
The characteristic MR imaging features are confirmatory for a definitive diagnosis of fibrolipomatous hamartoma (FLH), which alleviates the need for any unnecessary biopsy.
Dr. G S Sabhikhi, Department of Radiodiagnosis, School of Medical Sciences and Research, Sharda University, Greater Noida - 201306, Uttar Pradesh, India. E-mail: gssabhiki@gmail.com
Introduction: Fibrolipomatous hamartoma (FLH) is an uncommon slow-growing tumor of benign etiology, which predominantly affects the median nerve.
Case Report:We report the case study of a 17-year-old male patient, who presented with complaints of a gradually increasing localized swelling over the volar aspect of left hand for 1 year. A contrast-enhanced Magnetic resonance (MR) scan of the left hand was performed which demonstrated characteristic findings. The patient was treated surgically and post-excision histopathological examination confirmed the diagnosis.
Conclusion: The characteristic MR imaging features of coaxial cable-like appearance on axial section or spaghetti shaped enlarged nerve fascicles and fibrous tissue is confirmatory for a definitive diagnosis of FLH, which alleviates the need for any unnecessary biopsy.
Keywords: Fibrolipomatous hamartoma, magnetic resonance imaging, median nerve.
Fibrolipomatous hamartoma (FLH) of median nerve is a slow growing tumor with an uncertain etiology [1, 2]. It is a rare benign tumor with characteristic magnetic resonance image (MRI) findings, which may obviate the need for an unnecessary biopsy [3, 4]. The other names for FLH include neurofibrolipoma, perineural lipoma, intraneural lipoma, neural fibrolipoma, and lipomatosis of nerve [5, 6, 7]. Depending on the extent of nerve involvement, the treatment strategy varies, depends on the extent of nerve involvement as severe motor and sensory deficits, have been reported following complete tumor resection [8, 9, 10]. We report a case of FLH in a young male patient, initially diagnosed purely on the basis of imaging features. He was successfully operated and histopathology specimen confirmed the diagnosis.
A 17-year-old male patient was referred to the Department of Radiology for imaging of a focal swelling over the volar aspect of left hand. Initially, the swelling was peanut-sized which progressed to involve the entire palm region, extending from the distal forearm of wrist to the nar eminence and base of 2nd, 3rd and 4th fingers of left hand as depicted in (Fig. 1). The patient complained of periodic episodes of tingling and parasthesia over 2nd, 3rd and 4th fingers of right hand. There was no past history of trauma over the hand. On examination, an irregular-shaped, fusiform swelling was noted over the volar aspect of left hand, proximally extending from the ulnar aspect of left wrist to the thenar eminence and base of 2nd, 3rd and 4th digits. The swelling had a variable consistency on palpation, being softer over the ulnar aspect and firm over the 3rd and 4th metacarpals. The overlying skin was pinchable and non-adherent. On neurological examination, no motor weakness or sensory loss was elicited. The movements of left wrist revealed terminal restriction of palmar and dorsiflexion. No other cutaneous or soft tissue lesions were present.
