
In geriatric hip fracture surgery, multimodal opioid-sparing analgesia should be preferred over conventional opioid-based regimens, as it enhances pain control while improving safety, cognitive outcomes, and overall recovery.
Dr. Sukhil Raina, Department of Orthopaedics, Government Medical College and Hospital, Jammu and Kashmir, India. E-mail: sukhilraina99@gmail.com
Abstract
Introduction: Hip fracture surgery is frequently associated with severe post-operative pain, traditionally managed using opioid-based regimens. In elderly patients, opioids are linked to adverse effects such as delirium, respiratory depression, and delayed mobilization. Opioid-sparing multimodal analgesia, incorporating non-opioid medications and regional anesthesia techniques, has emerged as a promising alternative. This study aimed to compare the efficacy and safety of an opioid-sparing multimodal analgesia regimen with standard opioid-based analgesia in patients undergoing hip fracture surgery.
Materials and Methods: This prospective randomized controlled trial enrolled 50 patients aged ≥50 years undergoing operative management for hip fractures. Participants were randomized into two groups: Group M (multimodal analgesia, n = 25) and Group S (standard opioid-based analgesia, n = 25). Group M received scheduled non-opioid analgesics and a regional nerve block with opioids reserved for rescue, while Group S received conventional opioid-centered pain management. Post-operative pain was assessed using the Visual Analog Scale (VAS) at 2, 6, 12, 24, and 48 h. Total opioid consumption within 48 h, opioid-related adverse effects, incidence of delirium, time to first mobilization, length of hospital stay, and patient satisfaction were recorded.
Results: Baseline characteristics were comparable between groups. Group M demonstrated significantly lower VAS scores at all time points (e.g., 24 h: 2.2 ± 0.6 vs. 3.4 ± 0.8; P < 0.001) and reduced 48-h opioid consumption (9.6 ± 3.2 mg vs. 22.8 ± 5.6 mg; P < 0.001). Opioid-related adverse effects and post-operative delirium were significantly lower in Group M (12% vs. 36%; P = 0.04). Patients in Group M achieved earlier mobilization (27.4 ± 6.8 vs. 39.6 ± 9.2 h; P < 0.001) and had shorter hospital stays (6.1 ± 1.4 vs. 8.3 ± 2.0 days; P < 0.001). Patient satisfaction was higher in the multimodal group.
Conclusion: Opioid-sparing multimodal analgesia provides superior pain control with reduced opioid consumption and improved post-operative outcomes compared with standard analgesia in hip fracture surgery. Its routine adoption may enhance recovery and safety in this high-risk population.
Keywords: Hip fracture surgery, multimodal analgesia, opioid-sparing, post-operative pain, randomized controlled trial.
Hip fracture surgery represents one of the most common orthopedic emergencies worldwide, particularly among the elderly population, and is associated with substantial morbidity, mortality, and healthcare burden [1]. Patients sustaining hip fractures often experience severe acute pain that, if inadequately managed, contributes to delayed mobilization, prolonged hospital stay, increased risk of complications such as pneumonia, thromboembolism, delirium, pressure ulcers, and overall poorer functional recovery [2]. Effective post-operative analgesia is therefore a cornerstone of perioperative care in hip fracture patients. Conventionally, systemic opioids have been the mainstay of pain management in this population due to their potent analgesic effects and ease of administration [3]. However, older adults are especially vulnerable to opioid-related adverse effects, including respiratory depression, nausea and vomiting, constipation, urinary retention, pruritus, sedation, and cognitive dysfunction, with post-operative delirium being a particularly concerning complication linked to increased mortality and long-term functional decline [4]. These limitations have prompted growing interest in alternative strategies that provide adequate analgesia while minimizing opioid exposure.
