
The modified Smith-Petersen approach combined with ASIS osteotomy is a safe and efficient way for the management of anterior dome impaction acetabular fractures.
Dr. Theodoros H Tosounidis, Department of Orthopaedic Surgery, University Hospital of Heraklion, Heraklion, Crete - 71500, Greece. E-mail: ttosounidis@yahoo.com
Introduction:A case of anterior column (AC) and anterior dome marginal impaction acetabular fracture with concomitant injury of the common femoral artery (CFA) is presented.
Case Report:A 31-year-old patient suffered an anterior hip dislocation with ipsilateral fracture of the AC of the acetabulum and anterior dome impaction along with CFA injury. The fracture was treated utilizing the Smith-Petersen approach along with Anterior Superior Iliac Spine osteotomy. The impacted anterior dome and was stabilized using the two-level reconstruction technique. The patient was mobilized the first post-operative day and toe-touch weight bearing was exercised for 12 weeks. At 36 months post-operative, the patient was free of any hip symptoms and no radiographic signs of hip arthritis were present.
Conclusions: This above surgical approach provided adequate exposure of the anterior dome impaction fracture with subsequent excellent reduction and secure fixation. Surgeons treating these types of injuries should be aware of this surgical option.
Keywords: Hip dislocation, acetabulum fracture, anterior column, anterior dome, marginal impaction.
We present a case of anterior column (AC) acetabular fracture with marginal impaction of the anterior acetabular dome (AD) in a patient that was treated with open reduction and internal fixation of the anterior column and two-level reconstruction of the dome marginal impaction utilizing the modified Smith-Petersen (S-P) approach along with Anterior Superior Iliac Spine (ASIS) osteotomy.
