
GHN with Atraditional positioning causes scarcity of space available for the surgeon, assistant, scrub nurse, X-ray technician, risks while performing distal interlocking which are addressed by Novel room Set up called ‘Jahwari’s Position’.
Dr. Ahmed Jahwari, Senior consultant Spine surgery, Head of Department Orthopedics, Armed Forces Hospital, Oman. MD. FRCSC. E-mail: ahmedaljahwari111@gmail.com
Abstract
Introduction: Ante Grade Humeral Nailing (AGHN) with traditional positioning causes crowding at the patient's head end, cramming for the surgeon and anaesthetist, scarcity of space available for the scrub nurse and X-ray technician, and neurovascular risks while performing distal interlocking. Minimal literature is available regarding the optimal position and set up in the operating theatre (OT). The primary objective was to describe, how effective novel Jahwari’s position is by assessing the ergonomics for OT personnel, OT time, and radiation exposure. A secondary objective was to evaluate the safety of inserting distal interlocking screws.
Case Report: The head of the patient is placed away from the anaesthetist and their equipment, which were placed at the foot end of the patient. The patients were connected to the anaesthesia machine with a long airway extension, which was anchored to the table. The C arm machine was brought from the contralateral side and did not have to be moved. The scrub nurse and the surgeon were placed at the head end of the patient. Pregnant patients, those aged <18 years, and those with open fractures were excluded from our study. A single consultant operated on all cases for standardization. OT time and radiation exposure were monitored.
Conclusion: Inspired by our use of this position for cervical spine patients for more than a decade, Jahwari’s position and setup were innovated. This setup gives ample room for the anaesthetist at the foot end. The surgeon and assistants are free from cramming at the head end. Complementarily, it provides ample space for the X-ray technician and scrubs nurse.
Keywords: Jahwari position, antegrade humeral nailing, modified lateral position.
An optimized OT setup improves patient and surgical team outcomes. Various patient positioning techniques have been described for antegrade humeral nailing (AGHN), with their respective difficulties and benefits. These positions include the beach chair, supine, and traditional lateral positions. The OT layout remains the same with all these positions; only the patient’s positioning changes. With these well-known positions and OT setup, several studies indicate multiple issues such as iatrogenic neurovascular injuries, difficulties of positioning patients with specific trauma, and crowding at one end. Yi et al. describe the difficulties with the lateral decubitus position, including draping of patients and positioning patients with thoracic and facial injuries and distal neurovascular injuries while performing humeral nailing [1]. Ikpeme et al. described the shoulder pain in the supine position and the associated distal neurovascular injuries, such as injury to the radial and axillary nerves [2]. This was also supported by the argument of Gadegone et al. about iatrogenic injury during distal interlocking [3]. Blyth et al. also studied the neurovascular risks in anteroposterior (AP) distal locking. Of 51 humeral shaft fractures repaired in the traditional position, 8 iatrogenic injuries occurred: 3 to the radial and 5 to the lateral cutaneous nerve. Therefore, they suggested posteroanterior distal locking to minimize such risks [4].
Traditional positions are associated with certain disadvantages. Setting up a patient in a beach chair position is time-consuming and cumbersome. During distal interlocking in the anteroposterior direction, there is a constant risk to neurovascular structures because of the presence of vital structures in the vicinity. Distal locking against a moving target is a challenge in this position [5,6].
Musculocutaneous nerve injury, ulnar nerve, axillary nerve, and common peroneal nerve injuries are well-known complications of lateral position [7].
Whereas in traditional supine or traditional lateral positions crowding and cramming at the head end remains an issue. In addition, in beach chair and supine positions less favorable anteroposterior distal locking is mandatory.
