
Stepwise approach for CT-guided minimally invasive percutaneous C2 biopsy procedure helps in getting repeatable and high yielding results with safety and accuracy especially in technically challenging areas such as C2 vertebrae.
Dr. Rajendra T. Sakhrekar, Department of Spine Surgery, Sancheti Institute of Orthopedics and Rehabilitation, Shivajinagar, Pune - 411 005, Maharashtra, India. E-mail: raj.sakhrekar1@gmail.com
Introduction: Minimally invasive percutaneous CT-guided biopsies of the spine are well established. Although, technical difficulties with CT-guided percutaneous intervention of the C2 body present due to the smaller size of the vertebral elements and potential injury of the critical adjacent structures such as Carotid arteries laterally, vertebral artery, and cervical nerve posterolaterally, pharynx and larynx anteriorly, and spinal cord in the cervical spinal canal. Routinely transoral approach is used for the percutaneous intervention of the C2 body. Literature on the posterolateral approach for biopsies of the C2 vertebral body is sparse as compared to other approaches. This case report presents a case of adenocarcinoma diagnosed with CT-guided percutaneous biopsy of the C2 body using a posterolateral approach under local anesthesia.
Case Report: A 70-year-old female presented to our outpatient clinic with complaints of progressively increasing neck pain with a visual analog score (VAS) 7/10. Neck pain was radiating to the base of the occiput and aggravated by neck movements. On clinical examination, there was axial tenderness at the base of the skull and the upper part of the cervical spine. Neurological examinations of sensory and power in all the limbs were normal. Systemic examination and laboratory parameters did not reveal any abnormality. X-rays and MRI revealed a fracture of the odontoid process with marrow edema with differentials of metastasis. PET scan revealed left lung lesion likely to be primary lesion and lesion in C2 vertebral body as likely metastasis. A minimally invasive percutaneous CT-guided posterolateral approach for biopsy proved moderately differentiated adenocarcinoma from the lung with metastasis to C2 vertebrae. The patient was started on an appropriate Chemotherapy regimen as per the Immunohistochemistry (IHC) and Genomic studies with adjuvant radiotherapy.
Conclusion: Understanding the detailed anatomy prior to CT guided minimally invasive percutaneous C2 biopsy procedure helps in increasing its safety, precision, and high yield. Stepwise approach to the procedure aids in getting repeatable and high-yielding results especially in a technically challenging area such as C2 vertebrae.
Keywords: Adenocarcinoma, C2 cervical vertebral body, CT guided biopsy, posterolateral approach, safety.
Minimally invasive percutaneous biopsies of the spine are well established [1, 2, 3, 4, 5]. Although, technical difficulties with CT-guided percutaneous intervention of the C2 body present due to smaller size of the vertebral elements and potential injury of the critical adjacent structures like Carotid arteries laterally, vertebral artery, and cervical nerve posterolaterally, pharynx and larynx anteriorly, and spinal cord in the cervical spinal canal [1]. A routinely transoral approach is used for the percutaneous intervention of the C2 body, for which general anesthesia is mandatory, which needs nasopharyngeal intubation. Also, the transoral approach has increased the chances of infection compared with other approaches. Literature on the posterolateral approach for biopsy of the C2 vertebral body is sparse as compared to other approaches [6, 7, 8, 9, 10]. This case report presents a case of adenocarcinoma diagnosed with CT-guided percutaneous biopsy of the C2 body using a posterolateral approach under local anesthesia.