A 31-year-old patient was involved in road traffic collision and suffered an isolated injury to his right hemipelvis. The patient was clinically neurovascularly intact with Ankle Brachial Index normal for both lower extremities. Pelvic radiographs showed an anterior hip dislocation and a right acetabular fracture (Fig. 1a). The hip was relocated and the subsequent total body Computed Tomography (CT) scan revealed a fracture of the AC of the acetabulum along with anterior dome acetabular impaction (Fig. 1b). The CT Scan also revealed an intimal injury of the right common femoral artery (CFA) at the level of the inguinal ligament. The right lower limb arterial duplex revealed a dissection flap on the posterior wall of the CFA, which caused no significant velocity ratios with stable appearance and no extravasation. Non-operative management of the CFA injury was advised by the vascular surgery team.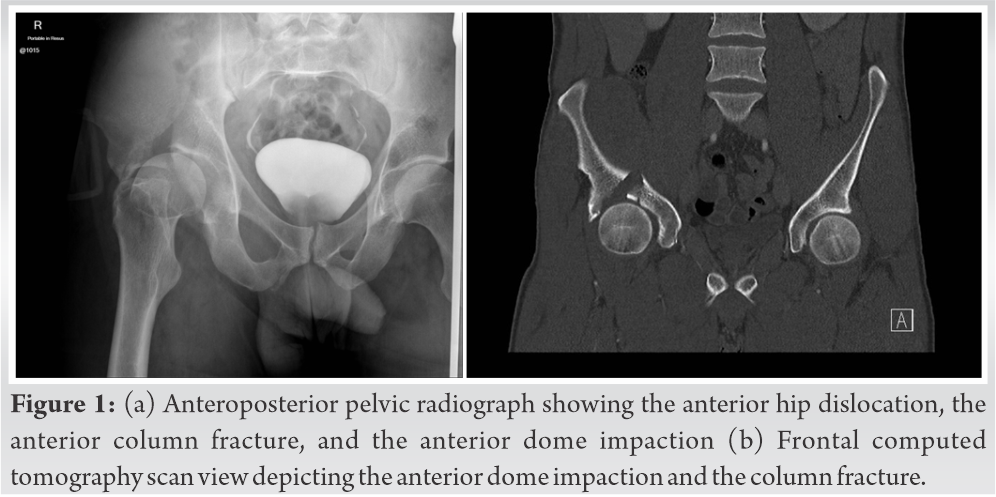
The definitive management of the injury was undertaken on the 7th post-injury date. Due to the injury of the CFA, an approach avoiding any manipulation of it theodorostosounidis was deemed essential. For that purpose, a modified S-P approach along an osteotomy of the ASIS was used. The S-P approach was extended proximally to incorporate the 1st window of the ilioinguinal approach (I-I). A digastric ASIS osteotomy was performed in order to gain access to the AD impaction and avoid undue tension to the vascular structures. The rectus femoris insertion to the anterior inferior iliac spine was left intact.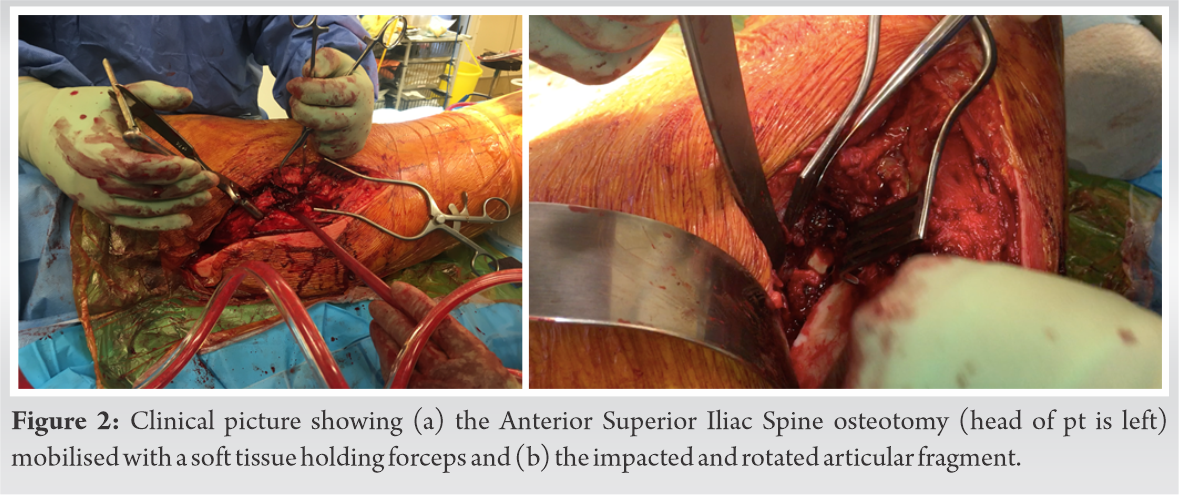 Mobilizing the ASIS and the attached soft tissues medially provided access to the impacted area, which was rotated around a posteriorly based hinge. Access to the intra-articular impaction was provided through the main AC fragment. Derotation of the 1 × 2 cm articular dome fragment (Fig. 3a, b) was performed using a Howarth elevator and the femoral head was a template for dome reduction. Great care was taken to mobilise the articular surface along with a sufficient amount of subchondral bone. Provisional stabilisation was achieved with two 0.062-inch Kirschner wires (Fig. 3c).
