
Any intraoperative complication, most important thing is to stay cool and keep thinking.
Dr. Rajan Toor, Department of Orthopaedics, Holy Spirit Hospital, Mumbai, Maharashtra, India. E-mail: dr.rajantoor@gmail.com
Introduction:Intramedullary (IM) nailing is a well-established method of treating closed tibia shaft fracture. We hereby describe an unusual incidence of the incarceration of the flexible IM reamer in the distal fracture fragment with breakage of the coiled shaft of the reamer in the proximal third of tibia during closed IM nailing. This case report highlights the usefulness of making a small window in the tibia to aid retrograde removal of incarcerated reamer.
Case Presentation:A 26-year-old male patient had road traffic accident and sustained a close fracture of the right distal 3rd tibia along with segmental fracture of the adjacent fibula. The tibia nailing was done under combined spinal and epidural anesthesia. The proximal tibia was approached by a midline incision with splitting of the patellar tendon. The reduction of the fracture fragments was done and the guide wire was inserted. The medullary canal was narrow and hence the initial reaming was started with the smallest available, that is, 8 mm reamer. After crossing the fracture site, we noticed that reamer coiled shaft got broken into multiple pieces in the medullary cavity at proximal 3rd tibia. The fracture site was exposed and a linear osteotomy was done in distal tibial fragment. Through this window, the broken reamer was pushed in the retrograde manner and was delivered out. Most of the broken metal pieces of the reamer shaft were removed with pituitary rongeur. An 8 mm solid IM nail was passed in antegrade manner across the fracture site and was locked distally and proximally. The operative wounds were irrigated and closure was done in layers. The patient was allowed partial weight bearing at 3 weeks post-surgery with gradually progressing to full weight bearing at 10 weeks after confirming clinical and radiological union.
Conclusion:To handle this unusual occurrence one needs to stay calm, make a small window to aid retrograde removal of reamer and remove the fragmented pieces of the coiled shaft of the reamer. In tight medullary canal, it is desirable to have smaller diameter reamers, that is, 6 mm during the surgery.
Keywords:Tibia shaft fracture, Impacted flexible intramedullary reamer, Broken coiled reamer shaft, SIGN nail.
Intramedullary (IM) nailing is a well-established and preferred method of treating long bone fractures. IM nailing of the tibia requires reaming of the medullary canal. Serial IM reaming enlarges the medullary canal thereby allowing use of larger diameter IM nail. Larger diameter IM nail has a higher stiffness with a better fatigue strength. Complications associated with the reamer are very rare. Search of the literature shows two case reports of the breakage of the rigid reamer during IM tibia nailing [1] and during Total Knee Arthroplasty [2]. Low et al. [3] have described incarceration of the flexible IM reamer during the closed nailing of the femur with method of removal of such reamer. Darowish et al. [4] have described a catastrophic IM fragmentation of a tinel reamer. We hereby describe an unusual occurrence of the incarceration of the flexible IM reamer with breakage of the coiled shaft of the reamer during closed IM nailing of the tibia. We also describe the rescue efforts in removing the impacted reamer with the broken coiled shaft pieces of the reamer and completion of the IM nailing surgery of the tibia. To the best of our knowledge, this unusual occurrence has not been reported in the literature by far.
