
Jacqueline T. Hecht and Charles I. Scott, Jr (1981) 1st time described the features of congenital limb anomaly (short leg, ankle, foot, absence of rays) in half of the siblings (male), and suggested that it has a genetic association (recessive inheritance or gonadal mosaicism) [1]. In 2005, Courtens et al. described a male newborn baby with features of fibular aplasia, tibial campomelia, and oligosyndactyly and named it fibular aplasia, tibial campomelia, and oligosyndactyly (FATCO) syndrome. Since their findings were quite similar to Hecht and Scott’s original description, so it is also called Hecht Scott Syndrome [2].
The FATCO syndrome is a rare disorder with a roughly calculated incidence of 5.7 to 20 cases/1 million births [3]. Hence, it is commendable to report each case, due to its sporadic incidence and paucity of the standardized management protocol for this rare entity. FATCO syndrome variant may also be associated with other congenital deformities. Here we are presenting a male child, born by non-consanguineous marriage having features similar to the FATCO syndrome variant. Prior to this case report, no one case ever has been reported of the FATCO syndrome variant with absent talus and ipsilateral absent proximal tibial growth plate.
It is a case report of 14 days old newly born male baby, whose anxious parents presented to the outpatient department with a deformity in the left lower limb of the baby. It was, the first offspring of non-consanguineous parents (mother age- 32 years and father age 33 years), born at the full term by vaginal delivery and birth weight was 2600 g (above 50th percentile). The APGAR scores were 2 at first, and 6 at 5th min, respectively. The history-taking did not reveal a history of rash, teratogenic drug, radiation exposure, or fever in the antenatal period.
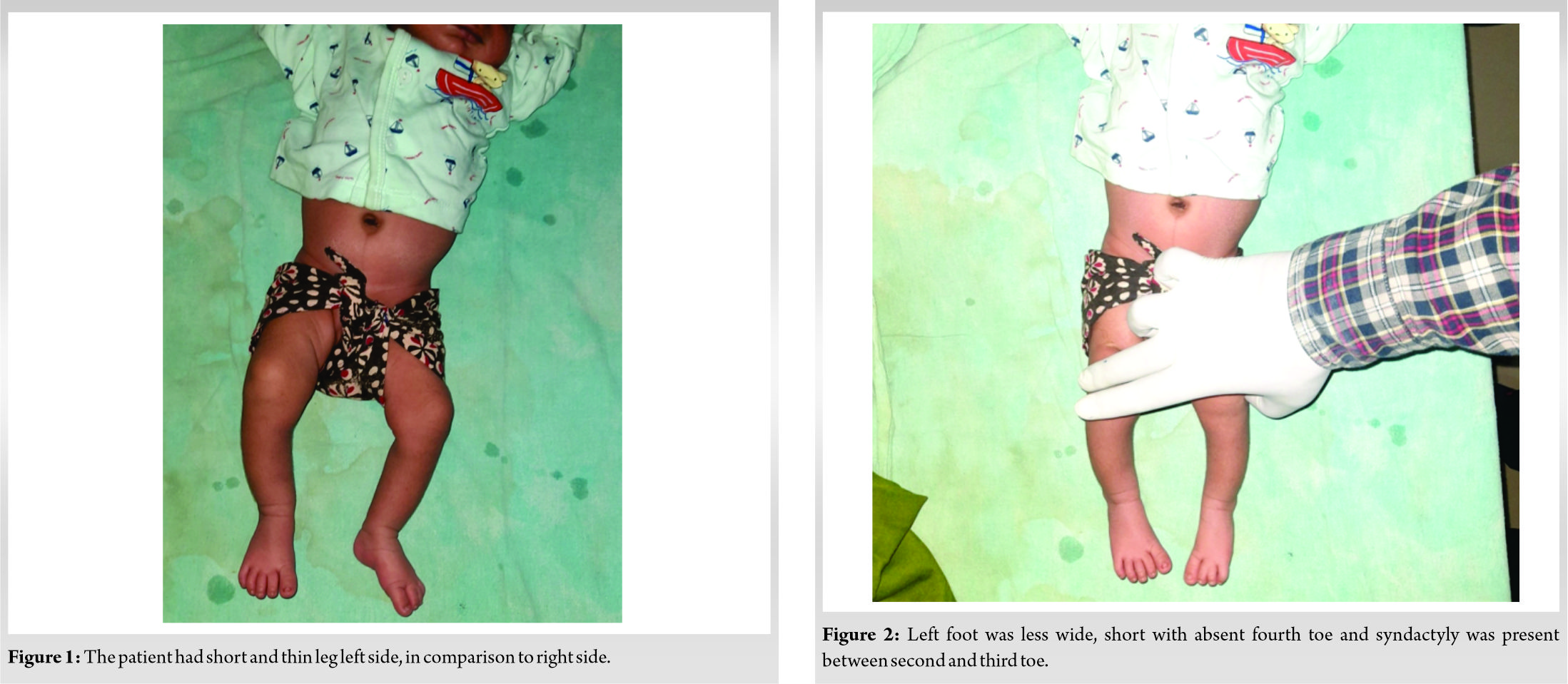
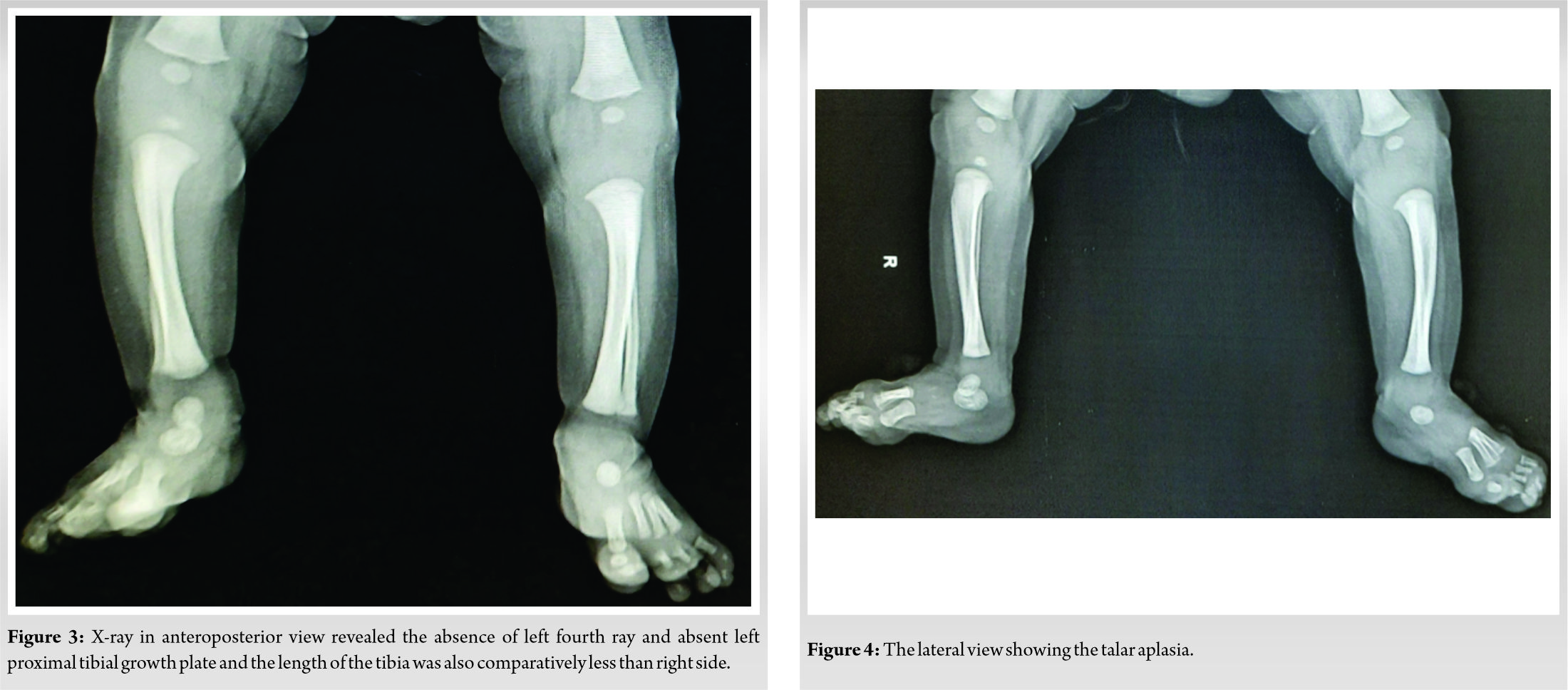
On inspection of the lower limb of the baby, the left leg was short and thin in comparison to the right side (Fig. 1). The left foot appeared shorter due to absent fourth ray and the syndactyly was between 2nd and 3rd toe (Fig. 2). There was no bowing or associated skin dimpling over the limb. On palpation, the ankle joint was normal but the left knee was laxed on a medial and lateral stress test in comparison to the right side. Examination of another side of the limb, upper limb, face, pelvis, and spine were normal. Systemic examination did not reveal any additional findings. The X-ray of the lower limb showed the absence of proximal tibial epiphysis, absent talus, and absence of the fourth ray on the left side. Due to the absent left proximal tibial epiphysis, the tibia, as well as the fibula, was shorter than the normal side (Fig. 3, 4).
