
Prompt recognition, with optimal operative intervention, provides satisfactory functional outcomes for displaced scaphoid fractures.
Dr. Akash Singhal, Department of Orthopaedics, Government Medical College and Hospital, Chandigarh, India. E-mail: akash15636@ymail.com
Introduction: Scaphoid fractures are common wrist injuries and are commonly missed. Patients present with radial-sided wrist pain. Computed Tomography and Magnetic Resonance Imaging help in better planning, with analysis of comminution, torn ligaments, timely diagnosis, and intricate fixation prevent avascular necrosis, non-union, and carpal collapse.
Case Presentation:We present a rare scenario of right hand dominant 42 years male with scaphoid waist fracture, where the fracture fragment was unusually displaced 4 cm proximal to the wrist in the volar compartment of the forearm. Urgent open reduction and internal fixation with a Herbert screw was done. At 1 year follow-up, fracture united, with satisfactory range of motion and functional outcomes of the wrist.
Conclusion: Timely diagnosis and urgent operative intervention for unstable displaced scaphoid fractures with rigid fixation provides long-term satisfactory outcomes and prevents complications.
Keywords: Displaced, rare, scaphoid, union, unusual.
Scaphoid is the most common carpal bone to get fractured, accounting for 60% of all carpal fractures [1]. Waist fractures account for a majority of the fractures of the scaphoid, followed by proximal pole and distal pole fractures [1]. Typically, patients present with radial-sided wrist pain on fall on outstretched hand [2]. Forming an intricate mechanical linkage with distal radius and carpal bones, with unique blood circulation, scaphoid fractures are prone for avascular necrosis, non-union, carpal collapse, etc. [3].
Scaphoid fractures remain notorious to remain undiagnosed and differentials most commonly with wrist pain or ligament disruption cases [4]. Though initial wrist radiographic views form the first investigation, in recent years Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) have proven to be more consistent and precise in the assessment of fracture anatomy [1]. The treatment protocol is dictated by the fracture anatomy including the site of the fracture, communication, displacement, associated carpal bones fracture and instability, etc. [4]. Commonly used options include conservative management in form of a short arm cast and operative management in form of screw fixation [4]. We report a rare case of an unusual occurrence of scaphoid fracture fragment in a volar compartment of the distal forearm.