To overcome the challenges of traditional positioning, we adopted a modified layout coined as “Jahwari’s position.” We have been using this position in cervical spine patients for the past 10 years, as time-tested it is, we wanted to implement it in a trauma scenario also. With help of a long radiolucent extension, attached to the OT table central pillar with a head of the patient located away from the anaesthesia machine. The patient is connected to the anaesthesia machine with a long airway tube which is anchored at multiple points before it reaches the machine. Access to IV lines and physical monitoring is done by the anaesthetist from the foot end. This setup gives ample room for the anaesthetist at the foot end. Likewise, the surgeon is also free from cramming at the head end where they usually stand during the surgical procedure.
To the best of our knowledge, there is no description in the literature of the novel setup we are describing. The primary objective was to describe and find out the effectiveness of the novel room setup by assessing the ergonomics for OT personnel, OT time, and radiation exposure. A secondary objective was to evaluate the safety of inserting distal interlocking screws.
The patients were placed in a novel setup using Jahwari’s position with the head of the patient placed away from the anaesthetist and their equipment, which were placed at the foot end of the patient as shown in the clinical photo (Fig. 1) With help of the long radiolucent extension, attached to the OT table central pillar with the head of the patient located away from the anaesthesia machine. Metallic extension bars were used to extend the inbuilt bars from the main operating table. The patient is connected to the anaesthesia machine with a long airway tube which is anchored at multiple points before it reaches the machine. Access to IV lines and physical monitoring is done by the anaesthetist from the foot end. This setup gives ample room for the anesthetist at the foot end. Likewise, the surgeon is also free from cramming at the head end where they usually stand during the surgical procedure. Complementarily, it provides ample space for the X-ray technician and scrubs nurse.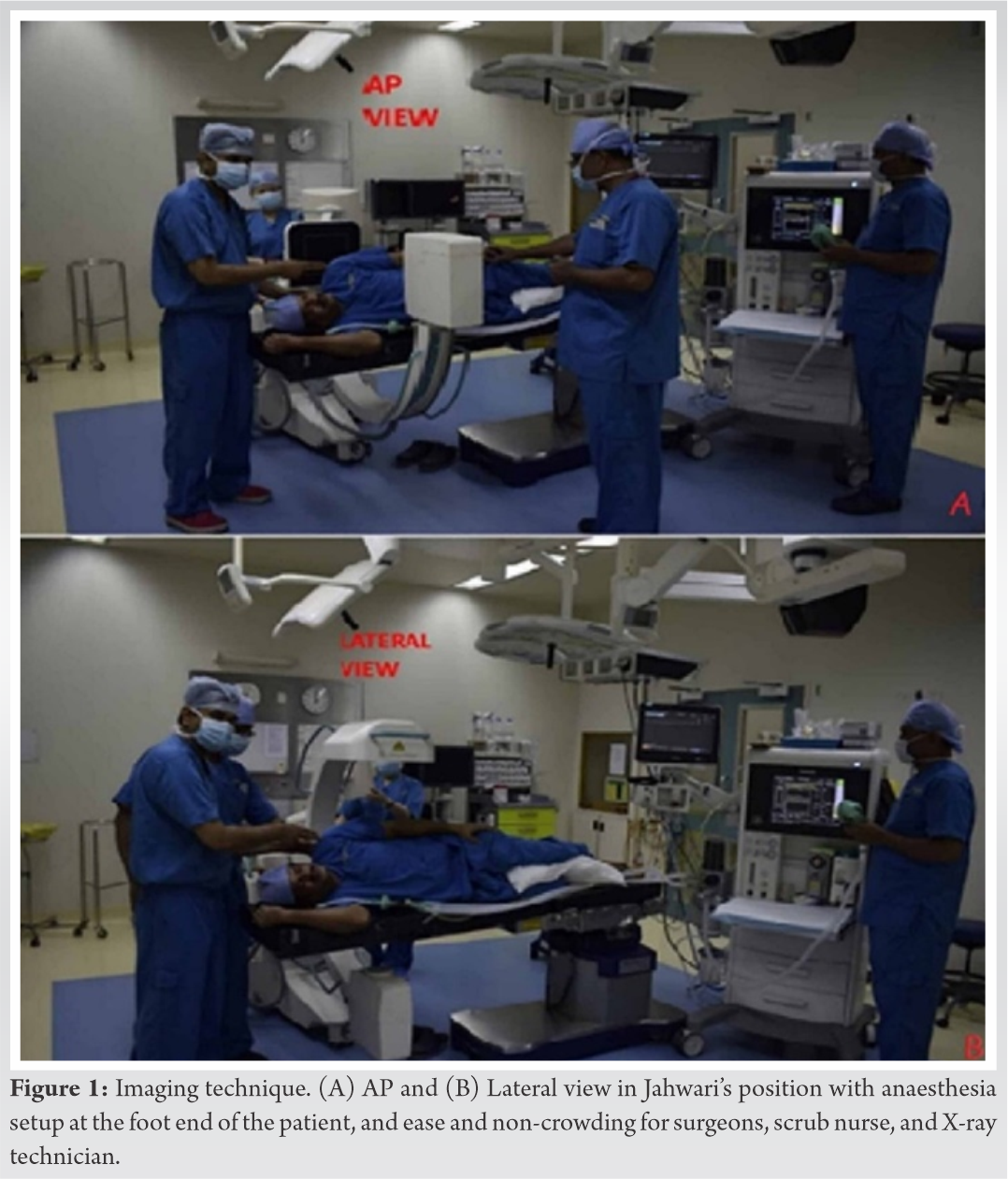
Operating table extensions used were mostly radiolucent with no inbuilt metallic extension bars. Side supports were mandatory to secure the patient in a lateral position. Metallic extension bars, which are supplied as accessories, were used in extending the inbuilt bars from the main operating table (Maquet Yuno, Getinge AB, Gothenburg, Sweden) to secure the patient in this position (Fig. 2).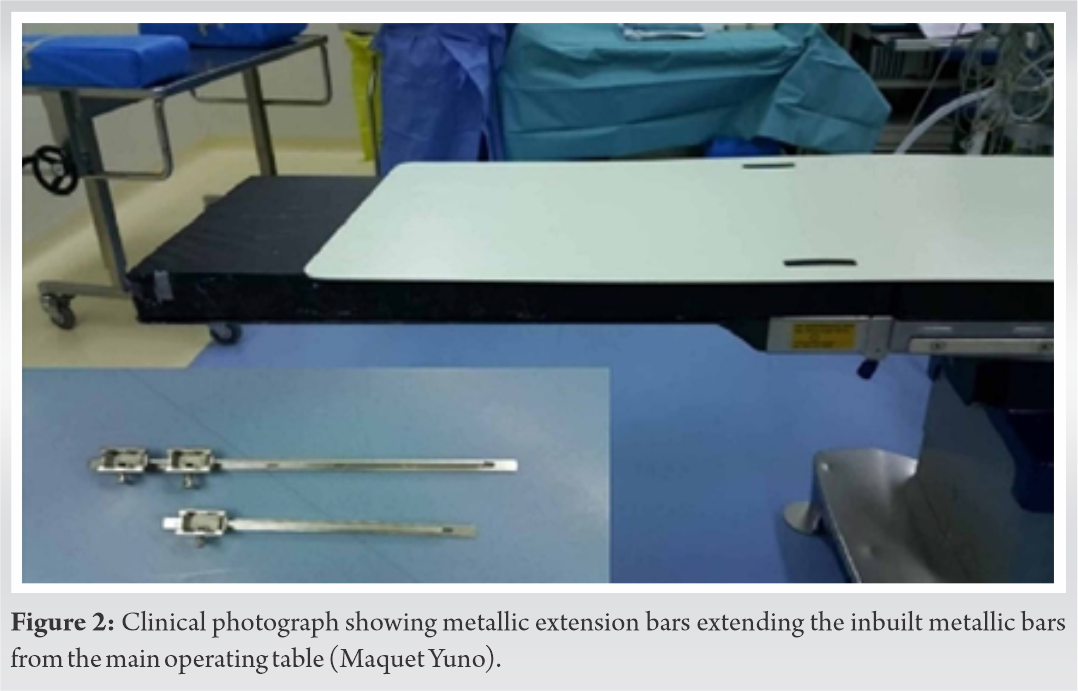
During the nailing procedure, horizontal C arm position gives an AP view of the shoulder, whereas while obtaining the lateral view overlap from the other shoulder is an issue. This can be combated by slightly tilting the patient either anteriorly or posteriorly to overcome the overlap from the opposite shoulder.