Multimodal analgesia, which combines agents and techniques acting through different mechanisms along the nociceptive pathway, has emerged as a promising approach to optimize pain control and reduce opioid requirements [5]. Such regimens typically incorporate non-opioid systemic medications such as acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), -2 inhibitors, and gabapentinoids, along with regional anesthesia techniques including peripheral nerve blocks and local infiltration analgesia [6]. By targeting multiple pain pathways simultaneously, multimodal analgesia aims to achieve superior analgesic efficacy with lower doses of individual drugs, thereby reducing the incidence of adverse effects [7]. In the context of hip fracture surgery, regional techniques such as femoral nerve block, fascia iliaca compartment block, and pericapsular nerve group (PENG) block have demonstrated significant opioid-sparing effects and improved early post-operative comfort [8].
Moreover, early mobilization, a key determinant of functional recovery and survival after hip fracture, is facilitated by effective analgesia that does not compromise sensorium or motor function [9]. Despite accumulating evidence supporting the benefits of multimodal, opioid-sparing strategies in elective orthopedic procedures, their role in emergency hip fracture surgery remains inadequately defined. Many institutions continue to rely on conventional opioid-centered regimens due to logistical constraints, limited availability of trained personnel for regional anesthesia, and variability in clinical practice [10]. Furthermore, existing studies often differ in analgesic protocols, outcome measures, and patient populations, making it difficult to draw definitive conclusions regarding the optimal pain management strategy for this high-risk group. Given the increasing global incidence of hip fractures with population aging and the heightened emphasis on enhanced recovery pathways, there is a critical need for high-quality randomized controlled trials comparing opioid-sparing multimodal analgesia with standard opioid-based regimens in hip fracture surgery. Such trials are essential to evaluate not only pain scores and opioid consumption but also clinically meaningful outcomes including incidence of delirium, post-operative complications, time to mobilization, length of hospital stay, patient satisfaction, and functional recovery. Establishing evidence-based analgesic protocols tailored to the unique physiological vulnerabilities of elderly hip fracture patients has the potential to improve perioperative safety, enhance recovery, and reduce healthcare burden. Against this background, the present randomized controlled trial is designed to compare the efficacy and safety of an opioid-sparing multimodal analgesia regimen with standard analgesia in patients undergoing hip fracture surgery, with the aim of determining whether a multimodal approach can provide equivalent or superior pain relief while minimizing opioid-related adverse effects and improving post-operative outcomes.
Cyclooxygenase-2
Study design
This study was conducted as a prospective, randomized, controlled, parallel-group clinical trial designed to compare the efficacy and safety of an opioid-sparing multimodal analgesia regimen with standard opioid-based analgesia in patients undergoing hip fracture surgery. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Study setting
The study was carried out in the Department of Orthopedics and Anesthesiology of a tertiary care teaching hospital.
Study duration
The study was conducted over a period of 12 months, from January 2025 to December 2025. This duration allowed adequate recruitment of participants, uniform application of interventions, and follow-up for post-operative outcomes during the hospital stay.
Participants
Inclusion criteria
- Patients aged ≥50 years
- Diagnosed with unilateral hip fracture (intertrochanteric, femoral neck, or subtrochanteric)
- Planned for operative management (hemiarthroplasty, total hip arthroplasty, or internal fixation)
- Classified as American Society of Anesthesiologists (ASA) physical status I–III
- Provided written informed consent
Exclusion criteria
- Polytrauma patients
- Pathological fractures
- Known allergy or contraindication to study medications
- Chronic opioid use or opioid dependence
- Severe cognitive impairment precluding pain assessment
- Severe hepatic or renal dysfunction
- Coagulopathy or contraindication to regional anesthesia.
Study sampling
A consecutive sampling method was adopted. All eligible patients presenting with hip fractures during the study period were screened for inclusion. Those fulfilling the eligibility criteria and providing informed consent were enrolled until the required sample size was achieved. This approach ensured feasibility in an emergency surgical setting while maintaining representativeness of the target population.
Study sample size
The total sample size was fixed at 50 participants. Based on feasibility and departmental surgical volume, 50 patients were enrolled and randomly allocated into two equal groups of 25 each. This sample size was considered adequate to demonstrate clinically meaningful differences in post-operative pain scores and opioid consumption between groups within the available study period.