A 42-years-male right-hand dominant patient suffered a low-energy trauma after he fell from 8 feet height on his outstretched hand. The patient following this went to a periphery site primary care center, with complaints of radial sided wrist pain and swelling, where analgesics were given and the patient was referred to our tertiary care center. On presentation to the emergency room of our hospital, distal neurovascular status was found to be normal, splint was given and X-rays were done. On the evaluation of X-rays and CT, the patient was found to be suffering from a right-sided scaphoid fracture, with the second half of the fracture fragment lying approximately 4 cm proximal in the distal volar forearm compartment (Figs. 1, 2).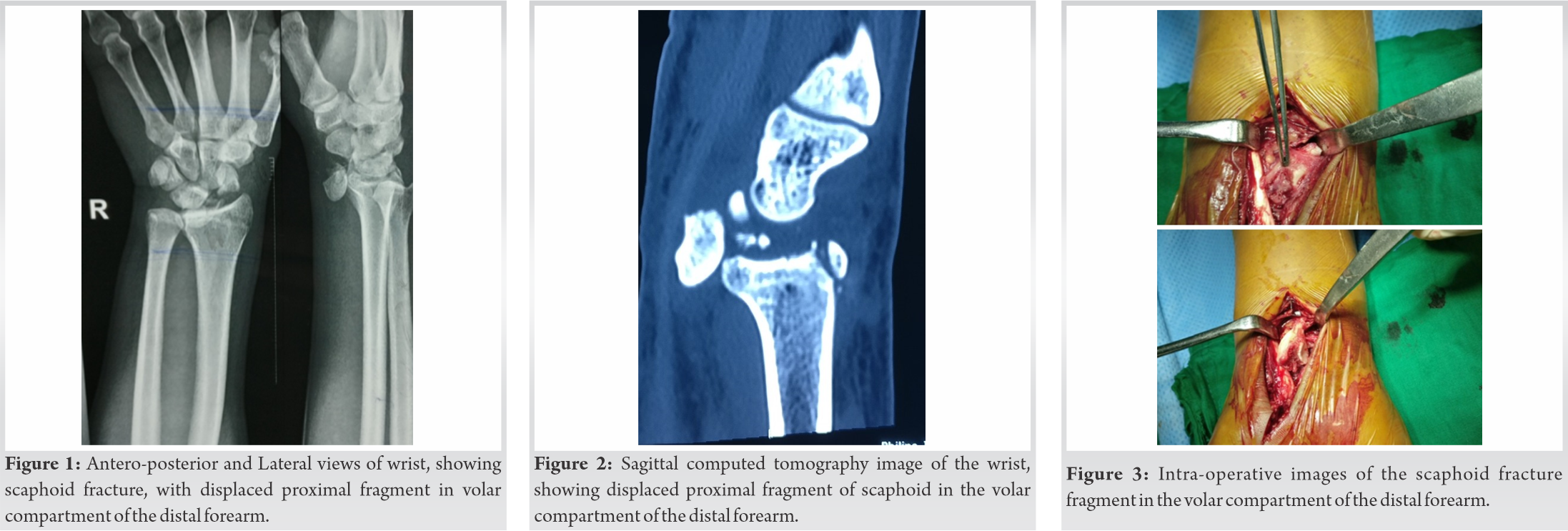 A plan for urgent operative intervention was made. Extended Palmar approach to the scaphoid was used and a fracture fragment was seen lying in the distal volar forearm compartment, 6 cm proximal to the distal wrist crease, lying adjacent to the Flexor Carpi radialis (Fig. 3). Fracture ends were freshened up and reduced provisionally with k wires and then definitive internal fixation was done with one Herbert screw. Post-operatively, a single dose of intravenous 1.5 g cefuroxime was given and the wrist was immobilized with a short arm cast for 6 weeks. After 6 weeks, the cast was removed, wrist range of motion exercises was started. At 1 year follow-up, the complete union was present, with satisfactory grip strength, wrist ROM from 70 degrees dorsiflexion to 40 degrees palmar flexion, Mayo wrist score of 88, and Patient Rated Wrist/Hand Evaluation questionnaire score of 21 [5] (Fig. 4, 5).
A plan for urgent operative intervention was made. Extended Palmar approach to the scaphoid was used and a fracture fragment was seen lying in the distal volar forearm compartment, 6 cm proximal to the distal wrist crease, lying adjacent to the Flexor Carpi radialis (Fig. 3). Fracture ends were freshened up and reduced provisionally with k wires and then definitive internal fixation was done with one Herbert screw. Post-operatively, a