After the patient is positioned as described above, the surgical technique we did is as follows:
Antegrade humeral nailing
The clavicle, acromion, and coracoid process were identified and marked. The axillary nerve was approximately marked 5–7 cm distal to the angle of the acromion. Following the incision of the skin and subcutaneous tissues, the deltoid was split. Entry through the greater tuberosity is not recommended due to supraspinatus tendon injury. The entry point was thus through the rotator interval. A guidewire was passed, and sequential reaming was done.
After passing the nail over the guidewire and confirming its position with fluoroscopy, proximal locking was cautiously performed using the jig because of the proximity of the axillary nerve (Fig. 3).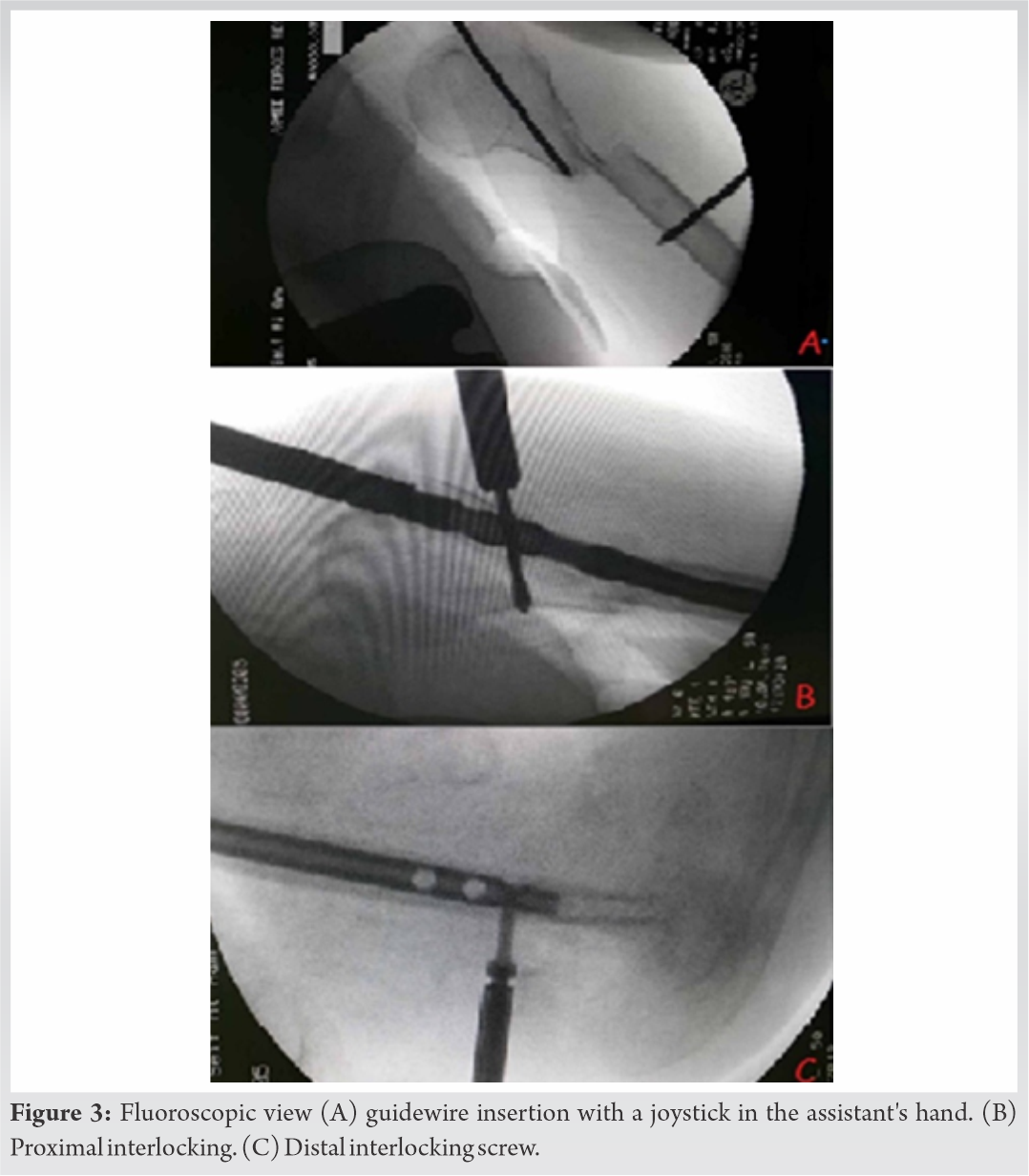 In traditional positions such as beach chair or supine, distal locking has to be performed anteroposterior, which poses more risk to the neurovascular structures; Whereas in Jahwari’s position or even in the traditional lateral position where posteroanterior distal locking was possible, the risk to neurovascular structures dramatically reduced as depicted in the schematic diagram (Fig. 4) and led to better ergonomics (Fig. 5)
In traditional positions such as beach chair or supine, distal locking has to be performed anteroposterior, which poses more risk to the neurovascular structures; Whereas in Jahwari’s position or even in the traditional lateral position where posteroanterior distal locking was possible, the risk to neurovascular structures dramatically reduced as depicted in the schematic diagram (Fig. 4) and led to better ergonomics (Fig. 5)