Mobilizing the ASIS and the attached soft tissues medially provided access to the impacted area, which was rotated around a posteriorly based hinge. Access to the intra-articular impaction was provided through the main AC fragment. Derotation of the 1 × 2 cm articular dome fragment (Fig. 3a, b) was performed using a Howarth elevator and the femoral head was a template for dome reduction. Great care was taken to mobilise the articular surface along with a sufficient amount of subchondral bone. Provisional stabilisation was achieved with two 0.062-inch Kirschner wires (Fig. 3c).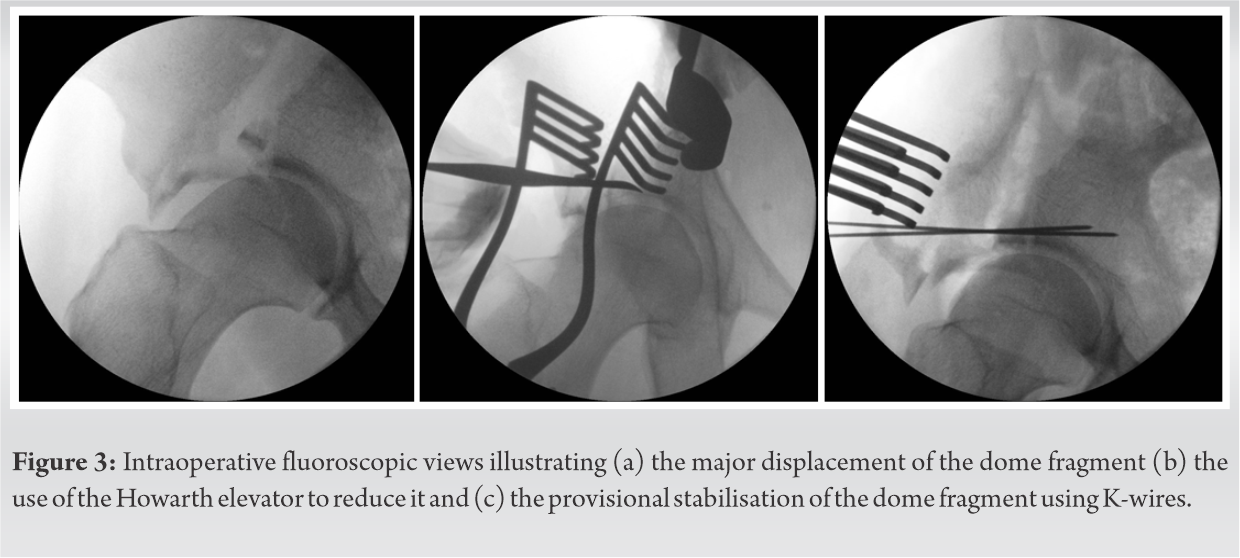 No graft was used to fill in the subchondral void. Subsequent stabilization with three cortical, fully treaded, 2.0 mm screws was performed. The screws were placed close to the articular surface in a rafting mode, taking care to countersink the screw heads into the subchondral bone. The AC was then reduced and stabilized using standard techniques.
No graft was used to fill in the subchondral void. Subsequent stabilization with three cortical, fully treaded, 2.0 mm screws was performed. The screws were placed close to the articular surface in a rafting mode, taking care to countersink the screw heads into the subchondral bone. The AC was then reduced and stabilized using standard techniques.
The ASIS osteotomy was fixed with one cortical, fully threaded, 3.5 mm screw in a lag mode (Fig. 4a-c).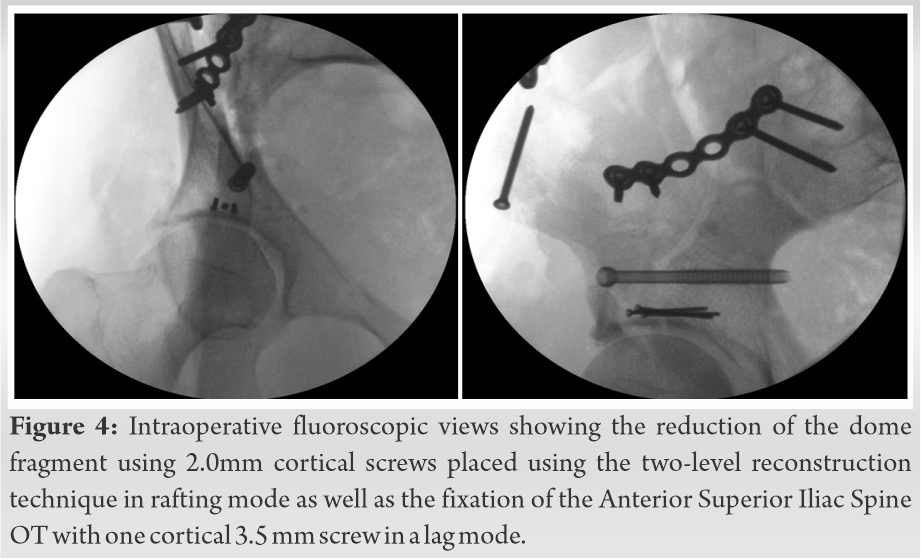 The patient was mobilized the first post-operative day and toe-touch weight-bearing was exercised for 12 weeks due to AD impaction. Full weight-bearing was allowed at 3 months. The patient had regular follow-up visits with clinical and radiological review at 2, 6, 12, weeks and 6, 12, 24, and 36 months. At the final follow-up, the patient was free of any hip symptoms. Radiological review revealed no signs of hip arthritis, the osteotomy had united and small heterotopic ossification was evident at the interspinous area (Fig. 5a-c).