single dose of intravenous 1.5 g cefuroxime was given and the wrist was immobilized with a short arm cast for 6 weeks. After 6 weeks, the cast was removed, wrist range of motion exercises was started. At 1 year follow-up, the complete union was present, with satisfactory grip strength, wrist ROM from 70 degrees dorsiflexion to 40 degrees palmar flexion, Mayo wrist score of 88, and Patient Rated Wrist/Hand Evaluation questionnaire score of 21 [5] (Fig. 4, 5).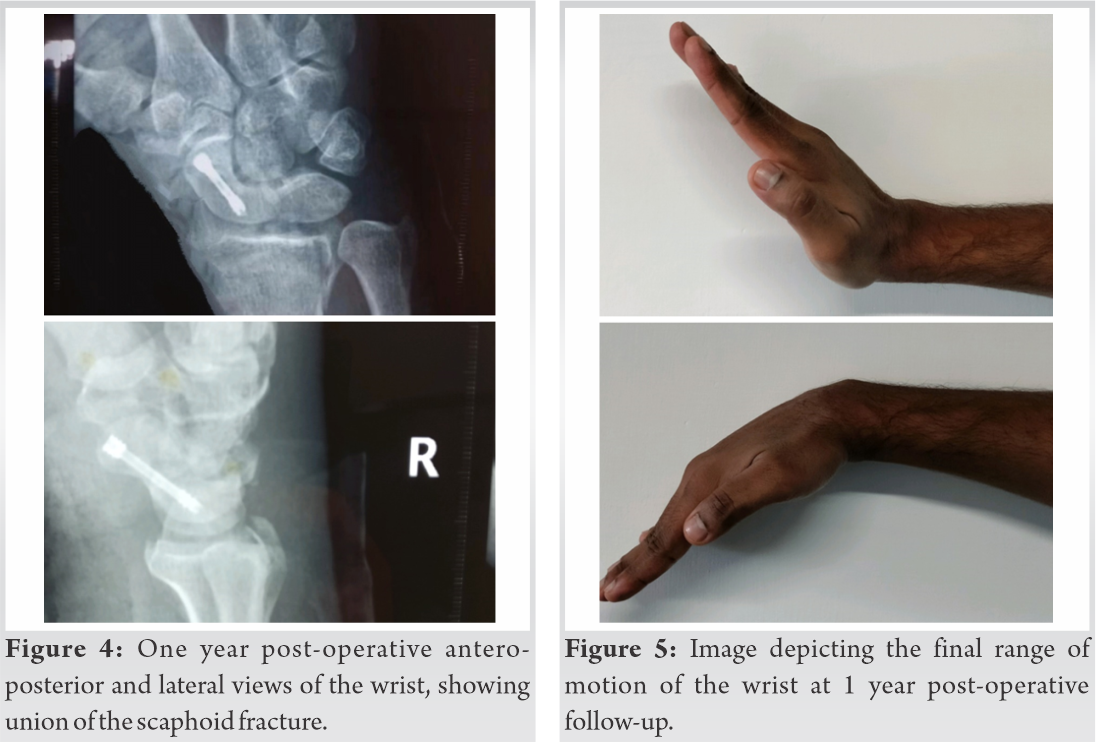
Scaphoid fractures are the most common traumatic carpal bone injuries presenting to the emergency room [1]. Though in the current case, the diagnosis was very much straightforward, many a time, diagnosis is missed with conventional radiographic views alone, and hence, CT and MRI should form a part of routine investigation for patients presenting with post-traumatic radial sided pain and snuffbox tenderness [4, 6]. Further, CT and MRI help in better planning, with analysis of comminution, torn ligaments, etc., leading to sub-optimal management [6, 7]. As scaphoid is covered with articular cartilage in >80% surface and intricate blood supply, timely diagnosis and optimal intervention should be the crux, as delay in diagnosis lead to preventable complications including non-union, mal-union, AVN, progressive degenerative changes, and carpal collapse, the so-called scaphoid non-union advanced collapse., with suboptimal results on delayed intervention [1, 3, 4, 8]. In the present case, timely diagnosis with help of X-rays and CT scan and intervention within 48 h from injury, led to satisfactory functional outcomes, no such complications were observed at 1-year follow-up (Fig. 1, 2).
Scaphoid waist fractures can be approached from both the palmar and dorsal side of the wrist [9]. However, the scaphoid has a precarious blood supply, with a dorsal carpal branch of the radial artery comprising of a major blood vessel, entering through the dorsal ridge of the scaphoid, palmar approach is commonly used, as it prevents blood supply damage and simultaneously gives an adequate exposure [4, 8, 9]. Further, the dorsal approach to scaphoid waist fractures, wrist hyperflexion is needed, which may exaggerate the humpback deformity [4, 9]. In the current case, an extended palmar approach was used for fixation of the scaphoid waist fracture (Fig. 3).
