
Ollier’sdiseasecan involve any skeletal structure and must be carefully identified with investigations.
Dr. Mohit Dhingra, Department of Orthopaedics, All India Institute of Medical Sciences, Rishikesh - 249 201, Uttarakhand, India. E-mail: modisbanu77@gmail.com
Introduction: Enchondromas are benign lesion of cartilaginous origin seen in early childhood. Multiple enchondromatosis is also known as Ollier’s disease which involves the appendicular skeleton with multiple site involvement. We present a rare case of appendicular as well as axial skeleton involvement in a case of Ollier’s disease.
Case Report: A 13-year-old male with multiple enchondromas including all the appendicular skeleton along with ribs and cervical spine. Patient was evaluated with X-rays and non-contrast computerized tomography and is on conservative treatment and on regular monthly follow-up with no neurological deficit and no respiratory complications till now. Further evaluation for deformity correction if required, will be considered after skeletal maturity.
Conclusion: Ollier’s disease is a rare presentation with multiple enchondromas in the appendicular skeleton. Current case is further rare presentation of the Ollier’s disease with involvement of cervical spine and ribs as well.
Keywords: Ollier’s disease, enchondroma, spine enchondroma, maffucci syndrome.
Enchondromas are benign cartilaginous tumors seen in early childhood and they lie in close proximity to the physics. Ollier’s disease is a rare non-hereditary condition characterized by multiple enchondromas which usually shows an unilateral distribution. It is seen to have a prevalence of 1 in 100,000 in the population. Literature on multifocal enchondromas in Ollier’s disease is relatively scarce [1]. We report here a case of Ollier’s disease with concurrent involvement of cervical spine and ribs.
A 13-year-old boy presented to our OPD with complaints of difficulty in walking, pain in the neck and multiple swellings along with deformities over both the upper and lower extremities. Family members provide a history of insidious onset of multiple swellings over the body since 6 years of age which first appeared in the right hand and then progressed to the current situation. There was no relevant family history or treatment history.
