
Forearm fractures need to be primarily evaluated for both proximal and distal radioulnar joint instability for appropriate management.
Dr. Rajsirish Bellal Sridharan, C27 Villa, Tvs Green Acres, Gandhi Road, Kolapakkam, Chennai - 116, Tamil Nadu, India. E-mail: dr.rajsirish@gmail.com
Introduction:Monteggia fracture-dislocation is defined as a proximal third ulna fracture with radiocapitellar joint dislocation. The term “Monteggia equivalent or variant” describes various injuries with similar radiographic patterns and injury biomechanics. Several isolated cases of unusual injuries associated with Monteggia fractures have been reported. However, an associated TFCC injury has not been described in the literature before. We present a rare report of a 24-year-old female with a Monteggia fracture and associated TFCC injury – a crisscross type of injury.
Case Report:A 24-year-old female was involved in a road traffic accident and presented to our level I trauma center with pain and deformity in the left forearm. On evaluation, she was found to have type I Monteggia fracture-dislocation. Intraoperatively, once the proximal ulna was fixed, she had clicking in the wrist during rotations. Fluoroscopic images showed DRUJ subluxation, but it was stable in supination. Hence was splinted in a reduced position. The patient continued to have persistent symptoms in the wrist despite adequate conservative measures. Hence, she underwent arthroscopic TFCC repair and DRUJ pinning. At her last follow-up (3 months), the patient was clinically better with a good range of motion and no pain.
Conclusion:In treating Monteggia fracture-dislocations, high index of suspicion is needed to diagnose radioulnar joint instability. If they are missed, they can result in long-term disability, so appropriate evaluation to diagnose TFCC and DRUJ injuries is required. DRUJ stabilization and TFCC repair can produce consistent results when treated adequately.
Keywords:TFCC, monteggia, wrist, arthroscopy, proximal ulna.
Monteggia fracture, as initially described by Giovanni Battista Monteggia [1], is an anterior dislocation of radial head with a fracture of the proximal ulna. Jose Luis Bado classified this complex injury into four types [2]. However, the classification did not include certain injuries (radial head fracture, distal humerus fracture, interosseous membrane rupture, and DRUJ injuries), which was later grouped under Monteggia variants. In their systemic review, Artiaco et al. [3] described a new comprehensive locker-based classification system in which he has included most of the injuries associated with Monteggia fracture. In this case report, we present a rare case of proximal radioulnar joint dislocation, proximal ulna fracture (Monteggia fracture) with TFCC injury and DRUJ instability. This case illustrates that distal radioulnar joint instability and TFCC tear may be associated with a Monteggia fracture-dislocation.
A 24-year-old female, right-hand dominant software engineer fell onto her outstretched hand and presented with pain, swelling, and deformity around the left elbow. Initial radiographs showed a closed Monteggia fracture-dislocation (proximal shaft of the ulna with anterior dislocation of the radial head – Bado type 1) (Fig. 1a). Under regional anesthesia, the fracture was fixed with LCDCP, and the radial head was reduced by closed means (Fig. 1b). 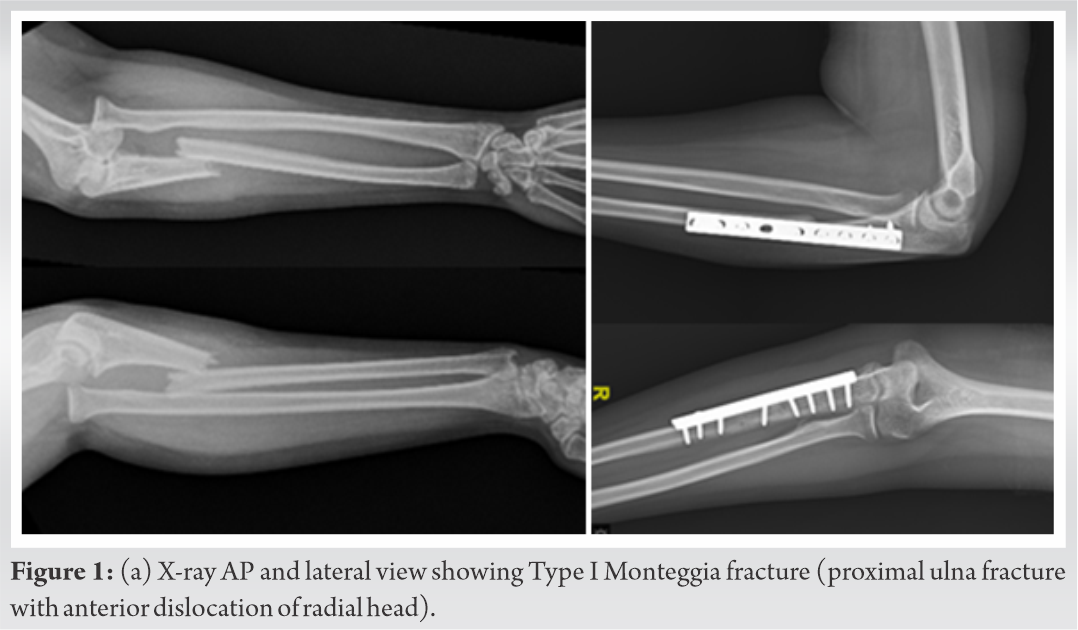 Intraoperatively, we noticed a click at the wrist with pronosupination, and fluoroscopic imaging showed a subtle reducible dorsal subluxation of the distal radioulnar joint. Hence, we performed a closed reduction of DRUJ, and she was given an above elbow slab in full supination. After 3 weeks of the index procedure, the POP cast was removed, and radiographs showed well-reduced radial head and well-aligned ulna fracture. She was started on active and passive range of motion exercises for the elbow and wrist. However, she had persistent wrist pain and stiffness after 2 weeks of physical therapy. Range of motion in the elbow was 0–130o, wrist movements dorsiflexion 0–50o, palmar flexion 0–40o, supination – nil, and pronation 0–40o. Subsequently, we investigated the patient using an MRI, which showed dorsal subluxation of the ulna with TFCC tear in the ulnar attachment of the volar radioulnar ligament (Fig. 2). The patient was counseled for arthroscopic TFCC repair and DRUJ stabilization. She underwent wrist arthroscopy assessment through standard portals, and the volar TFCC was repaired using Arthrex Micro Lasso and FiberWire (Fig. 3). The DRUJ was stabilized with 1.6 mm K-wire.