A 70-year-old female presented to our outpatient clinic with complaints of progressively increasing neck pain with a Visual Analog Score (VAS) of 7/10. Neck pain was radiating to the base of the occiput and aggravated by neck movements and prolonged sitting affecting Activities of daily living (ADLs). On clinical examination, there was axial tenderness at the base of the skull and upper part of the cervical spine, Paraspinal muscle spasm with terminal restriction of movements, especially rotation due to pain. Neurological examinations of sensory and power in all the limbs were normal. Systemic examination and laboratory parameters did not reveal any abnormality. Orthogonal view of X-ray Cervical spine revealed degenerative changes in the cervical spine with lytic lesion present in the body of C2 with detailed description difficult due to C1 atlas vertebrae overlap (Fig. 1).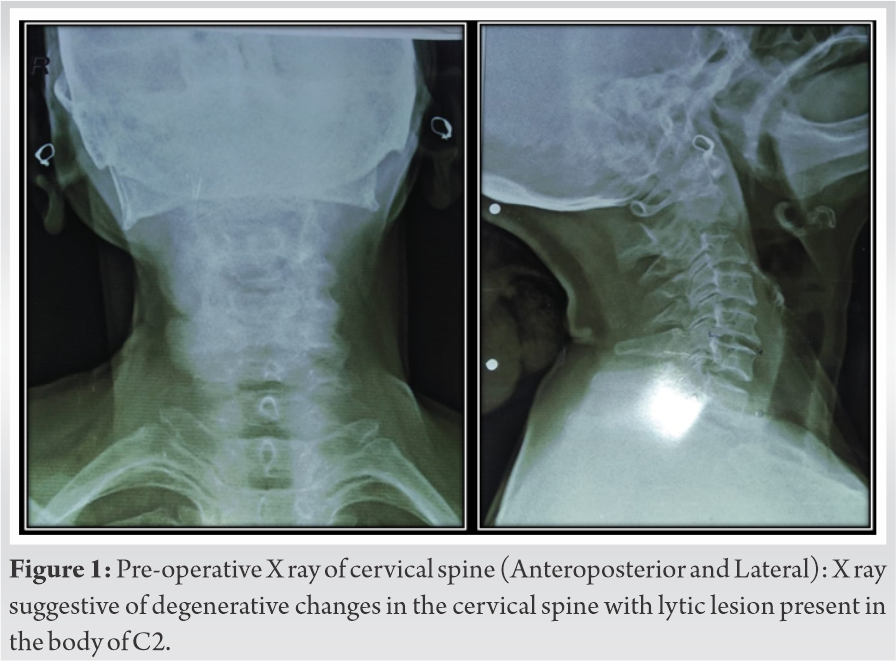 Magnetic Resonance Imaging (MRI) revealed a fracture of the odontoid process with associated marrow edema. Marrow signal abnormality in C2 also involves the right neural arch of the C2 with mild expansion and paravertebral soft tissue indenting the thecal sac (Fig. 2, 3).
Magnetic Resonance Imaging (MRI) revealed a fracture of the odontoid process with associated marrow edema. Marrow signal abnormality in C2 also involves the right neural arch of the C2 with mild expansion and paravertebral soft tissue indenting the thecal sac (Fig. 2, 3). 