Study groups
Participants were randomly allocated using a computer-generated randomization sequence into two groups:
- Group M (multimodal analgesia group, n = 25): Patients received an opioid-sparing multimodal analgesia regimen comprising pre-operative and post-operative paracetamol, NSAIDs or COX-2 inhibitors (where not contraindicated), and a regional nerve block (fascia iliaca or PENG block) administered perioperatively, with opioids reserved only as rescue analgesia.
- Group S (standard analgesia group, n = 25): Patients received conventional opioid-based analgesia, consisting of intravenous opioids in the perioperative period along with routine post-operative opioid administration as per institutional protocol.
Study parameters
The primary outcome parameters included post-operative pain intensity measured using the Visual Analog Scale (VAS) at pre-defined intervals and total opioid consumption within the first 48 h. Secondary parameters included incidence of post-operative delirium, occurrence of opioid-related adverse effects (nausea, vomiting, sedation, and respiratory depression), time to first mobilization, length of hospital stay, and patient satisfaction with pain control.
Study procedure
After enrollment, baseline demographic and clinical data were recorded. Participants were randomized into either Group M or Group S. All patients underwent standard pre-operative evaluation and were optimized for surgery. Anesthetic technique (spinal or general anesthesia) was standardized across both groups. In Group M, a regional nerve block was administered preoperatively or immediately postoperatively by an experienced anesthesiologist, and non-opioid analgesics were initiated according to protocol. In Group S, analgesia relied primarily on systemic opioids as per routine practice. Postoperatively, patients were monitored in the recovery unit and then transferred to the orthopedic ward. Pain management followed the assigned group protocol throughout the hospital stay.
Study data collection
Data were collected using a structured case record form. Pain scores were recorded at 2, 6, 12, 24, and 48 h postoperatively using the VAS. Opioid consumption was documented in morphine-equivalent doses. Patients were assessed daily for signs of delirium using a standardized screening tool. Adverse events and complications were recorded prospectively. Time to first assisted ambulation and total length of hospital stay were documented. Patient satisfaction with analgesia was assessed on post-operative day 2 using a Likert scale.
Data analysis
Data were entered into a spreadsheet and analyzed using statistical software. Continuous variables were expressed as mean ± standard deviation, while categorical variables were presented as frequencies and percentages. Intergroup comparisons of continuous variables were performed using the independent t-test or Mann–Whitney U test as appropriate. Categorical variables were compared using the Chi-square test or Fisher’s exact test. A P < 0.05 was considered statistically significant. The analysis followed the intention-to-treat principle.
A total of 50 patients were enrolled and randomized equally into Group M (multimodal analgesia) and Group S (standard opioid-based analgesia), with 25 patients in each group.
Baseline characteristics
Both groups were comparable with respect to demographic and clinical variables. The mean age was 71.4 ± 8.2 years in Group M and 72.1 ± 7.9 years in Group S (P = 0.74). Sex distribution was similar (14/11 male/female in Group M vs. 13/12 in Group S; P = 0.78). Mean body mass index did not differ significantly between groups (23.6 ± 3.1 vs. 24.1 ± 3.4 kg/m2; P = 0.56). ASA physical status distribution (I/II/III) was comparable (5/14/6 vs. 6/13/6; P = 0.93), as was fracture type distribution (IT/FN/ST: 12/9/4 vs. 11/10/4; P = 0.95). These findings confirm adequate randomization and baseline homogeneity.
Intraoperative characteristics
Operative duration was comparable between the two groups (86.2 ± 14.5 min in Group M vs. 88.9 ± 15.1 min in Group S; P = 0.52). The proportion of patients receiving spinal versus general anesthesia was similar (18/7 vs. 17/8; P = 0.77). However, intraoperative opioid consumption was significantly lower in Group M (4.1 ± 1.3 mg morphine equivalents) compared to Group S (7.6 ± 2.0 mg; P < 0.001), demonstrating an early opioid-sparing effect.