As far as OT time is concerned Jahwari’s position took 30 min less on average compared to other positions. Ninety percent of OT staff favoured the new position especially due to lack of hindrance from each other.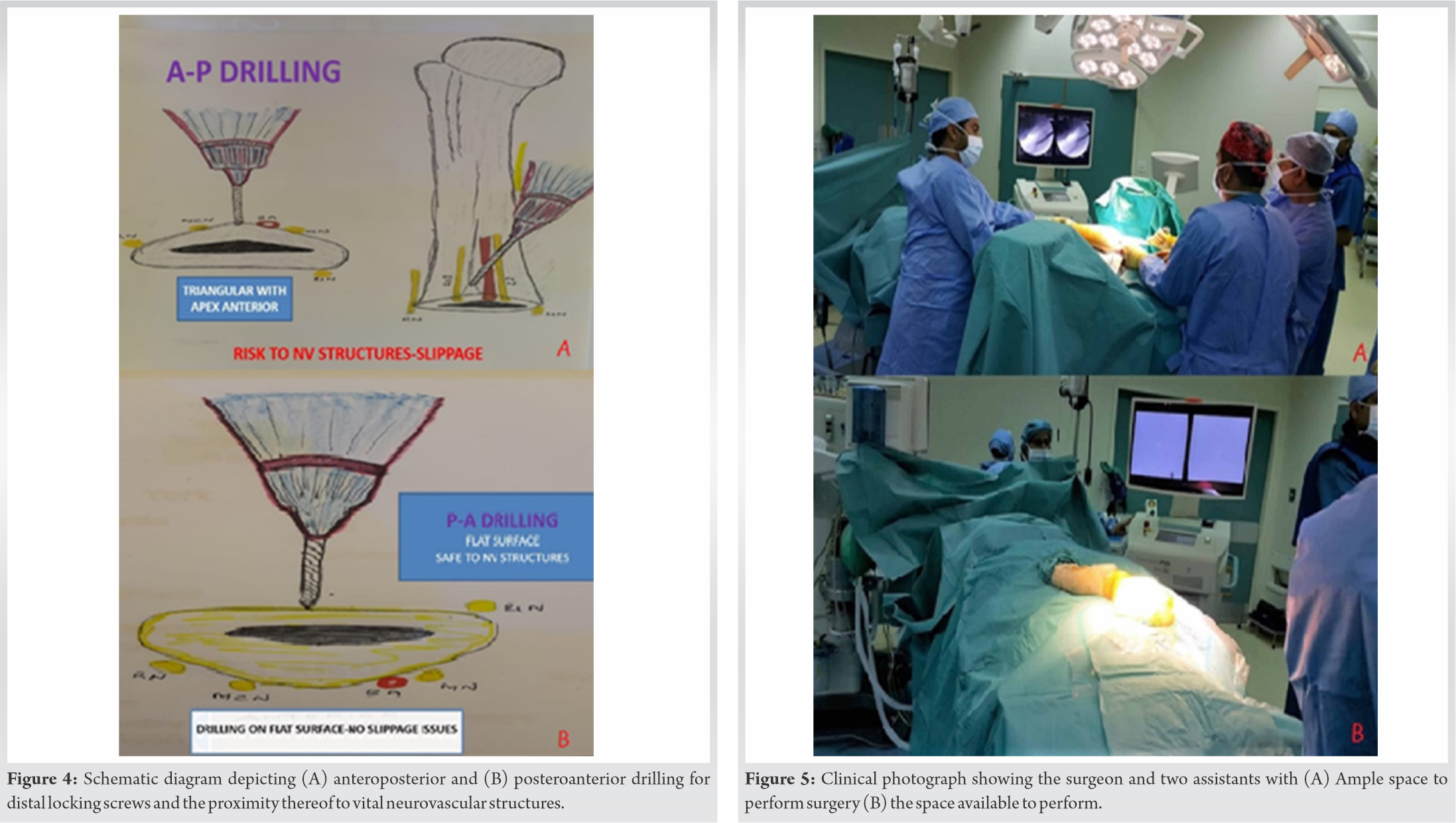
The operative time for the Jahwari’s position group ranged from 60 to 100 min (average 80 min). Reduced operative time and radiation exposure improve patient safety independently, not considering surgical risks.
Barbagello et al. debate how lack of optimization of the OT, arrangement, and flow leads to increased cost and disturbance in performing surgical procedures. They mention that most OTs are designed for elective setup, not emergencies, and concluded that OT optimization led to the best use of human resources and OT personnel, increased patient safety, and better surgical team outcomes [8]. Wong et al. emphasized three factors that could affect outcomes based on OT setup optimization, namely physical factors (noise and light), human factors of the patient or OT staff (ergonomics: patient and surgeon positioning), and surgeon-related factors (fatigue and stress). They mentioned that optimizing the OT would mean optimizing these factors, with better outcomes for the patient and surgeon [9].
The beach chair layout allows the surgeon to address multiple upper limb issues that may be associated with humeral shaft fractures, including shoulder dislocations and glenoid injuries.
However, the setup is time-consuming and cumbersome. AP distal locking poses constant risks to the neurovascular structures and is challenging against a moving target [5,10].
The traditional supine and lateral positions are preferred over the beach chair position for patient monitoring and safety. However, crowding at the head end remains problematic. Whereas, the latter position facilitates safe, posteroanterior distal interlocking, minimizing neurovascular risks [6].
All these disadvantages of traditional positions are obviated by our novel position including crowding at the head end. In addition, performing posteroanterior distal interlocking without neurovascular risk was an added benefit. Above 90% of staff favoured the novel position as mentioned in the results. Documented radiation exposure to the surgical team and patient was less compared to the traditional methods.
Distally, the humerus is triangular, with the apex pointing anteriorly when viewed in cross-section. This risks slippage of the drill bit at the apex during anteroposterior interlocking. In the beach chair position, this risk increases since the surgeon work on a moving target. Therefore, the lateral position (with posteroanterior distal locking screws), whether traditional or Jahwari’s position, is considered better.