On examination, the child had multiple swellings of varying sizes and shapes seen over the upper and lower limbs (Fig. 1). Patient had a marked shortening of the left lower limb and walks with a short limb non assisted gait. Palpation revealed swellings to be bony hard in consistency and he was seen to have swellings over the hip, knee, ankle and feet bilaterally with similar findings. A shortening of 2 cm was found on the left lower limb which was infratrochanteric. Chest examination revealed similar swellings over the 6th, 7th, 8th, and 9th rib bilaterally at the costochondral junction anteriorly. A thoracolumbar scoliosis with convexity toward the right side is seen. Movements were restricted in all the major peripheral joints (shoulder, knee, elbow, wrist, hip, ankle, hand, and foot) along with restriction of cervical spine arc of motion. However, pain was present on extremes of flexion and extension with no tenderness over cervical spine.
A thorough skeletal survey in the form of plain radiographs was performed, which showed multiple eccentric, expansile geographic lesions with stippled calcification in the metaphyseal region of the appendicular skeleton and ribs (Fig. 2, 3).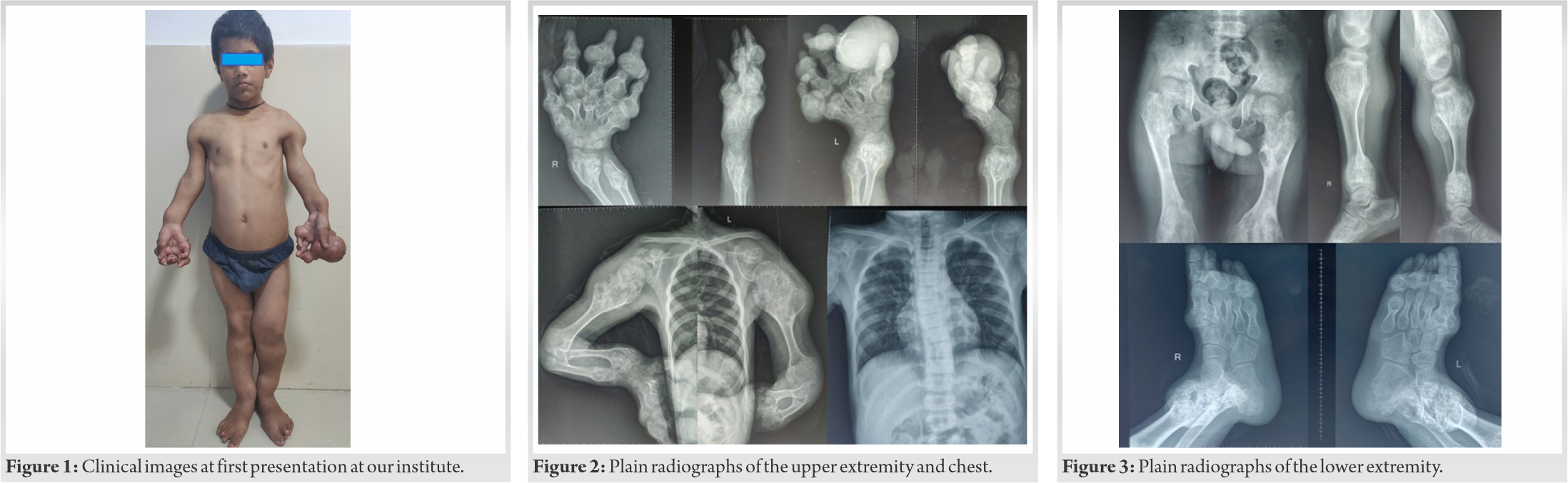 He was further investigated with computed tomography (CT) which revealed similar lesions in the right arch of C1 and C2 with no canal compromise (Fig. 4).
He was further investigated with computed tomography (CT) which revealed similar lesions in the right arch of C1 and C2 with no canal compromise (Fig. 4).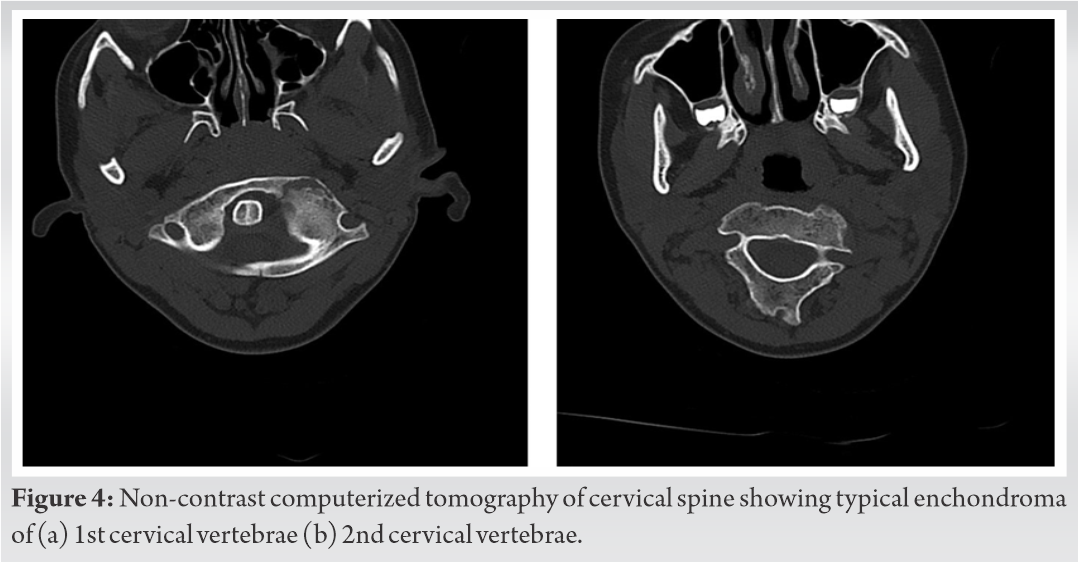 A core biopsy was done from one of the lesion and histopathological examination revealed hypercellular tumor composed of chondrocytes with mild anisonucleosis with peripheral rim of osteoid deposition suggestive of enchondroma (Fig. 5). With proper counseling and explanation regarding the condition of the patient to the guardian, conservative treatment protocol with aim to improve patient function was taken for the patient. He is kept on observation with monthly follow-up for any new lesion or complaints with symptomatic treatment for pain in form of Paracetamol 500 mg SOS and Shoe raise on the shorter side. Patient completed 1-year of follow-up with no increase in any lesion and no pain. There is no neurological deficit and no respiratory symptoms in regular follow up. Patient is followed up on regular basis every month for any sudden increase in swelling, any respiratory complaints, any neurological symptoms and radiographic evaluation as monitoring protocol for malignant transformation of the benign condition.