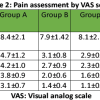
Post-operative pain scores
Group M consistently demonstrated significantly lower VAS pain scores at all post-operative time intervals (Table 1 and Fig. 1). At 2 h, mean VAS scores were 3.2 ± 0.9 in Group M versus 4.8 ± 1.1 in Group S (P < 0.001). Similar statistically significant differences were observed at 6 h (2.9 ± 0.8 vs. 4.3 ± 1.0), 12 h (2.6 ± 0.7 vs. 3.9 ± 0.9), 24 h (2.2 ± 0.6 vs. 3.4 ± 0.8), and 48 h (1.9 ± 0.5 vs. 2.9 ± 0.7), all with P < 0.001.
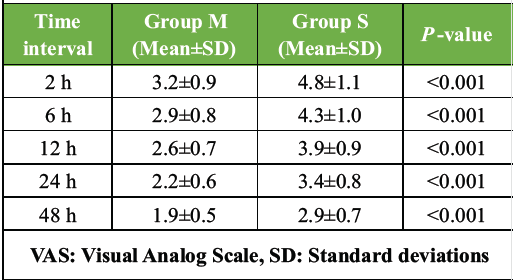
Table 1: Post-operative pain scores (VAS)
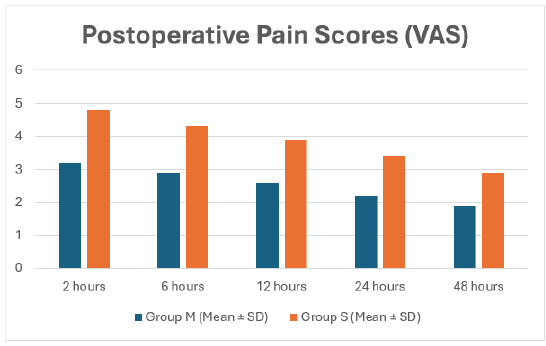
Figure 1: Patients in Group M consistently reported significantly lower pain scores at all time points, confirming the superior analgesic efficacy of multimodal analgesia.
Total opioid consumption
Total opioid consumption during the first 48 post-operative hours was significantly lower in Group M (9.6 ± 3.2 mg morphine equivalents) compared to Group S (22.8 ± 5.6 mg; P < 0.001) (Table 2), confirming a substantial opioid-sparing benefit.
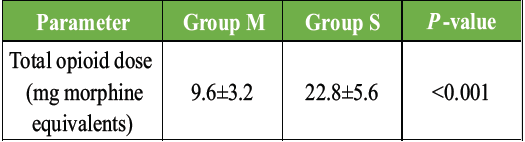
Table 2: Total opioid consumption (first 48 h)
Opioid-related adverse effects
The incidence of opioid-related side effects was significantly higher in Group S. Nausea/vomiting occurred in 4 patients (16%) in Group M versus 11 patients (44%) in Group S (P = 0.03). Excessive sedation was observed in 2 patients (8%) in Group M and 9 patients (36%) in Group S (P = 0.02). Constipation was reported in 5 patients (20%) in Group M and 13 patients (52%) in Group S (P = 0.02). Respiratory depression occurred in 3 patients (12%) in Group S and none in Group M, although this difference did not reach statistical significance (P = 0.07) (Fig. 2).
Post-operative delirium
Post-operative delirium was significantly less frequent in Group M (3 patients, 12%) compared to Group S (9 patients, 36%) (P = 0.04), suggesting a cognitive benefit associated with reduced opioid exposure.
Functional recovery
Time to first mobilization was significantly shorter in Group M (27.4 ± 6.8 h) compared to Group S (39.6 ± 9.2 h; P < 0.001) (Table 3), indicating enhanced early functional recovery.
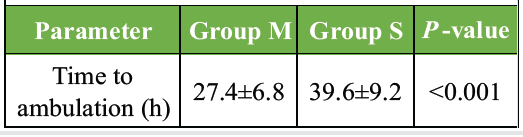
Table 3: Time to first mobilizations
Length of hospital stay
The mean length of hospital stay was significantly reduced in the multimodal group (6.1 ± 1.4 days) compared to the standard analgesia group (8.3 ± 2.0 days; P < 0.001), reflecting faster overall recovery and decreased healthcare utilization.