Inspired by our use of this position for the past 10 years, as time tested and efficient it is – Jahwari’s position, with its associated layout, allows the anaesthetists, surgeons, scrub nurses, and C-arm technician to work comfortably. Furthermore, the risk of the X-ray technician contaminating the operative field is also minimized, with ample space available for manoeuvring the C-arm. Likewise, the scrub nurse has adequate space to keep trolleys uncontaminated. These factors reduce the OT time, patient and staff radiation exposure and allow posteroanterior insertion of distal locking screws in safe manner.
In our experience, optimizing the OT layout and positioning while performing AGHN has an impact on patient safety, comfort levels for all the members involved in the surgery, reducing OT time, and radiation exposure compared to traditional positions and layouts.
References
- 1.1. Yi JW, Lee JS, Cho HJ. Retrograde intramedullary nailing for humerus fracture in a supine position: Performing an unfamiliar procedure in a familiar position. Clin Orthop Surg 2017;9:392-5. [Google Scholar | PubMed]
- 2.2. Ikpeme JO. Intramedullary interlocking nailing. For humeral fractures: Experiences with the Russell-Taylor humeral nail. Injury 1994;25:447-55. [Google Scholar | PubMed]
- 3.3. Gadegone W, Gadegone P, Lokhande V. Humerus nailing in lateral position (operative technique). Open J Orthop 2020;10:33. [Google Scholar | PubMed]
- 4.4. Blyth MJ, Macleod CM, Asante DK, Kinninmonth AW. Iatrogenic nerve injury with the Russell-Taylor humeral nail. Injury 2003;34:227-8. [Google Scholar | PubMed]
- 5.5. White WJ, Hawken RM, Giles NC. Posterior to anterior distal locking of humeral intramedullary nails. Ann R Coll Surg Engl 2012;94:603. [Google Scholar | PubMed]
- 6.6. Liu N, Mohri T, Hayashi J, Orito R, Nakai T, Yoneda Y. A new rotator interval approach for antegrade humeral nailing: A technical note. Open J Orthop 2014;4:321. [Google Scholar | PubMed]
- 7.7. Li X, Eichinger JK, Hartshorn T, Zhou H, Matzkin EG, Warner JP. A comparison of the lateral decubitus and beach-chair positions for shoulder surgery: Advantages and complications. J Am Acad Orthop Surg 2015;23:18-28. [Google Scholar | PubMed]
- 8.8. Barbagallo S, Corradi L, de Goyet JD. Optimization and planning of operating theatre activities: An original definition of pathways and process modeling. BMC Med Inform Decis Mak 2015;15:38. [Google Scholar | PubMed]
- 9.9. Wong SW, Smith R, Crowe P. Optimizing the operating theatre environment. ANZ J Surg 2010;80:917-24. [Google Scholar | PubMed]
- 10.10. Baltov A, Mihail R, Dian E. Complications after interlocking intramedullary nailing of humeral shaft fractures. Injury 2014;45:9. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2021 Massive Eccentric Wear of the Acetabular Cup after Polyethylene Liner Abrasion in Hip Arthroplasty may lead to a high Risk of Injury during Revision Surgery
March 10, 2021 Massive Eccentric Wear of the Acetabular Cup after Polyethylene Liner Abrasion in Hip Arthroplasty may lead to a high Risk of Injury during Revision Surgery April 13, 2013 Acute Compressive Ulnar Neuropathy In A Patient Of Dengue Fever: An Unusual Presentation
April 13, 2013 Acute Compressive Ulnar Neuropathy In A Patient Of Dengue Fever: An Unusual Presentation May 23, 2018 Why there are so many submission, why the rush to publish?
May 23, 2018 Why there are so many submission, why the rush to publish? July 7, 2017 Temporary Fixation Using a Long Femoral-tibial Nail to Treat a Displaced Medial Tibial Plateau Fracture in a 90-year-old Patient: A Case Report
July 7, 2017 Temporary Fixation Using a Long Femoral-tibial Nail to Treat a Displaced Medial Tibial Plateau Fracture in a 90-year-old Patient: A Case Report