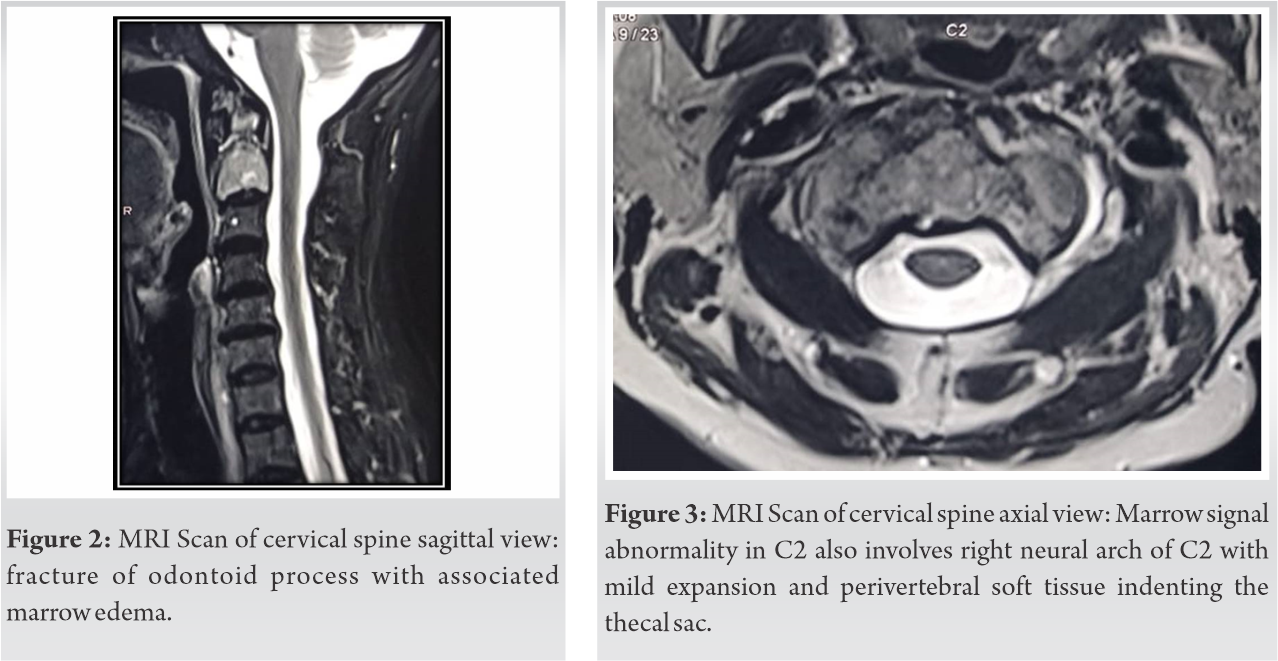 MRI suggested the possibility of neoplastic etiology was likely although infective etiology could not be ruled out. Positron Emission Tomography (PET) scan was done for the search of primary. PET scan showed metabolically active soft tissue density heterogeneously enhancing irregular margin mass lesion in the left upper lobe of lung – likely primary. Scan also revealed metabolically active lytic sclerotic expansile lesion involving odontoid process and body of C2 vertebra- likely metastasis (Fig. 4, 5).
MRI suggested the possibility of neoplastic etiology was likely although infective etiology could not be ruled out. Positron Emission Tomography (PET) scan was done for the search of primary. PET scan showed metabolically active soft tissue density heterogeneously enhancing irregular margin mass lesion in the left upper lobe of lung – likely primary. Scan also revealed metabolically active lytic sclerotic expansile lesion involving odontoid process and body of C2 vertebra- likely metastasis (Fig. 4, 5). 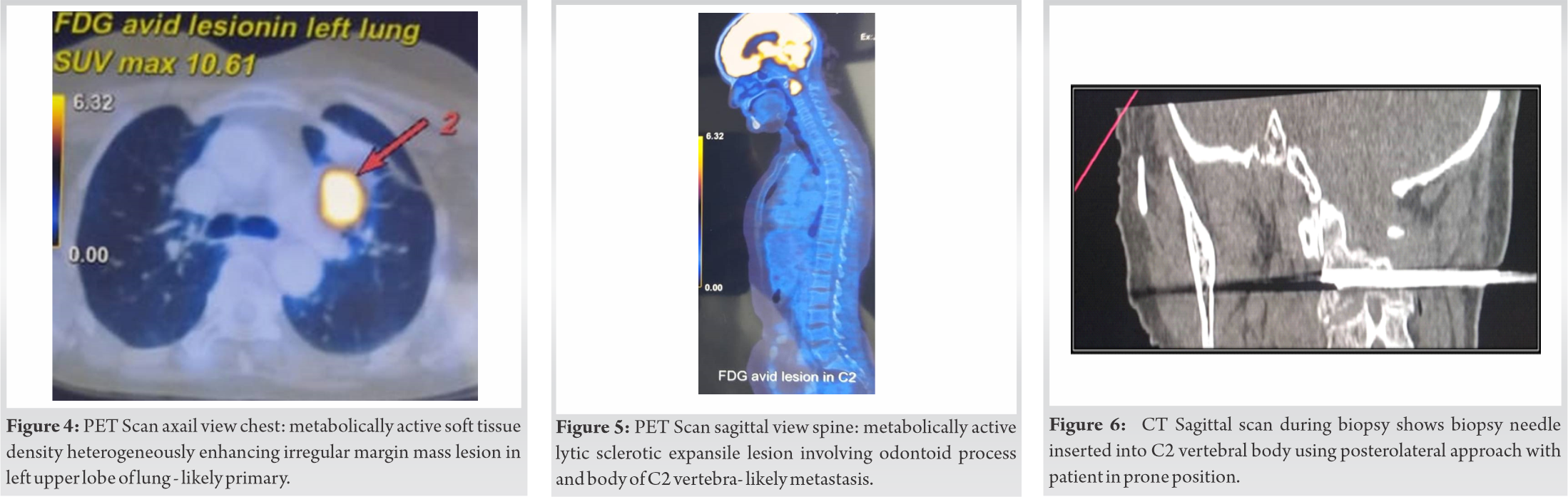 In view of the above clinical and radiological findings CT scan guided transpedicular C2 vertebrae and lung biopsy was performed (Fig. 6, 7). The procedure was safe and uneventful. The duration of the procedure was 54 min. The patient was observed for 60 min in daycare and then discharged. There were no early or late complications noted. Histopathological examination of the biopsy revealed moderately differentiated adenocarcinoma from the lung with metastasis to C2 vertebrae (Fig. 8).