A 26-year-old male patient had road traffic accident and sustained a close fracture of the right tibia along with segmental fracture of the adjacent fibula. The patient also had a fracture of the base of 5th metatarsal left foot. The right tibia was fractured at the junction of middle 1/3rd and lower 1/3rd shaft with a lateral butterfly fragment (Fig. 1). The tibia nailing was undertaken at tertiary care hospital for the said patient under combined spinal and epidural anesthesia. The proximal tibia was approached by a midline incision with splitting of the patellar tendon. The reduction of the fracture fragments was achieved and confirmed on the image intensifier on antero-posterior (AP) and lateral projections. The guide wire was inserted and passed across the fracture site which was confirmed on AP and lateral projection on the image intensifier. The medullary canal was narrow and hence the initial reaming was started with the smallest available, that is, 8 mm reamer. The reamer was noted to pass the fracture site and entered the medullary cavity of the distal fracture fragment which was confirmed on image intensifier (Fig. 2). At this juncture, the reamer stopped progressing further. On visualization with image intensifier, to our surprise we noticed that the reamer coiled shaft got broken into multiple pieces in the medullary cavity at the junction of upper 1/3rd and middle 1/3rd tibia about 8 cm from the tip of the reamer (Fig. 3).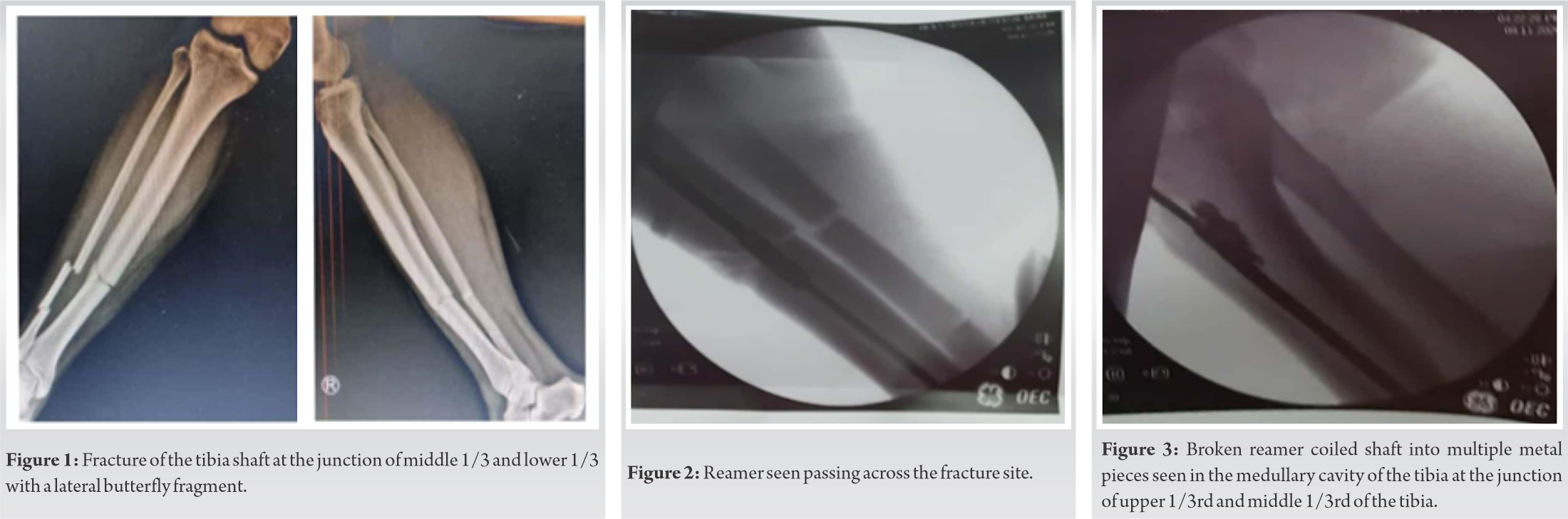 As there was no way the broken reamer could have been removed from the top of the tibia, decision was made to expose the fracture site. The fracture site was exposed with a vertical incision. A linear osteotomy (5 × 2 cm) was done in distal tibial fragment without disturbing the anterior and medial border to make a small window keeping intact the soft tissue attachment. Through this window the broken reamer was pushed in the retrograde manner and was delivered out through the opening made in the proximal tibia. Most of the broken metal pieces of the reamer shaft were removed through the proximal tibia opening with pituitary rongeur. An 8 mm solid IM nail (SIGN nail, www.signfracturecare.org) was passed in antegrade manner across the fracture site. The nail was locked distally with two screws and proximally with one screw in dynamic mode (Fig. 4). The reduction and fixation of the fracture was confirmed on image intensifier. The operative wounds were irrigated with normal saline + povidone iodine solution and closed in layers with absorbable sutures for deeper tissues and skin was approximated with skin stapler. The patient was allowed partial weight bearing on the operated leg at 3 weeks post-surgery gradually progressing to full weight bearing at 10 weeks after confirming clinical and radiological union (Fig. 5).