Treatment options comprise percutaneous/open reduction and international fixation (ORIF) with screws or K-wires [4]. The percutaneous approach is mostly used for undisplaced/minimally displaced fractures whereas ORIF is preferred for displaced fractures [4]. Further, as the scaphoid fractures heal by a primary union, with the formation of harversian canals and vessels and without any callus formation, solid anatomical fixation is required with a thicker implant [10]. In the current case, ORIF was done with one Herbert screw (rather than K-wires, which provides suboptimal stability) drilled in a retrograde fashion, 5 mm shorter than the required depth to prevent protrusion, and position was confirmed under c-arm images, to see for the correct length and alignment of the fracture fragments[4, 10] (Fig. 4).
Most of the previously published cases in the literature report the unsual incidence, diagnosis, and treatments of scaphoid fractures, with no mention of the rare occurrence of such enormous displacement of scaphoid fracture fragment [11]. We could find only two related cases by Wanajo et al. and Toker et al., in which they mentioned the unusual dorsal dislocation and volar dislocation of scaphoid fracture fragment, respectively, and that too way back in 2008 and 2009 respectively [11, 12]. In addition, both of these previously reported cases were managed with k wires, rather than Herbert screws, which provide more stable fixation [11, 12]. To add to this, the case reported by Wanajo et al. reported complication of scapholunate dissociation on follow-up, while the case report by Toker et al. had a short-term follow-up of only 8 weeks [11, 12]. The current case report had no complications and showed complete union at 1-year follow-up.
Timely diagnosis, with optimal fracture fragments fixation through palmar approach, provides satisfactory long-term functional outcomes in unusually displaced, unstable scaphoid fractures.
Complex scaphoid fractures with enormous displacement necessitates early operative intervention for long-term optimal functional outcomes. Appropriate approach and pre-operative surgical planning get satisfactory results.
References
- 1.Duckworth AD, Jenkins PJ, Aitken SA, Clement ND, Court-Brown CM, McQueen MM, i. Scaphoid fracture epidemiology. J Trauma Acute Care Surg 2012;72:E41-5. [Google Scholar]
- 2.Jørgsholm P, Thomsen NO, Besjakov J, Abrahamsson SO, Björkman A. The benefit of magnetic resonance imaging for patients with posttraumatic radial wrist tenderness. J Hand Surg Am 2013;38:29-33. [Google Scholar]
- 3.Berger RA. The anatomy of the scaphoid. Hand Clin 2001;17:525-32. [Google Scholar]
- 4.Clementson M, Björkman A, Thomsen NO. Acute scaphoid fractures: Guidelines for diagnosis and treatment. EFORT Open Rev 2020;5:96-103. [Google Scholar]
- 5.Slutsky DJ. Outcomes assessment in wrist surgery. J Wrist Surg 2013;2:1-4. [Google Scholar]
- 6.Gilley E, Puri SK, Hearns KA, Weiland AJ, Carlson MG. Importance of computed tomography in determining displacement in scaphoid fractures. J Wrist Surg 2018;7:38-42. [Google Scholar]
- 7.Ring D, Lozano-Calderón S. Imaging for suspected scaphoid fracture. J Hand Surg Am 2008;33:954-57. [Google Scholar]
- 8.Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg Am 1980;5:508-13. [Google Scholar]
- 9.Geissler WB, Adams JE, Bindra RR, Lanzinger WD, Slutsky DJ. Scaphoid fractures: What’s hot, what’s not. Instr Course Lect 2012;61:71-84. [Google Scholar]
- 10.Marsell R, Einhorn TA. The biology of fracture healing. Injury 2011;42:551-5. [Google Scholar]
- 11.Wanajo S, Sato K, Nakamura T, Ikegami H, Tanino Y, Toyama Y Isolated dorsal fracture-dislocation of the scaphoid: A case report. J Hand Surg Eur Vol 2008;33:311-3. [Google Scholar]
- 12.Toker S, Kilincoglu V. An abnormally displaced scaphoid fracture: A case report. Cases J 2009;2:9309. [Google Scholar]