In view of the above clinical and radiological findings CT scan guided transpedicular C2 vertebrae and lung biopsy was performed (Fig. 6, 7). The procedure was safe and uneventful. The duration of the procedure was 54 min. The patient was observed for 60 min in daycare and then discharged. There were no early or late complications noted. Histopathological examination of the biopsy revealed moderately differentiated adenocarcinoma from the lung with metastasis to C2 vertebrae (Fig. 8).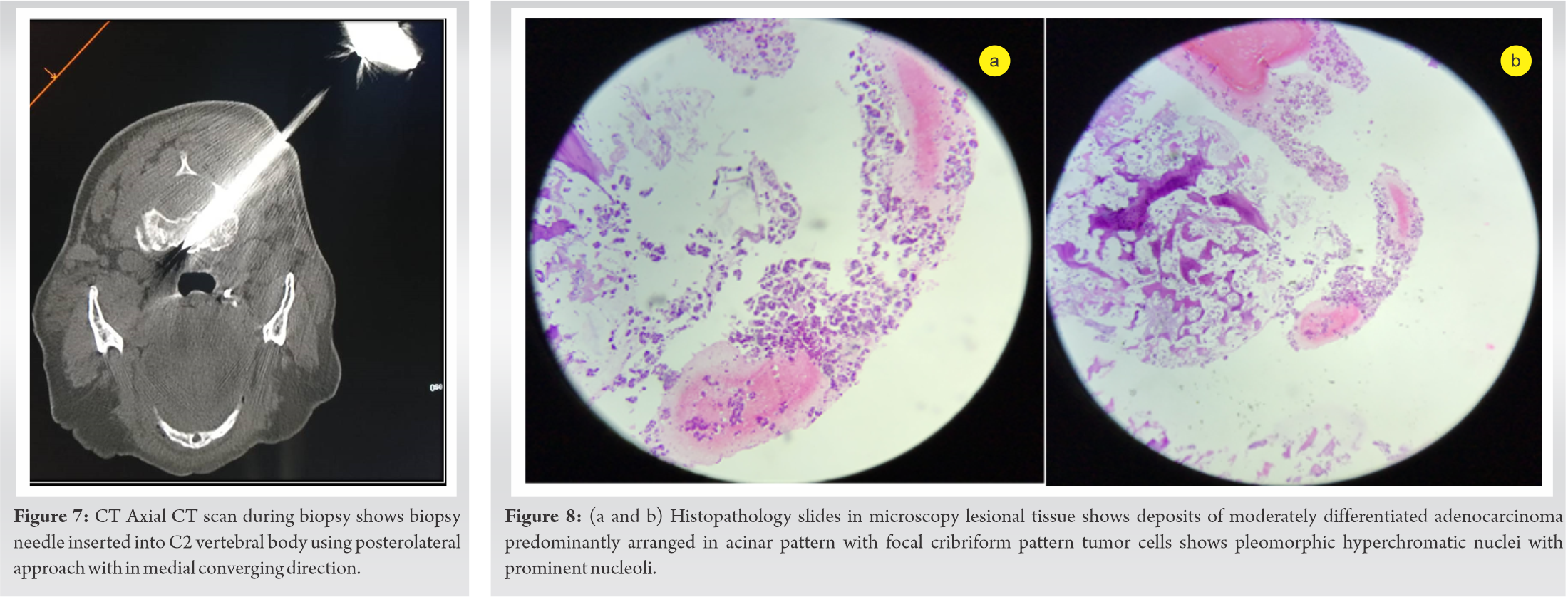 The patient was started on an appropriate Chemotherapy regimen as per the Immunohistochemistry (IHC) and Genomic studies with adjuvant radiotherapy.