A core biopsy was done from one of the lesion and histopathological examination revealed hypercellular tumor composed of chondrocytes with mild anisonucleosis with peripheral rim of osteoid deposition suggestive of enchondroma (Fig. 5). With proper counseling and explanation regarding the condition of the patient to the guardian, conservative treatment protocol with aim to improve patient function was taken for the patient. He is kept on observation with monthly follow-up for any new lesion or complaints with symptomatic treatment for pain in form of Paracetamol 500 mg SOS and Shoe raise on the shorter side. Patient completed 1-year of follow-up with no increase in any lesion and no pain. There is no neurological deficit and no respiratory symptoms in regular follow up. Patient is followed up on regular basis every month for any sudden increase in swelling, any respiratory complaints, any neurological symptoms and radiographic evaluation as monitoring protocol for malignant transformation of the benign condition.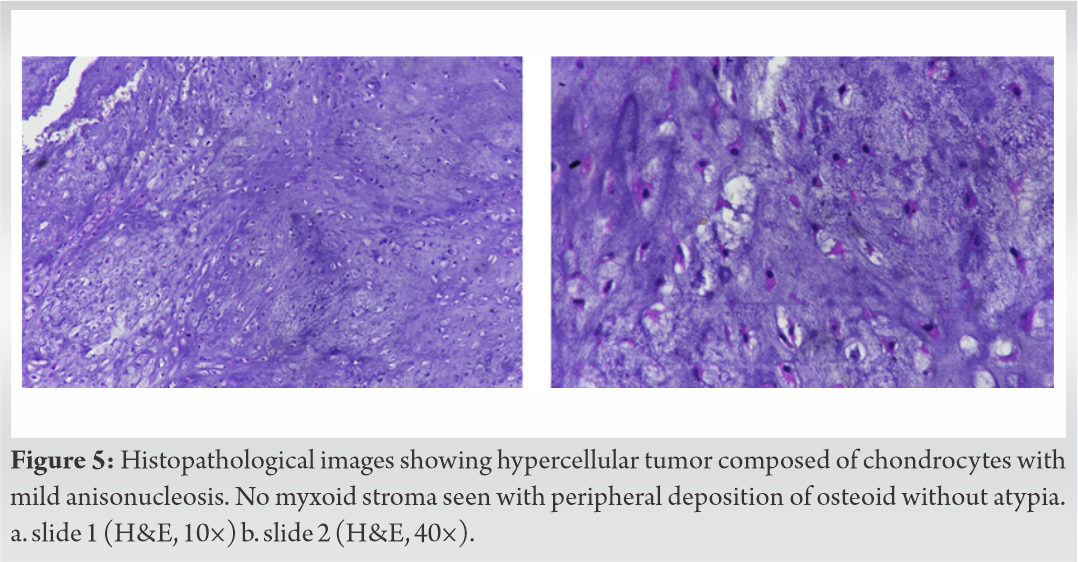
Enchondromas are benign chondrogenic or cartilaginous tumors. They are commonly located in the metaphyseal region (intraosseous) and occur frequently near the growth plate. The lesions are usually solitary with a predilection for small bones of hands and feet. The tumor is composed of hyaline cartilage and grows into the diaphysis (medullary cavity) which often fails to ossify. The incidence of enchondroma reported in literature is 2.8 % and it’s the second most common benign tumor following osteochondroma. While it may affect an individual at any age, its commonly seen in 20–50 years of age with a 1:1 male to female ratio. It is caused by the abnormal chondroblast function in the metaphysis [2].
Enchondromas are usually solitary lesions. The condition in which a person has multiple enchondromas (enchondromatosis) is called as Ollier’s disease [3, 4]. Its characterized by the presence of asymmetric lesions which are of various morphology such as shape and size which leads to considerable disfigurement of the body part [5]. The condition sees frequent involvement of the short bones such as phalanges, metacarpals, metatarsals, and long tubular bone such as femur, tibia, and fibula but, involvement of the trunk is rare except ribs and scoliosis that is due to pelvic involvement [6]. Involvement of the spine is further rare with scarce data about it. If hemangiomas are seen along with multiple enchondromas that maybe subcutaneous or visceral its termed as maffucci syndrome [6].