Non-contrast multiplanar, multi-sequence MRI of the left hand was performed. MR showed gross thickening of the median nerve. Diffuse presence of lipomatous tissue (hyperintense on T1W and T2W sequences, hypointense on SPAIR sequence) was noted inter-digitating between the prominent thickened nerve fascicles (hypointense on T1W and T2W sequences), in a coaxial cable-like pattern, extending from the level of distal forearm up to the distal metacarpal regions of 2nd-4th digits. The thickened nerve was seen causing compression and displacement of the flexor tendons and convexity of the carpal tunnel retinacular sheath. The extension of the lipomatous tissue was seen extending to the 2nd and 3rd inter-metacarpal space. No evidence of any focal osseous lesions was noted. The tendons of the hand appeared normal in signal intensity (Fig. 2-4). The MR features were suggestive of fibro-lipomatous hamartoma of the median nerve with adjacent mass effect.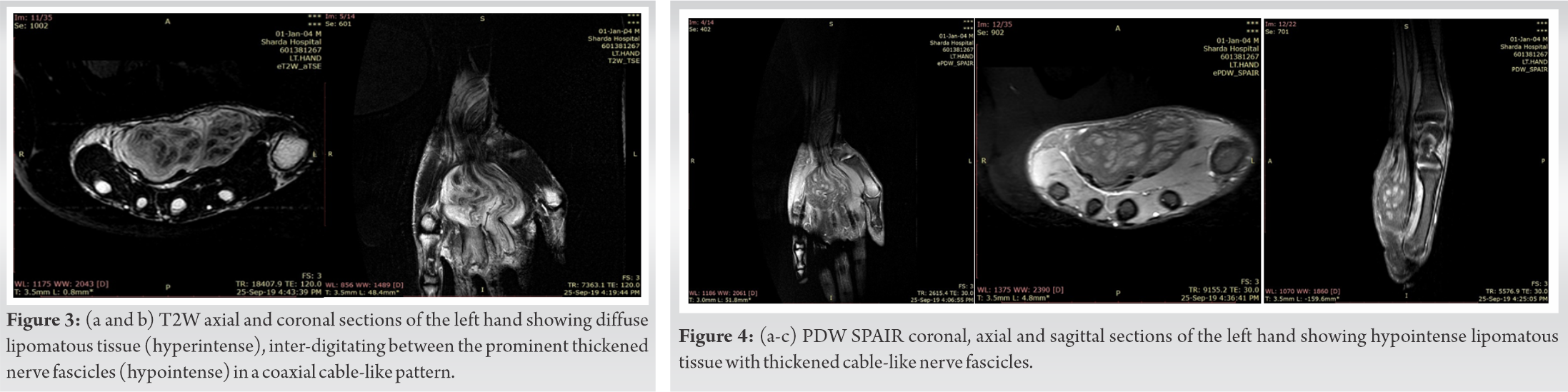
Under general anesthesia, the patient underwent surgical decompression of carpal tunnel. On extensive dissection, the grossly thickened median nerve was identified as two giant fascicles adherent with fibrolipomatous structures around (Fig. 5). Biopsy of fibrolipomatous structures was taken and care was taken not to injure the giant median nerve bundles. The patient reported absolute pain relief after the surgical decompression of carpal tunnel without any neurological deficit. Histopathological examination of the lesion showed a uniform pattern consisting of lobules of mature adipocytes, separated by fibro-collagenous septae, interspersed with perineural elements as demonstrated in (Fig. 6).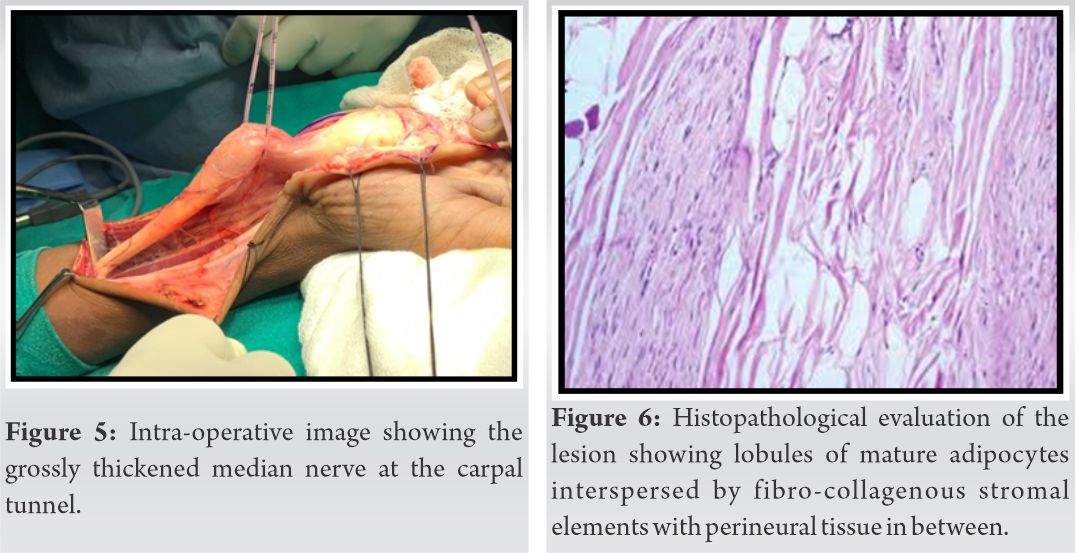
The patient recovered completely from paresthesia after 12 weeks of surgical decompression of the carpal tunnel and he was neurologically stable. The patient performed his activity of daily living without any difficulties. The patient was followed up for 24 months.
FLH are slow-growing tumors of benign etiology, which usually affect the infants, and less commonly children and young adults [6, 9, 11, 12]. The median nerve is the most predominantly affected nerve (80%) in FLH, followed by the ulnar and radial nerves, dorsum of the foot and brachial plexus [9, 11]. Some researchers even consider it to be a congenital tumor, [13] while some others believe it to be incited secondary to nerve irritation, inflammation, or prior trauma [14]. FLH presents as a benign tumorous growth of combination of fibrous and lipomatous tissue within the nerve sheath [15, 16]. Due to their slow‑growing nature, fibrolipomatous lesions of nerve usually present as asymptomatic or minimally symptomatic swelling with or without mild to severe symptoms based on nerve affection [1, 8, 9].