The patient was started on an appropriate Chemotherapy regimen as per the Immunohistochemistry (IHC) and Genomic studies with adjuvant radiotherapy.
The high yield of the biopsy largely depends upon how accurately and safely the biopsy sample has been procured representing the exact pathology. Hence, a standard protocol for the procedure is mandatory especially in the area such as C2 vertebrae where getting the sample from the desired location can be technically demanding and perilous because of the close proximity to vital structures. Here is a stepwise description of the procedure, i.e., minimally invasive percutaneous CT scan guided C2 vertebrae Transpedicular biopsy:
1. Patient positioning
2. CT scan with table positioning
3. Needle positioning
4. Determine the direction in both planes
5. Primary insertion of the Jamshedi (J) needle
6. Check CT scan and Readjustment
7. Further insertion of the J-needle
8. Final confirmation CT scan
9. Biopsy
Patient positioning
Before positioning the patient make sure the necessary arrangements are done and the instrument trolley is kept ready. Comfortable patient positioning is a crucial step for timely completion of the procedure, as constant changes will mean that all the steps are to be done again. Hence in positioning care is to be taken in comforting the patient and in line neck positioning and hands relaxed to the side of the torso or fully abducted to either side of the head. Expose the desired area of biopsy clean and drape.
CT scan with table positioning
After positioning get CT scan done of the cervical spine and table positioning is determined using axial and sagittal Ct cuts. The horizontal line is drawn using skin marker, which determines the approximate needle position in the superoinferior direction.
Needle positioning
Once the horizontal line is drawn stack of 10 pins parallel to each other 2 mm apart over the sticky bandage is stuck perpendicular to the horizontal line from the midline to the proposed biopsy side. This helps us to determine the approximate needle position in the mediolateral direction. CT scan image will determine the pin, which will help us to mark the vertical line.
Determine the direction in both planes
Intersection of the horizontal and vertical line will be leading to the point of entry on the skin. Understanding the anatomy is very crucial in determining the direction. The likely structured to be injured is the vertebral artery laterally if the infero-medial wall of the foramen transversarium is violated and the cervical spinal cord medially if the wall of the spinal canal is violated. To prevent this entry point on the C2 vertebrae is taken in such a way that the line directed towards the center of the odontoid process to reach the body does not violate any of the above structures. Thus, analyzing sagittal, coronal, and axial images of the CT scan we will get the desired entry on bone and angulation of further entry in the soft tissue to the bone in both the Sagittal and Axial plane as shown. Furthermore, the measurement of the thickness of the soft tissue between bone and skin will prevent inadvertent penetration in depth.
Primary insertion of the Jamshedi (J) needle
After determining the angulation and depth trajectory path is anesthetized using 2% lignocaine with or without adrenaline up to the periosteum. Number 11 or 10 Jamshedi (J) needle with trocar is inserted in the calculated trajectory just to pierce the near cortex and needle to stand unsupported.
Check CT scan and readjustment
A check CT scan is taken to confirm the desired trajectory and calculate the further depth of insertion. If any readjustment is required is done at a stage and rescan might be necessary for the changed direction.
Further insertion of the J-needle
If the trajectory is satisfactory then the trocar is removed and the needle is further inserted in a corkscrew manner up to the calculated needle marking outside
Final confirmation CT scan
Taking a final CT scan for confirmation is not mandatory but can be taken to check the final positioning of the needle, especially in the small lesions. Once confirmed the needle can be withdrawn and bone biopsy can be collected with stylet in a sterile manner. The above procedure might require repetitions in case of more samples are required.
Biopsy
Histopathology confirming the diagnosis of adenocarcinoma. In microscopy lesioned tissue shows deposits of moderately differentiated adenocarcinoma predominantly arranged in acinar pattern with focal cribriform pattern tumor cells shows pleomorphic hyperchromatic nuclei with prominent nucleoli.