Intraoperatively, we noticed a click at the wrist with pronosupination, and fluoroscopic imaging showed a subtle reducible dorsal subluxation of the distal radioulnar joint. Hence, we performed a closed reduction of DRUJ, and she was given an above elbow slab in full supination. After 3 weeks of the index procedure, the POP cast was removed, and radiographs showed well-reduced radial head and well-aligned ulna fracture. She was started on active and passive range of motion exercises for the elbow and wrist. However, she had persistent wrist pain and stiffness after 2 weeks of physical therapy. Range of motion in the elbow was 0–130o, wrist movements dorsiflexion 0–50o, palmar flexion 0–40o, supination – nil, and pronation 0–40o. Subsequently, we investigated the patient using an MRI, which showed dorsal subluxation of the ulna with TFCC tear in the ulnar attachment of the volar radioulnar ligament (Fig. 2). The patient was counseled for arthroscopic TFCC repair and DRUJ stabilization. She underwent wrist arthroscopy assessment through standard portals, and the volar TFCC was repaired using Arthrex Micro Lasso and FiberWire (Fig. 3). The DRUJ was stabilized with 1.6 mm K-wire.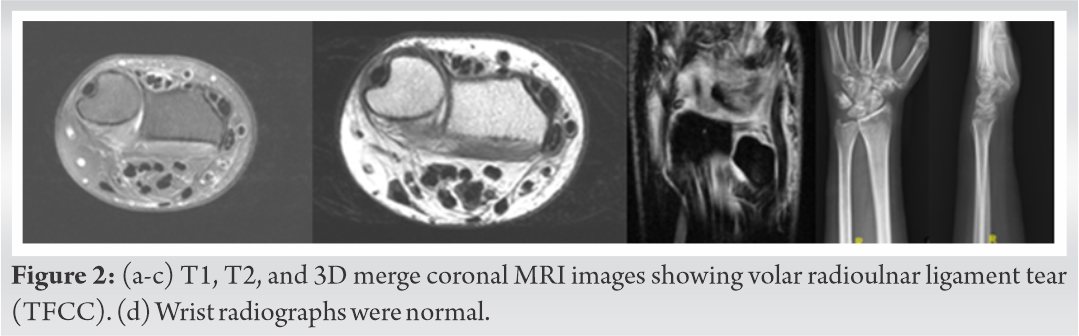
At 3 weeks following the second surgery, we removed the K-wire, and she was started on physiotherapy. The patient was routinely followed up thereafter. At her latest follow-up of 3 months, her range of motion in the wrist was dorsiflexion 0–45o and palmar flexion 0–20o. The forearm movements were pronation 0–80o and supination 0–50o (Fig. 4). All her movements were pain free. The patient was comfortable, and her radiographs showed a healing proximal ulna fracture. Wrist radiographs showed a well-reduced DRUJ.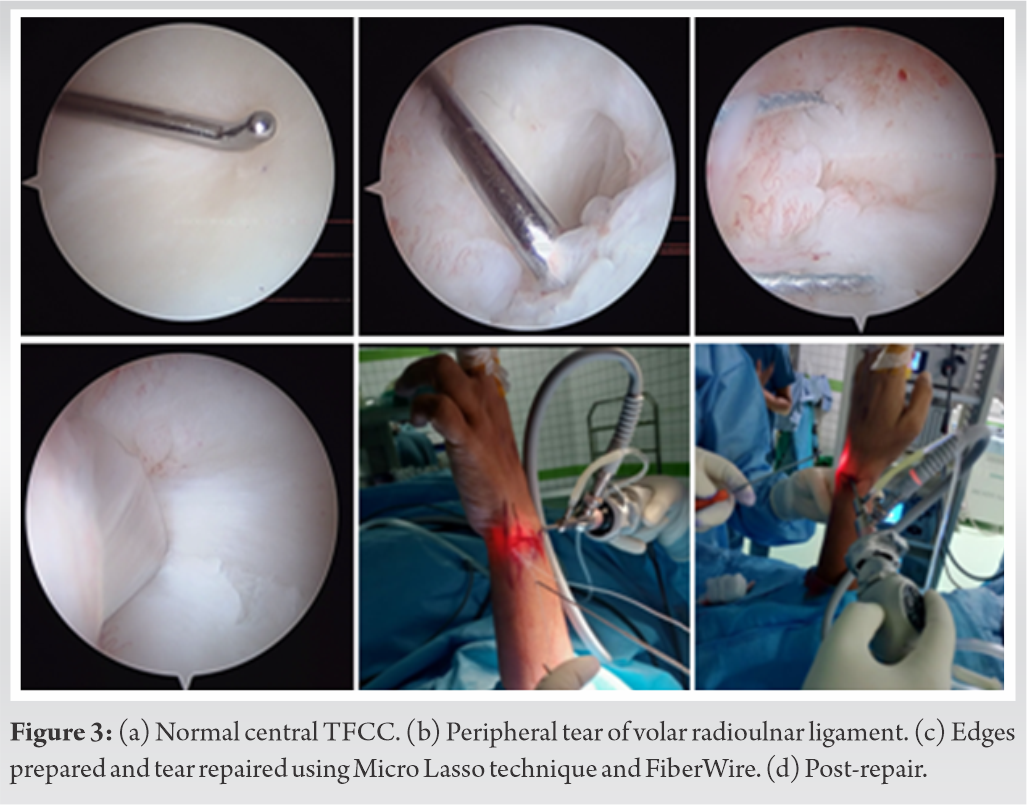
Our patient had peripheral TFCC tear with a Bado Type I Monteggia fracture-dislocation. This injury pattern has not been discussed before in the literature and may represent a less common Monteggia variant. Only two cases of frank DRUJ dislocation associated with this fracture have been reported in the literature, with the disruption of distal interosseous membrane being mooted as a reason [4, 5]. However, there was no IOM injury in our case. The pattern of injury in our patient may be explained by the Locker concept [3]. Artiaco et al. have suggested three lockers in the forearm (DRUJ, PRUJ, and MRUJ). The authors could explain the various described fracture-dislocations of the forearm based on a combination of disruption of these linkages.