Rescue analgesia requirement
A significantly lower proportion of patients in Group M required rescue opioid analgesia (7 patients, 28%) compared to Group S (19 patients, 76%; P < 0.001) (Table 4). In addition, the mean number of rescue doses was significantly lower in Group M (1.1 ± 0.6) versus Group S (3.4 ± 1.2; P < 0.001).
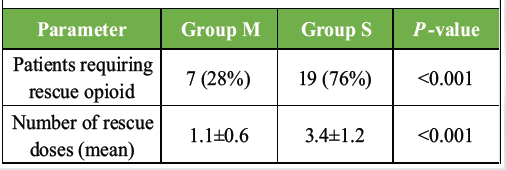
Table 4: Requirement of rescue analgesia
Patient satisfaction
Patient satisfaction scores favored the multimodal analgesia group. In Group M, 15 patients reported being very satisfied and 8 satisfied, compared to 6 very satisfied and 10 satisfied in Group S. Dissatisfaction was reported by 3 patients in Group S and none in Group M. The difference in satisfaction levels was statistically significant (P = 0.002).
Overall, multimodal analgesia demonstrated superior analgesic efficacy, significant opioid-sparing effects, fewer opioid-related adverse events, reduced delirium incidence, earlier mobilization, shorter hospital stay, and higher patient satisfaction compared to standard opioid-based analgesia.
The present randomized controlled trial demonstrated that an opioid-sparing multimodal analgesia regimen provided superior post-operative outcomes compared with standard opioid-based analgesia in patients undergoing hip fracture surgery. Both groups in the present study were comparable at baseline with respect to age (71.4 ± 8.2 vs. 72.1 ± 7.9 years), sex distribution, ASA status, and fracture pattern, confirming adequate randomization and minimizing baseline confounding. Despite similar operative duration (86.2 ± 14.5 vs. 88.9 ± 15.1 min) and anesthetic techniques, the multimodal group required significantly lower intraoperative opioids (4.1 ± 1.3 vs. 7.6 ± 2.0 mg morphine equivalents, P < 0.001), indicating an early opioid-sparing effect. This benefit persisted postoperatively, with consistently lower VAS scores at all measured intervals. At 2 h, pain scores were 3.2 ± 0.9 in the multimodal group versus 4.8 ± 1.1 in the standard group; at 24 h, 2.2 ± 0.6 versus 3.4 ± 0.8; and at 48 h, 1.9 ± 0.5 versus 2.9 ± 0.7, all showing highly significant differences (P < 0.001). These findings indicate that multimodal analgesia not only reduces opioid exposure but also achieves superior and sustained pain control. Total opioid consumption over 48 h was markedly lower in the multimodal group (9.6 ± 3.2 mg vs. 22.8 ± 5.6 mg, P < 0.001), representing more than a 50% reduction. This substantial decrease is clinically important in elderly hip fracture patients, who are particularly vulnerable to opioid-related adverse effects. In the present study, nausea and vomiting occurred in 16% of multimodal patients compared with 44% in the standard group, excessive sedation in 8% versus 36%, and constipation in 20% versus 52%. Although respiratory depression was observed only in the standard group (12%), the difference did not reach statistical significance, likely due to the limited sample size. These findings emphasize the safety advantage of opioid-sparing strategies. A particularly important observation was the significantly lower incidence of post-operative delirium in the multimodal group (12% vs. 36%, P = 0.04), a complication strongly associated with poor outcomes after hip fracture surgery. Reduced opioid exposure, improved pain control, and less sedation likely contributed to better cognitive stability. Functional recovery also favored the multimodal approach, with earlier ambulation (27.4 ± 6.8 vs. 39.6 ± 9.2 h, P < 0.001) and shorter hospital stay (6.1 ± 1.4 vs. 8.3 ± 2.0 days, P < 0.001), reflecting faster recovery and reduced healthcare burden. The need for rescue analgesia further highlighted the effectiveness of multimodal pain control, as only 28% of patients in the multimodal group required rescue opioids compared with 76% in the standard group, with fewer rescue doses (1.1 ± 0.6 vs. 3.4 ± 1.2, P < 0.001). Patient satisfaction mirrored these objective benefits, with a greater proportion of patients in the multimodal group reporting being “very satisfied” (15 vs. 6). These findings align with and extend observations from prior studies. Padilla et al. [11] reported that an opioid-sparing protocol in total hip arthroplasty significantly reduced inpatient opioid consumption (14.6 ± 16.7 vs. 25.7 ± 18.8 /day, P < 0.001) and post-discharge opioid use (13.9 ± 24.2 vs. 80.1 ± 55.9 MME, P < 0.001), while maintaining equivalent pain scores and patient-reported outcomes compared with traditional protocols. Although Padilla et al. [11] found no significant difference in VAS trajectories between cohorts (P = 0.463), the present study demonstrated significantly lower pain scores at all post-operative time points. This difference may reflect the emergency nature of hip fracture surgery and the higher baseline