The skeletal survey of the rest of the body, showed the normal femora, contra-lateral leg, pelvis, and long bones of the upper limb. The ultrasonographic examination of the pelvis and abdomen was non-significant. Finally, the karyotyping was done, which was normal. Ultimately after a diligent literature search, a diagnosis of FATCO syndrome variant was installed.
The exact etiology and genetic basis for the inheritance of FATO syndrome are not clear. Since the mutations of the WNT7A gene control the development of the dorsoventral part of a limb, so it was hypothesized that the WNT7A gene mutation is accountable for FATCO syndrome. Although most of the reported cases of FATO syndrome are sporadic, the X-linked, autosomal recessive, and autosomal dominant patterns have been found to be associated with it. Karaman and Kahveci found that the WNT7A gene is not a potential causative factor for FATCO syndrome [4]. Furthermore, Bieganski et al. reported the three cases of FATCO syndrome. They also conducted the genetic screening, but it could not find any genetic correlation. They proposed that FATCO syndrome is supposed to pertain to the phenotype of “fibular aplasia with ectrodactyly” [5]. Though, their presumption about FATCO syndrome is yet to be recognized by molecular genetics.
Onder et al. reported a monozygotic twin sister with FATCO syndrome, while the other twin sister was healthy and without any malformation. As we know, that, monozygotic twins are genetically identical or they have the same DNA sequence. Hence, despite having the same DNA sequence how did FATCO syndrome happen in one of the monozygotic twin sisters. Hence we can say that FATCO syndrome does not occur only due to a gene mutation but also by other unknown mechanisms [6]. Moreover, one case report also has found the correlation of chromosomal aberration with FATCO syndrome [7]. Hence, this syndrome has wide variability in expression, as well as an uncertain pattern of inheritance. And so far, there is a lack of exact information related to familial transmission.
The closest differential diagnosis of FATCO syndrome is Al-Awadi-Raas-Rothschild syndrome and Fuhrmann syndrome. Fuhrmann syndrome (resembling FATCO syndrome with broad-spectrum involvement in the form of hypoplasia/aplasia of femur, pelvis, ulna, and dysplastic nails) is a mild variant of Al-Awadi-Raas-Rothschild syndrome, and both are inherited as autosomal recessive disease and caused by mutations in WNT7A gene [8]. Although the Fuhrmann syndrome (OMIM no. 276820) is a quite different limb disorder than FATCO syndrome (OMIM no. 246570), there is a case report of extremely rare congenital limb deficiency disorder had the overlapping features of both FATCO and Fuhrmann’s syndromes [9].
Best of our knowledge, thirteen cases of classical FATCO syndrome have been reported [10] Goyal et al. reported a case with unilateral fibular hypoplasia, tibial cam¬pomelia, and oligodactyly. Although, the typically defined FATCO syndrome has fibular (unilateral or bilateral) aplasia, so they coined the term FATCO syndrome variant for their case report [11]. The second case of the FATCO syndrome variant was reported by Smets et al. [10]. Our case had oligosyndactyly, absent talus, and hypoplastic tibia and fibula (due to absent proximal tibial growth plate). Till now, no one has reported any case of FATCO syndrome with an absent proximal tibial growth plate. Which led to primary proximal tibial hypoplasia and obviously (secondary) fibular (hypoplasia) shortening in our case. Although this case did not show a classical feature of tibial campomelia (bent limb with characteristic skin dimple), but the other features are justifying it to be categorized as a variant of FATCO syndrome. Hence, here we have a claim for this case as FATCO syndrome variant. To the best of our knowledge, here we are reporting the third case report (second from India) whose clinical/radiological features fall under the domain of the FATCO syndrome variant.
Kinds of literature have suggested that the early prenatal diagnosis of FATCO syndrome is possible and the nuchal translucency may be the earliest feature on ultrasonography at 24 weeks of ges¬tation. The FATCO syndrome has normal brain development and it is not associated with any dysmorphic feature of the face or any other anomaly at the birth. Hence, these favorable features may be helpful in counseling and resolving the personal, social, or psychological problems of parents [12].
The objectives of management in such cases are correction of limb length inequality, functional stabilization of joints (knee and ankle). The of orthosis for unstable joints, epiphysiodesis, and limb lengthening procedures for limb length correction and amputation (Symes) with prosthesis for non-salvageable limb is commonly practiced methods to manage the case [13, 14]. In our case, parents were anxious for short legs, short foot, and absent toe. They were counseled that, short foot and absence of toe are not supposed to functionally destabilize the ankle joint significantly. Later on, limb length inequality will get managed surgically, and right now knee orthosis will be used for clinically evident knee instability. Various other deformities may be associated with FATCO syndrome-like bowing of tibia, valgus knee, and condylar agenesis short femur. In our case, clinical instability at the knee, short leg, and short foot had imparted great concern to the parents.