The imaging of FLH may include sonography, computed tomography or MRI. The preferred modality for diagnosing FLH is MRI, which remains the gold standard for diagnosis [7, 14]. Plain radiography examination of FLH is non-specific and it may be normal or may sometimes show mild prominence of the soft tissue which is related to fibrofatty tissue [17, 18]. The sonographic examination demonstrates the presence of hyperechoic fatty tissue which is surrounded by smooth round hypo-to-anechoic fascicles [19]. The spectral Doppler evaluation does not demon¬strate any significant vascularity within the mass [11, 18].
On cross-sectional imaging, FLH exhibit fusiform enlargement of the involved nerve, which is caused by thickening of nerve bundles and adjacent diffuse fibro-fatty proliferation. Thickened nerve bundles appear as tubular or serpentine structures on all imaging modalities. Thickening of the neural fascicles is caused by perineural and endoneural fibrosis [18, 20, 21]. The mature fat cells infiltrate interfascicular connective tissue [18]. The perineural and endoneural fibrosis is responsible for the low signal intensity of thickened nerve fascicles, which are seen as tubular or serpentine structures oriented horizontally along the length of the nerve [9, 11]. On axial images, the enlarged nerve has a coaxial cable-like appearance, due to its thickened nerve fascicles and is interspersed with infiltrating fat, which is the pathognomonic feature of FLH [11, 19, 22]. Another characteristic pathological feature of FLH is growth of the tumor along the branching pattern of the nerve [13, 23, 24]. The differential diagnosis of FLH includes intraneural lipoma, schwannoma, tenosynovitis, ganglion cyst, traumatic neuroma, and vascular malformation [6, 25, 26, 27].
The treatment strategy of FLH is still controversial and is largely dependent on the extent of the nerve involvement [1, 6, 12, 28]. Severe motor and sensory deficits have been reported following complete tumor resection. Conventional treatment involves carpal tunnel decompression by excision of the transverse carpal ligament, followed by biopsy of the enlarged nerve. The review on diagnostic findings of FLH of the median nerve is tabulated (Table 1).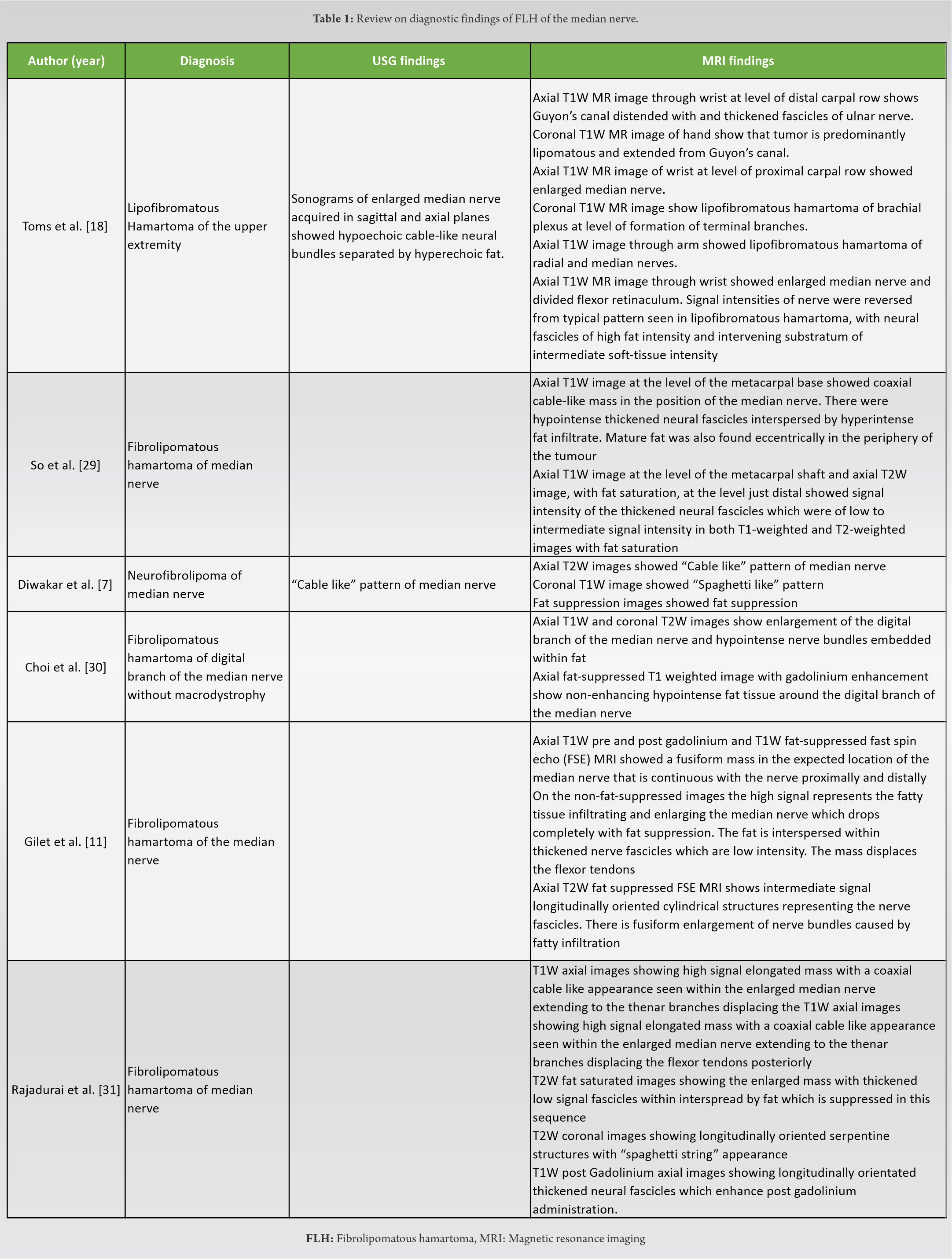
FLH is an uncommon, slow-growing tumor of benign etiology, with a predilection for the median nerve. The characteristic MRI features of coaxial cable-like appearance on axial section or spaghetti shaped enlarged nerve fascicles and fibrous tissue is confirmatory for a definitive diagnosis, which alleviates the need for any unnecessary biopsy.
Although a rare clinical entity of FLH of median nerve, the pathophysiology and management remains controversial, MRI remains the gold standard in the diagnosis of FLH of median nerve.