As there was no way the broken reamer could have been removed from the top of the tibia, decision was made to expose the fracture site. The fracture site was exposed with a vertical incision. A linear osteotomy (5 × 2 cm) was done in distal tibial fragment without disturbing the anterior and medial border to make a small window keeping intact the soft tissue attachment. Through this window the broken reamer was pushed in the retrograde manner and was delivered out through the opening made in the proximal tibia. Most of the broken metal pieces of the reamer shaft were removed through the proximal tibia opening with pituitary rongeur. An 8 mm solid IM nail (SIGN nail, www.signfracturecare.org) was passed in antegrade manner across the fracture site. The nail was locked distally with two screws and proximally with one screw in dynamic mode (Fig. 4). The reduction and fixation of the fracture was confirmed on image intensifier. The operative wounds were irrigated with normal saline + povidone iodine solution and closed in layers with absorbable sutures for deeper tissues and skin was approximated with skin stapler. The patient was allowed partial weight bearing on the operated leg at 3 weeks post-surgery gradually progressing to full weight bearing at 10 weeks after confirming clinical and radiological union (Fig. 5).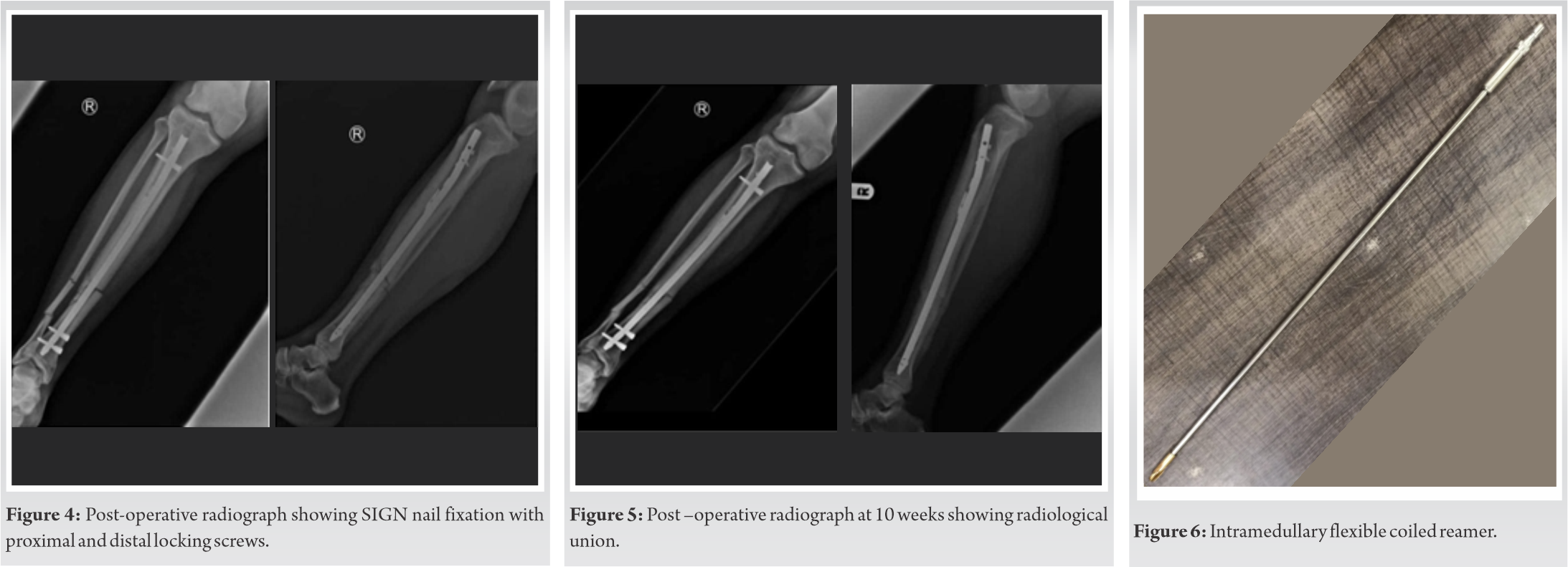
Tibia diaphysis fractures are the most commonly encountered long bone fractures by the orthopedic surgeons. IM nailing is the procedure of choice for these fractures. Medullary canal reaming is required so that larger diameter IM implant can be used. Larger diameter IM nail provides more stable fixation by increasing the contact area between the IM implant and the host bone. IM reaming of the tibia allows accumulation of the autologous bone graft and growth factors at the fracture site. These advantages of the reamed IM nail have shown to result in low rates of nonunion/delayed union, fewer reoperations, and faster time to union and weight bearing resulting in earlier return to work. IM tibia nail breakage is a well-documented complication and various methods to remove the broken piece are described in the literature [5, 6, 7, 8, 9, 10]. IM instrument breakage during IM nailing is rare. To the best of our knowledge, the impaction of the flexible IM reamer with breakage of the coiled shaft of the reamer during closed IM nailing of the tibia has not been described. Such unusual occurrence during the closed IM tibia nailing surgery causes extra struggle, heightened stress of the operating team. It also adds to the surgical and tourniquet time thereby increasing possibility of surgical infection. These factors may affect the course of patient’s post-operative recovery. The possible explanation for