With time, the addition of more case reports will make a better understanding of this rare syndrome. The early and more précised prenatal diagnosis of FATCO syndrome or its variant will be highly helpful for prenatal counseling of the parents regarding the morbidity due to it. This rare syndrome has a sporadic nature and still unknown exact mode of inheritance, so in such case the role of genetic counseling is not clear. Prenatal counseling of parents is to realizing them that what is inescapable and bound to happen.
Counseling of anxious parents is a very important aspect of the management. Parents must be acknowledged about the syndrome, that what exactly it is and what will be the holds of the disease over the child and parents over the time ahead. Hence, it will be very helpful in the management of it and resolving the social and psychological issues.
It is a rare exceptional congenital disorder of unknown molecular genetics. In near future, the additional case reports will be helpful for the better delineation of this less understood limb deficiency disorder.
References
- 1.Hecht JT, Scott CI Jr. Limb deficiency syndrome in half-sibs. Clin Genet 1981;20:432-7. [Google Scholar]
- 2.Courtens W, Jespers A, Harrewijn I. Fibular aplasia, tibial campomelia, and oligosyndactyly in a male newborn infant: A case report and review of the literature. Am J Med Genet A 2005;134:321-5. [Google Scholar]
- 3.Florio I, Wisser J, Huch R, Huch A. Prenatal ultrasound diagnosis of a femur-fibula-ulna complex during the first half of pregnancy. Fetal Diagn Ther 1999;14:310-2. [Google Scholar]
- 4.Karaman A, Kahveci H. A male newborn infant with fatco syndrome (fibular aplasia, tibial campomelia and oligodactyly): A case report. Genet Couns 2010;21:285-8. [Google Scholar]
- 5.Bieganski T, Jamsheer A, Sowinska A, Baranska D, Niedzielski K, Kozlowski K, et al. Three new patients with FATCO: Fibular agenesis with ectrodactyly. Am J Med Genet A 2012;158A:1542-50. [Google Scholar]
- 6.Onder Yılmaz H, Topak D, Yılmaz O, Çakmaklı S. A Turkish female twin sister patient with fibular aplasia, congenital tibia pseudoarthrosis, oligosyndactyly, and negative WNT7A gene mutation. J Pediatr Genet 2019;8:95-9. [Google Scholar]
- 7.Ekbote AV, Danda S. A case report of fibular aplasia, tibial campomelia, and oligosyndactyly (FATCO) syndrome associated with Klinefelter syndrome and review of the literature. Foot Ankle Spec 2012;5:37-40. [Google Scholar]
- 8.Al-Qattan MM. Molecular basis of the clinical features of Al-Awadi-Raas-Rothschild (limb/pelvis/uterus-hypoplasia/aplasia) syndrome (AARRS) and Fuhrmann syndrome. Am J Med Genet A 2013;161A:2274-80. [Google Scholar]
- 9.Abdalla EM, El-Beheiry AA. Overlap between fibular aplasia, tibial campomelia, and oligosyndactyly and fuhrmann’s syndromes in an Egyptian female infant. J Pediatr Genet 2017;6:118-21. [Google Scholar]
- 10.Smets G, Vankan Y, Demeyere A. A female newborn infant with FATCO syndrome variant (fibular hypoplasia, tibial campomelia, oligosyndactyly)-a case report. J Belg Soc Radiol 2016;100:41. [Google Scholar]
- 11.Goyal N, Kaur R, Gupta M. FATCO syndrome variant-fibular hypoplasia, tibial campomelia and oligosyndactyly-a case report. J Clin Diagn Res 2014;8:LD01-2. [Google Scholar]
- 12.Capece G, Fasolino A, Monica MD, Lonardo F, Scarano G, Neri G. Prenatal diagnosis of femur-fibula-ulna complex by ultrasonography in a male fetus at 24 weeks of gestation. Prenat Diagn 1994;14:502-5. [Google Scholar]
- 13.Choi IH, Kumar SJ, Bowen JR. Amputation or limb-lengthening for partial or total absence of the fibula. J Bone Joint Surg Am 1990;72:1391-9. [Google Scholar]
- 14.Epps CH Jr., Schneider PL. Treatment of hemimelias of the lower extremity. Long-term results. J Bone Joint Surg Am 1989;71:273. [Google Scholar]