pain burden in this population, where regional techniques and structured multimodal regimens exert a more pronounced analgesic benefit. The magnitude of opioid reduction in the present study (9.6 vs. 22.8 mg in 48 h) is consistent with the substantial reductions reported by Padilla et al., [11] reinforcing the concept that opioid-sparing strategies can meaningfully decrease opioid exposure without compromising analgesia. Lim et al. [12] conducted a large retrospective comparative study of hip fracture patients and demonstrated that implementation of a standardized multimodal protocol resulted in lower post-operative pain scores (6-h VAS 1.9 vs. 2.9; 24-h 2.0 vs. 2.4; 48-h 1.7 vs. 2.2; all P ≤ 0.001) and reduced 48-h opioid use (5.5 vs. 13.3 mg, P = 0.014). These values closely parallel the findings of the present trial, where 48-h pain scores were 1.9 versus 2.9 and opioid consumption was 9.6 versus 22.8 mg. The congruence between these datasets strengthens the external validity of the present findings and supports the adoption of multimodal analgesia as a standard of care in geriatric hip fracture patients.
Stone et al., [13] demonstrated that isolated substitution of intravenous acetaminophen for oral acetaminophen did not reduce opioid utilization and was associated with slightly higher opioid use, increased costs, and higher naloxone use. Their results underscore that opioid-sparing analgesia is not achieved through a single pharmacologic change but requires a comprehensive, protocol-driven multimodal strategy incorporating regional anesthesia and systematic non-opioid adjuncts. The present study, which integrated regional blocks and scheduled non-opioid medications, achieved meaningful reductions in opioid use and adverse effects, illustrating the importance of a holistic approach rather than reliance on a single agent. Chassery et al. [14] compared opioid-free anesthesia with opioid-sparing anesthesia in day-case total hip arthroplasty and found no difference in 24-h opioid consumption (12 [0–25] vs. 16 [0–30] mg, P = 0.7) and similar pain scores and recovery profiles. These findings suggest that complete intraoperative avoidance of opioids does not necessarily confer additional benefit over opioid-sparing strategies. In contrast, the present study demonstrated that a pragmatic multimodal regimen, rather than absolute opioid elimination, yields clinically significant improvements in pain, opioid consumption, and functional recovery in a frail emergency surgical population.
Feng et al. [15] similarly reported that implementation of an opiate-sparing protocol in primary total hip arthroplasty reduced total opioid use (75.55 ± 121.07 vs. 57.10 ± 87.48 MME, P < 0.001) while maintaining comparable pain scores and functional outcomes. Although Feng et al. [15] noted statistically significant differences in early pain scores, these were not clinically meaningful, reinforcing that the primary value of opioid-sparing protocols lies in reducing opioid burden without compromising analgesia. The present trial advances this concept by demonstrating that, in hip fracture surgery, multimodal analgesia can achieve both reduced opioid consumption and superior pain control, likely due to the high nociceptive load and vulnerability of this patient group. Collectively, the present findings, when viewed alongside prior evidence, suggest that multimodal analgesia is particularly advantageous in hip fracture surgery, where pain is severe, patients are elderly, and the risks of opioid-related morbidity are substantial. Unlike elective arthroplasty populations, hip fracture patients often present with acute pain, limited physiological reserve, and high susceptibility to delirium, making the benefits of opioid minimization more clinically apparent. The reduction in delirium from 36% to 12%, earlier mobilization by over 12 h, and shortening of hospital stay by more than 2 days observed in the present study highlight outcomes that extend beyond analgesia alone and influence survival, independence, and healthcare utilization. While limitations include the single-center design and modest sample size, the consistency of benefit across multiple clinically meaningful endpoints strengthens the conclusions. In summary, the present randomized trial demonstrates that opioid-sparing multimodal analgesia in hip fracture surgery achieves lower pain scores, markedly reduced opioid consumption, fewer adverse effects, reduced delirium, earlier mobilization, shorter hospital stay, and higher patient satisfaction compared with standard opioid-based analgesia. These results are concordant with and supported by existing literature, and they provide strong justification for integrating structured multimodal analgesic protocols into routine perioperative care for hip fracture patients.