References
- 1.Ranjan R, Kumar R, Jeyaraman M, Kumar S. Fibrolipomatous hamartoma (FLH) of median nerve: A rare case report and review. Indian J Orthop 2021;55 Suppl 1:267-72. [Google Scholar]
- 2.Saeed MA, Dawood AA, Mahmood HM. Lipofibromatous hamartoma of the median nerve with macrodactyly of middle finger. J Clin Orthop Trauma 2019;10:1077-81. [Google Scholar]
- 3.Azeemuddin M, Waheed AA, Khan N, Sayani R, Ahmed A. Fibrolipomatous hamartoma of the median nerve with macrodystrophia lipomatosa. Cureus 2018;10:e2293. [Google Scholar]
- 4.Uchiyama D, Oshige T, Nakamura K, Koganemaru M. Carpal tunnel syndrome caused by neural fibrolipoma. BMJ Case Rep 2016;2016:bcr2015212819. [Google Scholar]
- 5.Tokyol C, Aslan A, Hastürk GS, Kacar E, Boyaci MG. Spinal neural fibrolipoma: A case report and review of the literature. Asian J Neurosurg 2015;10:341. [Google Scholar]
- 6.Louaste J, Zejjari H, Chkoura M, Houmadi A, Rachid K. Carpal tunnel syndrome due to fibrolipomatous hamartoma of the median nerve. Hand (NY) 2011;6:76. [Google Scholar]
- 7.Diwakar N, Kamble RB, Gidaganti M. Imaging of neurofibrolipoma of median nerve. Neurol India 2011;59:488-9. [Google Scholar]
- 8.Prabhu A, Anil R, Kumar N. Fibrolipomatous hamartoma of the median nerve: An outcome of surgical management in six consecutive cases. Niger J Surg 2020;26:153-8. [Google Scholar]
- 9.Senger JL, Classen D, Bruce G, Kanthan R. Fibrolipomatous hamartoma of the median nerve: A cause of acute bilateral carpal tunnel syndrome in a three-year-old child: A case report and comprehensive literature review. Plast Surg (Oakv) 2014;22:201-6. [Google Scholar]
- 10.Agrawal R, Garg C, Agarwal A, Kumar P. Lipofibromatous hamartoma of the digital branches of the median nerve presenting as carpal tunnel syndrome: A rare case report with review of the literature. Indian J Pathol Microbiol 2016;59:96. [Google Scholar]
- 11.Gilet A, Jeremy M, Gould E. Fibrolipomatous hamartoma of the median nerve. Radiol Case Rep 2015;3:195. [Google Scholar]
- 12.Okechi H, Dimostheni A, Kerscher SR, Gugel I, Bevot A, Schaefer JF, et al. Fibrolipomatous hamartomas of the median nerve in infancy and early childhood-imaging hallmarks, symptomatology, and treatment. Eur J Pediatr 2018;177:567-73. [Google Scholar]
- 13.Razzaghi A, Anastakis DJ. Lipofibromatous hamartoma: Review of early diagnosis and treatment. Can J Surg 2005;48:394-9. [Google Scholar]
- 14.Michel CR, Dijanic C, Woernle M, Fernicola J, Grossman J. Carpal tunnel syndrome secondary to fibrolipomatous hamartoma of the median nerve. Cureus 2021;13:e15363. [Google Scholar]
- 15.Chandler EM, Chen CM, Spector JA. Bilateral fibrolipoma of the median nerve. J Plast Reconstr Aesthet Surg 2009;62:e99-100. [Google Scholar]