The pathogenesis of Monteggia fracture-dislocation has not been established yet. In general, being a double/concomitant injury, it is challenging to explain the pathomechanics [6]. However, based on the locker concept, a twisting injury of the forearm with the IOM as a pivot could result in DRUJ injury associated with Monteggia fracture-dislocations such as in our patient. Six reports in the literature have described simultaneous PRUJ and DRUJ dislocations but without any long bone injury [7, 8, 9, 10, 11, 12]. This injury pattern was described as “crisscross” by Leung et al. by the relative position of the radius and ulna on plain radiographs [7].
Missed DRUJ/TFCC injuries can result in persistent wrist pain [13]. Therefore, the various Monteggia fracture variants need to be identified and treated. While treating forearm injuries, it is imperative to examine both the wrist and elbow joints thoroughly [14]. The initial clinical and radiographic evaluation of the wrist may have been compromised in our patient, as attention was focused on the proximal radial dislocation and the ulnar shaft fracture, with the presumed diagnosis of a Monteggia fracture-dislocation.
In an acute setting, pain and anxiety are major limiting factors in identifying subtle findings. Therefore, proper AP and lateral radiographic views of these joints are needed with specific diligence to joint congruity [14]. When in doubt, opposite wrist X-rays should be taken for comparison. Acquiring further imaging studies, such as magnetic resonance imaging, are warranted if there is diagnostic uncertainty or if plain radiographs are inadequate.
Intraoperatively, accurate reduction (length and rotation) of the ulna fracture provides adequate stability to PRUJ and DRUJ [15]. These often are managed conservatively with splinting/immobilization. There are rare exceptions like IOM rupture where proximal and distal joint stabilization would be necessary in addition to the long bone fixation. In our patient, although the DRUJ was reduced and splinted during the index procedure, the patient had persistent symptoms and warranted TFCC repair with DRUJ stabilization.
Triangular fibrocartilage complex injury is a common etiology of ulnar-sided wrist pain following fall. It can be frequently missed when associated with other concomitant injuries. Less favorable outcomes for resuming pre-injury and grip strength recovery may be attributed to late detection and management. Arthroscopic suture repair using the outside-in technique has encouraging results in peripheral TFCC tears [16]. In our patient, the TFCC tear was successfully treated with arthroscopic TFCC repair and percutaneous DRUJ pinning. At the latest follow-up (3 m), she has regained good forearm rotation and elbow ROM.
In treating Monteggia fracture-dislocations, high index of suspicion is needed in cases where clinical findings suggest DRUJ instability. Missed TFCC tears and DRUJ instability can cause long-term disability. Hence, they should be evaluated at the earliest in Monteggia fracture-dislocations with wrist pain or DRUJ subluxation. In addition, DRUJ stabilization and TFCC repair can produce reliable results in these types of injuries.
TFCC directly connects the distal radius with the ulnar fovea and styloid process, thus providing DRUJ stability. While treating forearm injuries, it is imperative to examine both the wrist and elbow joints thoroughly. Accurate maintenance of length and rotation provides adequate reduction of the DRUJ and most of these injuries are managed conservatively with immobilization. In rare instances with persistent DRUJ instability, timely surgical management provides excellent results.