Despite the promising findings, the present study has several limitations. The relatively small sample size (n = 50) may limit statistical power and generalizability, while the single-center design restricts external validity across different healthcare settings. The follow-up period was confined to the hospital stay, precluding assessment of long-term outcomes such as functional recovery, chronic pain, and late complications. Heterogeneity in surgical procedures (hemiarthroplasty, total hip arthroplasty, and internal fixation) may have introduced variability in pain and recovery profiles. In addition, the use of different regional anesthesia techniques (fascia iliaca and PENG blocks) could have influenced analgesic efficacy. The absence of double blinding introduces potential observer and patient bias, particularly in subjective measures such as pain scores and satisfaction. Functional outcomes were not assessed using standardized scoring systems like the Harris Hip Score, limiting the depth of recovery evaluation. The use of consecutive sampling and exclusion of patients with severe comorbidities or cognitive impairment may have introduced selection bias and reduced applicability to the broader geriatric population. Furthermore, no cost-effectiveness analysis was performed and minor variability in the multimodal analgesia protocol.
This randomized controlled trial demonstrates that an opioid-sparing multimodal analgesia regimen offers clear advantages over standard opioid-based analgesia in patients undergoing hip fracture surgery, providing superior and sustained pain relief while significantly reducing opioid consumption. The multimodal approach was associated with fewer opioid-related adverse effects, a lower incidence of post-operative delirium, earlier mobilization, shorter hospital stay, and higher patient satisfaction, all of which are critical determinants of recovery in the elderly hip fracture population. These findings underscore the clinical value of integrating regional anesthesia and non-opioid adjuncts into routine perioperative care and support the adoption of structured multimodal analgesic protocols as a safer and more effective standard for pain management in hip fracture surgery.
In geriatric hip fracture surgery, multimodal opioid-sparing analgesia should be preferred over conventional opioid-based regimens, as it enhances pain control while improving safety, cognitive outcomes, and overall recovery.