- 16.Gennaro S, Merciadri P, Secci F. Intraneural lipoma of the median nerve mimicking carpal tunnel syndrome. Acta Neurochir (Wien) 2012;154:1299-301. [Google Scholar]
- 17.Burt AM, Huang BK. Imaging review of lipomatous musculoskeletal lesions. SICOT J 2017;3:34. [Google Scholar]
- 18.oms AP, Anastakis D, Bleakney RR, Marshall TJ. Lipofibromatous hamartoma of the upper extremity: A review of the radiologic findings for 15 patients. AJR Am J Roentgenol 2006;186:805-11. [Google Scholar]
- 19.Arora R, Arora AJ. Imaging features on sonography and MRI in a case of lipofibromatous hamartoma of the median nerve. Quant Imaging Med Surg 2014;4:207-9. [Google Scholar]
- 20.Maldjian C. Fibrolipomatous hamartoma of the median nerve on CT. Radiol Case Rep 2015;8:895. [Google Scholar]
- 21.Pallewatte AS, Samarasinghe EC. Fibrolipomatous hamartoma arising from the median nerve-a case report. Indian J Radiol Imaging 2021;31:472-5. [Google Scholar]
- 22.Marom EM, Helms CA. Fibrolipomatous hamartoma: Pathognomonic on MR imaging. Skeletal Radiol 1999;28:260-4. [Google Scholar]
- 23.Nouira K, Belhiba H, Baccar S, Miaaoui A, Ben Messaoud M, Turki I, et al. Fibrolipoma of the median nerve. Joint Bone Spine 2007;74:98-9. [Google Scholar]
- 24.Ogose A, Hotta T, Higuchi T, Katsumi N, Koda H, Umezu H. Fibrolipomatous hamartoma in the foot: Magnetic resonance imaging and surgical treatment : A report of two cases. JBJS 2002;84:432-6. [Google Scholar]
- 25.Nardella D, Sohawon S, Carlier A. Lipofibromatous hamartoma of the median nerve. Three case reports. J Plast Reconstr Aesthet Surg 2009;62:e314-7. [Google Scholar]
- 26.Hankins CL. Carpal tunnel syndrome caused by a fibrolipomatous hamartoma of the median nerve treated by endoscopic release of the carpal tunnel. J Plast Surg Hand Surg 2012;46:124-7. [Google Scholar]
- 27.Kameh DS, Perez-Berenguer JL, Pearl GS. Lipofibromatous hamartoma and related peripheral nerve lesions. South Med J 2000;93:800-2. [Google Scholar]
- 28.Ha JF, Teh BM, Abeysuriya DT, Luo DY. Fibrolipomatous hamartoma of the median nerve in the elbow: A case report. Ochsner J 2012;12:152-4. [Google Scholar]
- 29.29. So CK, Tam KF, Lui CY, Lee CM. Fibrolipomatous hamartoma of the median nerve. J HK Coll Radiol 2007;10:81-4. [Google Scholar]
- 30.Choi W, Jung JY, Song IS, Lee JS, Lee TJ, Jung YY. Fibrolipomatous hamartoma of digital branch of the median nerve without macrodystrophy: Two case reports with magnetic resonance imaging findings. J Korean Soc Radiol 2012;67:483-7. [Google Scholar]
- 31.Rajadurai N. Fibrolipomatous hamartoma of median nerve: An MRI diagnosis. Orthop Rheumatol Open Access J 2016;3:555614. [Google Scholar]