Minimally invasive percutaneous CT-guided posterolateral approach to cervical spine biopsy can be used for both infection and primary or metastatic lesions. It can reduce the need for a transoral approach, which routinely necessitates general anesthesia, nasopharyngeal intubation, and hospital stay for observation [11, 12, 13, 14, 15]. Anterolateral approach for C2 biopsy also needs general anesthesia or at least sedation. General anesthesia has its own risks and might not be suitable for general debilitated patients. The posterolateral percutaneous CT-guided approach for C2 a biopsy can be done under local anesthesia. With the posterolateral approach, there is a risk of injury to the vertebral artery and spinal cord. Before the procedure, it is must review axial MRI images carefully to see the course of the vertebral artery and position of the cervical canal and to find a safe needle trajectory to avoid injuring vertebral arteries and spinal cord during the procedure. Cox et al. reported 43 cases of CT-guided biopsy of the cervical spine. Of the 43 lesions biopsied, they used posterior or posterolateral approach in 26 cases (60%), lateral in 9 cases (21%), and anterolateral in 6 cases (14%). Whenever feasible they preferred the posterior approach as it avoids major neurovascular structures. They also reported most common lesions biopsied were malignant, measuring 13 of 43 (30%). The C2 and the C4 vertebral levels were the most common sites of lesions with five cases each (23%) [7]. In 2004, Lis et al. studied the diagnostic yield of CT-guided spine biopsies in 410 lesions, of which nine were in the cervical spine (2% of 410 sample size). They reported a success rate of 100% for the nine cervical spine lesions biopsied. Lis et al. so mentioned five patients that were negative for tumor but proved to be infectious with culture or histologic findings. Two were bacterial and two fungal, with one lesion, determined to be tuberculosis. One patient had superimposed bacterial infection with metastatic esophageal carcinoma [16]. Hence to emphasize confirming or excluding metastasis or infection in a patient with a known primary tumor. In 1992 Brugieres et al. reported recurrent laryngeal nerve dysfunction in three of 12 patients (25%) biopsied with CT guidance for cervical bone, all of which resolved on follow-up [17]. Peh et al. in 2006, reported low complication rates with CT-guided biopsies of the spine, varying from 0% to 10%, with <1% risk of major complication [18]. Huang et al. in 2013, reported the incidence of complications following CT-guided biopsies of spinal lesions of bruising, level of discomfort/pain, and fever was <16.1% in any category of the 386 patients studied [19]. Fraser-Hill et al. discussed and Cox et al. reported cost-effectiveness of Percutaneous CT-guided biopsy compared with open biopsies [7, 20]. This case reports that the minimally invasive posterolateral percutaneous CT-guided approach for C2 biopsy is safe, precise, accurate, and cost-effective.
Understanding the detailed anatomy prior to CT guided minimally invasive percutaneous C2 biopsy procedure helps in increasing its safety, precision, and high yield. Stepwise approach to the procedure aids in getting repeatable and high-yielding results, especially in technically challenging areas like C2 vertebrae.
Minimally invasive CT-guided percutaneous C2 biopsy by posterolateral approach is technically demanding but can be used safely, precisely, cost-effectively with the high field.