References
- 1. Varacallo M, Luo TD, Johanson NA. Total knee arthroplasty techniques. In: StatPearls. Treasure Island, FL, Florida: StatPearls Publishing; 2022. [Google Scholar] [PubMed]
- 2. Parvizi J, Miller AG, Gandhi K. Multimodal pain management after total joint arthroplasty. J Bone Joint Surg Am 2011;93:1075-84. [Google Scholar] [PubMed]
- 3. Politzer CS, Kildow BJ, Goltz DE, Green CL, Bolognesi MP, Seyler TM. Trends in opioid utilization before and after total knee arthroplasty. J Arthroplasty 2018;33:S147-53.e1. [Google Scholar] [PubMed]
- 4. Bedard NA, DeMik DE, Dowdle SB, Callaghan JJ. Trends and risk factors for prolonged opioid use after unicompartmental knee arthroplasty. Bone Joint J 2018;100-B Suppl 1:62-7. [Google Scholar] [PubMed]
- 5. Cornett E, Kaye A, Urman R, Hart BM, Chami A, Gayle JA, et al. Enhanced recovery pathways in orthopedic surgery. J Anaesthesiol Clin Pharmacol 2019;35:S35-9. [Google Scholar] [PubMed]
- 6. Halawi MJ, Grant SA, Bolognesi MP. Multimodal analgesia for total joint arthroplasty. Orthopedics 2015;38:e616-25. [Google Scholar] [PubMed]
- 7. World Health Organization. The World Medicines Situation 2011: Access to Controlled Medicines; 2011. Available from: https://www.who.int/publications/i/item/who-emp-mie-2011-2.4 [Last accessed on 2022 Dec 19]. [Google Scholar] [PubMed]
- 8. Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg 1993;77:1048-56. [Google Scholar] [PubMed]
- 9. Chou R, Gordon DB, De Leon-Casasola OA, Rosenberg JM, Bickler S, Brennan T, et al. Management of postoperative pain: A clinical practice guideline from the American pain society, the American society of regional anesthesia and pain medicine, and the American society of anesthesiologists’ committee on regional anesthesia, executive committee, and administrative council. J Pain 2016;17:131-57. Erratum in: J Pain 2016;17:508-10. [Google Scholar] [PubMed]
- 10. Rakowski JA, Holloway RW, Ahmad S, Jeppson CN, James JA, Ghurani GB, et al. A prospective randomized trial of intravenous ketorolac vs. Acetaminophen administered with opioid patient-controlled analgesia in gynecologic surgery. Gynecol Oncol 2019;155:468-72. [Google Scholar] [PubMed]
- 11. Padilla JA, Gabor JA, Schwarzkopf R, Davidovitch RI. A novel opioid-sparing pain management protocol following total hip arthroplasty: Effects on opioid consumption, pain severity, and patient-reported outcomes. J Arthroplasty 2019;34:2669-75. [Google Scholar] [PubMed]
- 12. Lim EJ, Kim CH, Kim JW. Effectiveness of multimodal analgesia on surgically treated geriatric hip fracture patients: A propensity score matching analysis. Reg Anesth Pain Med 2025 [Google Scholar] [PubMed]
- 13. Stone AB, Iban YC, Zhong H, Poeran J, Liu J, Cozowicz C, et al. Opioid sparing effects of intravenous and oral acetaminophen in hip fracture patients: A population-based study. J Clin Anesth 2023;86:111074. [Google Scholar] [PubMed]
- 14. Chassery C, Atthar V, Marty P, Vuillaume C, Casalprim J, Basset B, et al. Opioid-free versus opioid-sparing anaesthesia in ambulatory total hip arthroplasty: A randomised controlled trial. Br J Anaesth 2024;132:352-8. [Google Scholar] [PubMed]
- 15. Feng JE, Mahure SA, Waren DP, Lajam CM, Slover JD, Long WJ, et al. Utilization of a novel opioid-sparing protocol in primary total hip arthroplasty results in reduced opiate consumption and improved functional status. J Arthroplast 2020;35:S231-6. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Comparative Evaluation of Multimodal Analgesia Techniques in Total Knee Arthroplasty: A Comparative Study
October 1, 2025 Comparative Evaluation of Multimodal Analgesia Techniques in Total Knee Arthroplasty: A Comparative Study January 1, 2026 Comparative Evaluation of Efficacy of Transdermal Buprenorphine Patch versus Intraoperative Cocktail Injection for Post-operative Pain Relief in Total Hip Arthroplasty
January 1, 2026 Comparative Evaluation of Efficacy of Transdermal Buprenorphine Patch versus Intraoperative Cocktail Injection for Post-operative Pain Relief in Total Hip Arthroplasty November 1, 2024 Functional Outcomes in ACL Reconstruction: A Randomized Controlled Trial Comparing All-Inside and Transportal Techniques
November 1, 2024 Functional Outcomes in ACL Reconstruction: A Randomized Controlled Trial Comparing All-Inside and Transportal Techniques April 7, 2014 A Rare Combination Open Fracture Dislocation of Elbow with Open Fracture both Bones Forearm with Radial Nerve Palsy
April 7, 2014 A Rare Combination Open Fracture Dislocation of Elbow with Open Fracture both Bones Forearm with Radial Nerve Palsy