The patient was mobilized the first post-operative day and toe-touch weight-bearing was exercised for 12 weeks due to AD impaction. Full weight-bearing was allowed at 3 months. The patient had regular follow-up visits with clinical and radiological review at 2, 6, 12, weeks and 6, 12, 24, and 36 months. At the final follow-up, the patient was free of any hip symptoms. Radiological review revealed no signs of hip arthritis, the osteotomy had united and small heterotopic ossification was evident at the interspinous area (Fig. 5a-c).
In the herein report we present a rare case of AC/AD impaction fracture that was treated with a modified S-P approach along with ASIS osteotomy utilizing the two-level reconstruction technique for the management of the impacted articular area. To the best of our knowledge, this is the first report of such a case in the contemporary orthopaedic trauma surgery literature.
ASIS osteotomy is a digastric osteotomy with the external oblique muscle attached superiorly to it and the sartorius muscle attached inferiorly. This allows for stable fixation of the osteotomy when it is re-attached to the iliac bone. In a cadaveric study, Sheean et al. [1] combined an anterior intrapelvic approach (AIP) with lateral window-ASIS osteotomy and they concluded that iliopectineal eminence visualization is enhanced. The authors suggested that this combination could be used as a suitable alternative to I-I approach for selected fractures. Sagi et al. [2] reported on a series of 30 acetabular fractures that (18 associated both column fractures and 12 AC and posterior hemitransverse). The authors reported improved visualization especially in patients with a large abdomen and in fractures that involve the anterior wall and the pubic root. At their series, there was no osteotomy related complications such as lateral femoral cutaneous nerve palsy, non-union, failures of the osteotomy fixation. In the case presented in this report, we refrained from proceeding via an ilioinguinal or AIP because of the injury of the CFA and because we anticipated adequate fracture exposure via the S-P approach and the ASIS osteotomy.
Marginal impaction is a well-known entity that can be encountered either as part of the posterior wall injury or in the constellation of AC injuries as anteromedial dome impaction especially in the geriatric acetabular fractures [3]. In both clinical situations, it is considered an ominous prognostic radiological sign. Anteromedial dome impaction can be addressed via the AIP approach by mobilizing the quadrilateral surface or by osteotomy at the AC fracture. When the I-I approach is used the impaction can be reduced through the AC fracture or via an osteotomy of the iliac bone. Lefaivre et al. [4] described a case of modified S-P approach for a fixation of anterior column/anterior dome fracture. Nevertheless, the authors used an additional tricortical osteotomy of the iliac crest to gain better exposure. In addition, the fixation of the dome fracture was performed with interfragmentary screws placed after the reduction of the main cortical fragment. In our case, the well-described technique of “two-level” reconstruction that is used in posterior wall fractures was employed [5].
Our case illustrates that a modified S-P approach along with ASIS osteotomy offers an efficient method of reducing and fixing anterior marginal impaction acetabular fractures in selected cases using the two-level reconstruction dome technique. Surgeons who are practising such surgery should be aware of this option.
Marginal impaction is a negative prognostic sign of acetabular fractures. A modified S-P approach along with ASIS osteotomy is an effective alternative of reducing and fixing anterior marginal impaction acetabular fractures in selected cases, utilizing the two-level reconstructions of the dome technique. Surgeons who are practising such surgery should be aware of this option.
References
- 1.Sheean AJ, Hurley RK, Collinge CA, Beltran MJ. Increased anterior column exposure using the anterior intrapelvic approach combined with an anterior superior iliac spine osteotomy: A cadaveric study. J Orthop Trauma 2017;31:565-9. [Google Scholar]
- 2.Sagi HC, Bolhofner B. Osteotomy of the anterior superior iliac spine as an adjunct to improve access and visualization through the lateral window. J Orthop Trauma 2015;29:e266-9. [Google Scholar]
- 3.Tosounidis TH, Stengel D, Giannoudis PV. Anteromedial dome impaction in acetabular fractures: Issues and controversies. Injury 2016;47:1605-7. [Google Scholar]
- 4.Lefaivre KA, Starr AJ, Reinert CM. A modified anterior exposure to the acetabulum for treatment of difficult anterior acetabular fractures. J Orthop Trauma 2009;23:370-8. [Google Scholar]
- 5.Giannoudis PV, Tzioupis C, Moed BR. Two-level reconstruction of comminuted posterior-wall fractures of the acetabulum. J Bone Joint Surg Br 2007;89:503-9. [Google Scholar]