References
- 1.1. Robertson RC, Ball RP. Destructive spinal lesions: Diagnosis by needle biopsy. J Bone Joint Surg 1935;17:749-58. [Google Scholar]
- 2.2. Gupta S, Henningsen JA, Wallace MJ, Madoff DC, Morello FA Jr., Ahrar K, et al. Percutaneous biopsy of head and neck lesions with CT guidance: Various approaches and relevant anatomic and technical considerations. Radiographics 2007;27:371-90. [Google Scholar]
- 3.3. Ghelman B, Lospinuso MF, Levine DB, O’Leary PF, Burke SW. Percutaneous computed-tomography-guided biopsy of the thoracic and lumbar spine. Spine (Phila Pa 1976) 1991;16:736-9. [Google Scholar]
- 4.4. Schratter M. CT-guided percutaneous biopsy in orthopedics. Indications-planning-technic-personal experiences, with special reference to the spine. Radiologe 1990;30:201-13. [Google Scholar]
- 5.5. Valls J, Ottolenghi CE, Schajowicz F. Aspiration biopsy in diagnosis of lesions of vertebral bodies. J Am Med Assoc 1948;136:376-82. [Google Scholar]
- 6.6. Sun HY, Lee JW, Kim KJ, Yeom JS, Kang HS. Percutaneous intervention of the C2 vertebral body using a CT-guided posterolateral approach. AJR Am J Roentgenol 2009;193:1703-5. [Google Scholar]
- 7.7. Cox M, Pukenas B, Poplawski M, Bress A, Deely D, Flanders A. CT-guided cervical bone biopsy in 43 patients: Diagnostic yield and safety at two large tertiary care hospitals. Acad Radiol 2016;23:1372-5. [Google Scholar]
- 8.8. Rimondi E, Staals E, Errani C, Bianchi G, Casadei R, Alberghini M, et al. Percutaneous CT-guided biopsy of the spine: Results of 430 biopsies. Eur Spine J 2008;17:975-81. [Google Scholar]
- 9.9. Kornblum MB, Wesolowski DP, Fischgrund JS, Herkowitz HN. Computed tomography-guided biopsy of the spine. A review of 103 patients. Spine (Phila Pa 1976) 1998;23:81-5. [Google Scholar]
- 10.10. Kattapuram S, Rosenthal D. Percutaneous biopsy of the cervical spine using CT guidance. AJR Am J Roentgenol 1987;149:539-41. [Google Scholar]
- 11.11. Kaltsikis I, Chourmouzi D, Drevelegas K, Potsi S, Moumtzouoglou A, Drevelegas A. Core needle biopsy of spinal lesions under CT guidance: Review of 79 cases. J Neurol Surg A Cent Eur Neurosurg 2012;73:199-203. [Google Scholar]
- 12.12. Brugieres P, Revel MP, Dumas JL, Heran F, Voisin MC, Gaston A. CT-guided vertebral biopsy: A report of 89 cases. J Neuroradiol 1991;18:351-9. [Google Scholar]
- 13.13. Adapon BD, Legada BD Jr., Lim EV, Silao JV Jr., Dalmacio-Cruz A. CT-guided closed biopsy of the spine. J Comput Assist Tomogr 1981;5:73-8. [Google Scholar]
- 14.14. Kang M, Gupta S, Khandelwal N, Shankar S, Gulati M, Suri S. CT-guided fine-needle aspiration biopsy of spinal lesions. Acta Radiol 1999;40:474-8. [Google Scholar]
- 15.15. Ippolito V, Saccalani M, Pavia M, Brembilla R, Motta C. CT-guided percutaneous trochar-biopsy of the spine. Chir Organi Mov 1998;83:7-13. [Google Scholar]
- 16.16. Lis E, Bilsky M, Pisinski L, Boland P, Healey JH, O’malley B, et al. Percutaneous CT-guided biopsy of osseous lesion of the spine in patients with known or suspected malignancy. AJNR Am J Neuroradiol 2004;25:1583-8. [Google Scholar]
- 17.17. Brugieres P, Gaston A, Voisin MC, Ricolfi F, Chakir N. CT-guided percutaneous biopsy of the cervical spine: A series of 12 cases. Neuroradiology 1992;34:358-60. [Google Scholar]
- 18.18. Peh W. CT-guided percutaneous biopsy of spinal lesions. Biomed Imaging Interv J 2006;2:e25. [Google Scholar]
- 19.19. Huang A, Halpern E, Rosenthal DI. Incidence of delayed complications following percutaneous CT-guided biopsy of bone and soft tissue lesions of the spine and extremities: A 2-year prospective study and analysis of risk factors. Skeletal Radiol 2013;42:61-8. [Google Scholar]
- 20.20. Fraser-Hill M, Renfrew D, Hilsenrath P. Percutaneous needle biopsy of musculoskeletal lesions. 2. Cost-effectiveness. AJR Am J Roentgen 1992;158:813-8. [Google Scholar]