the breakage of reamer is that once the cutting reamer is jammed in the diaphysis of the shaft the torque will get concentrated at the vulnerable/ fatigued area of the coiled reamer thereby putting excessive stress on the coiled shaft of the reamer (Fig. 6). When encountered with tight medullary canal, it is desirable to have smaller diameter reamers i.e., 6 mm during the surgery. One needs to start reaming with a smaller diameter (6 mm) reamer. We managed to handle this unusual occurrence by staying stay calm, making a small window to aid retrograde removal of reamer and removing the fragmented pieces of the coiled shaft of the reamer with the help of pituitary rongeur.
In tight medullary canal, it is desirable to start reaming with smaller diameter reamers, that is, 6 mm reamer. Furthermore, it raises the question whether the flexible reamers should have a definite life as multiple uses decrease the fatigue strength of reamers.
While nailing the tibial fractures with anticipated tight medullary canal, it is advisable to start with a smaller diameter reamer, that is, 6 mm. Furthermore, it is advantageous to have tip cutting reamers to start with in situation of tight medullary canal.
References
- 1.Rijal L, Manandhar H, Nepal P, Ansari MT, Yadhav CS. Instrument fails, but surgeon should not. Surgical techniques for retrieval of broken intramedullary reamer from tibia. Eur J Orthop Surg Traumatol 2010;20:505-7. [Google Scholar]
- 2.Bisbinas I, Ho YM, Learmonth DJ. Reamer breakage in the femoral medulla during total knee arthroplasty: Should reamers have a finite life? J Arthroplasty 2004;19:501-3. [Google Scholar]
- 3.Low TH, Loke YH, Chiu CK. Minimally invasive retrieval of incarcerated flexible intramedullary reamer. Eur J Orthop Surg Traumatol 2012;22:113-5. [Google Scholar]
- 4.Darowish M, Gorczyca JT. Catastrophic intramedullary fragmentation of a tinel reamer. J Trauma 2009;67:E36-40. [Google Scholar]
- 5.Giannoudis PV, Matthews SJ, Smith RM. Removal of the retained fragment of broken solid nails by the intra-medullary route. Injury 2001;32:407-10. [Google Scholar]
- 6.Brewster NT, Ashcroft GP, Scotland TR. Extraction of broken intramedullary nails: An improvement in technique. Injury 1995;26:286. [Google Scholar]
- 7.Charnley GJ, Farrington WJ. Laparoscopic forceps removal of a broken tibial intramedullary nail. Injury 1998;29:489-90. [Google Scholar]
- 8.Incavo SJ, Kristiansen TK. Retrieval of a broken intramedullary nail. Clin Orthop Relat Res 1986;210:201-2. [Google Scholar]
- 9.Levine JW, Georgiadis GM. Removal of a broken cannulated tibial nail: A simple intramedullary technique. J Orthop Trauma 2004;18:247-9. [Google Scholar]
- 10.Oberst M, Holz U. Intramedulläre knochenendoskopie. Unfallchirurg 2005;108:75-8. [Google Scholar]