References
- 1.1. Monteggia GB. Lussazioni delle ossa delle estremita superiori. In: Monteggia GB, editor. Instituzioni Chirurgiches. 2nd ed., Vol. 5. Milan: Maspero; 1814. p. 131-3. [Google Scholar]
- 2.2. Bado JL. The Monteggia Lesion. Springfield, IL: Charles C. Thomas; 1959. [Google Scholar]
- 3.3. Artiaco S, Fusini F, Sard A, Dutto E, Massè A, Battiston B. Fracture-dislocations of the forearm joint: A systematic review of the literature and a comprehensive locker-based classification system. J Orthop Traumatol 2020;21:21. [Google Scholar]
- 4.4. Cheung EV, Yao J. Monteggia fracture-dislocation associated with proximal and distal radioulnar joint instability. A case report. J Bone Joint Surg Am 2009;91:950-4. [Google Scholar]
- 5.5. Zhang Y, Xiao W, Li J. A very rare presentation of reoperation combined both old monteggia fracture and secondary distal radioulnar joint dislocation in adult: A case report. Medicine (Baltimore) 2019;98:e15310. [Google Scholar]
- 6.6. Inoue T, Kubota M, Marumo K. A Type III monteggia injury with ipsilateral fracture of the distal radius and ulna in a child: Case report followed for 21 years. Case Rep Orthop 2018;2018:1876075. [Google Scholar]
- 7.7. Leung YF, Ip SP, Ip WY, Kam WL, Wai YL. The crisscross injury mechanism in forearm injuries. Arch Orthop Trauma Surg 2005;125:298-303. [Google Scholar]
- 8.8. Verettas DJ, Drosos GI, Xarchas KC, Chatzipapas CN, Staikos C. Simultaneous dislocation of the radial head and distal radio-ulnar joint. A case report. Int J Med Sci 2008;5:292-4. [Google Scholar]
- 9.9. Potter M, Wang A. Simultaneous dislocation of the radiocapitellar and distal radioulnar joints without fracture: Case report. J Hand Surg Am 2012;37:2502-5. [Google Scholar]
- 10.10. Nishi T, Suzuki N, Tani T, Aonuma H. Simultaneous dislocation of radiocapitellar and distal radioulnar joint. Case Rep Orthop 2013;2013:106567. [Google Scholar]
- 11.11. Spicer DD, Hargreaves D, Eckersley R. Simultaneous dislocations of the radiocapitellar and distal radioulnar joints. J Orthop Trauma 2002;16:136-8. [Google Scholar]
- 12.12. Papageorgiou C, Vradelis K. Simultaneous dislocation of the proximal and distal radioulnar joints. A case report. Acta Orthop Scand 1995;66:180. [Google Scholar]
- 13.13. Thomas BP, Sreekanth R. Distal radioulnar joint injuries. Indian J Orthop 2012;46:493-504. [Google Scholar]
- 14.14. Macintyre NR, Ilyas AM, Jupiter JB. Treatment of forearm fractures. Acta Chir Orthop Traumatol Cech 2009;76:7-14. [Google Scholar]
- 15.15. Hayami N, Omokawa S, Iida A, Kira T, Moritomo H, Mahakkanukrauh P, et al. Effect of soft tissue injury and ulnar angulation on radial head instability in a Bado Type I Monteggia fracture model. Medicine (Baltimore) 2019;98:e17728. [Google Scholar]
- 16.16. Chen AC, Weng CJ, Chiu CH, Chang SS, Cheng CY, Chan YS. Results of arthroscopic repair of peripheral triangular fibrocartilage complex tear with exploration of dorsal sensory branch of ulnar nerve. Open Orthop J 2017;11:525-32. [Google Scholar]