Ollier’s is generally diagnosed in first decade of the life with multiple asymmetric swellings with unilateral predominance, limb length discrepancy and deformities. The affected bones are usually shorter and develop deformations in the curvature and often presents with bending of bones. Familial trait has still not been established and is viewed as a nonhereditary sporadic disorder. The mutations in isocitrate dehydrogenase (IDH1 and IDH2) and PTH1R are often seen [7]. The diagnosis is made based upon the radiographic appearance and clinical features and histological examination. A CT is helpful in cases wherein the radiographic evaluation is not suitable as in pelvis and spine. Magnetic resonance imaging analysis has less significance in imaging of the lesions. The histology often depicts higher cellularity, binucleated cells and pleomorphism as compared to solitary lesions. Although enchondromas have low chance of malignant transformation, Ollier’s disease is characterized by a malignant transformation rate of up to 35%. A lifelong monitoring of the patient is required with surgical intervention reserved for cases of pathological fracture, growth defect and malignant transformation [8, 9, 10].
The patient in our case has a peculiar presentation of Ollier’s disease. He had involvement of almost all bones of the appendicular skeleton (upper and lower limb). Moreover, there was enchondromas seen along the ribs and of the cervical spine. Literature on symmetrical involvement of bones in Ollier’s disease is scarce and those which report on the involvement of axial skeleton are even rarer. The treatment in cases of Ollier’s disease is mainly focused on nursing care and looking out for possible complications. A periodic evaluation of the patients is to be done to rule out the chance of malignant transformation.
Ollier’s disease presents as multiple enchondromas that generally affects the small bones or the appendicular skeleton. Involvement of spine and ribs is rare and simultaneous presentation in single patient is not reported yet. We conclude that the thorough investigation in case of Ollier’s disease should be done to look out for areas not assessable with X-rays.
Ollier’s disease is a rare presentation which poses challenges to the orthopedic surgeons regarding a proper treatment plan. A thorough clinical assessment is necessary to rule out any spinal involvement in every case as neurological symptoms may not be present is every case. Deformity and disability needs to be properly managed with proper counseling as well.
References
- 1.Flemming DJ, Murphey MD. Enchondroma and chondrosarcoma. Semin Musculoskelet Radiol 2000;4:59-71. [Google Scholar]
- 2.Silve C, Jüppner H. Ollier disease. Orphanet J Rare Dis 2006;1:37. [Google Scholar]
- 3.Kumar A, Jain VK, Bharadwaj M, Arya RK. Ollier disease: Pathogenesis, diagnosis, and management. Orthopedics 2015;38:e497-506. [Google Scholar]
- 4.Miyawaki T, Kinoshita Y, Iizuka T. A case of Ollier’s disease of the hand. Ann Plast Surg 1997;38:77-80. [Google Scholar]
- 5.Wang JP, Xu ZY, Bao ZQ, Dai XS, Ma L, Yao N, et al. Ollier disease: Two case reports and a review of the literature. Am J Transl Res 2018;10:3818-26. [Google Scholar]
- 6.Ding C, Chen W, Liu F, Xiong M, Chen J. Skull base chondrosarcoma caused by ollier disease: A case report and literature review. World Neurosurg 2019;127:103-8. [Google Scholar]
- 7.Tan CL, Vellayappan B, Wu B, Yeo TT, McLendon RE. Molecular profiling of different glioma specimens from an Ollier disease patient suggests a multifocal disease process in the setting of IDH mosaicism. Brain Tumor Pathol 2018;35:202-8. [Google Scholar]
- 8.Chun KA, Stephanie S, Choi JY, Nam JH, Suh JS. Enchondroma of the Foot. J Foot Ankle Surg 2015;54:836-9. [Google Scholar]
- 9.Le BB, Nguyen BD. Ollier disease with digital enchondromatosis: Anatomic and functional imaging. Clin Nucl Med 2014;39:e375-8. [Google Scholar]
- 10.Errani C, Tsukamoto S, Ciani G, Akahane M, Cevolani L, Tanzi P, et al. Risk factors for local recurrence from atypical cartilaginous tumour and enchondroma of the long bones. Eur J Orthop Surg Traumatol 2017;27:805-11. [Google Scholar]







