
Total humeral replacement can be one of the treatment options in cases where nonunion surgery is extremely difficult, considering the patient’s age and activities of daily living.
Dr. Takahiro Niikura, Department of Orthopaedic Surgery, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-cho, Chuo-ku, Kobe 650-0017, Japan. E-mail: tniikura@med.kobe-u.ac.jp
Introduction:We report a very rare case of nonunion with ballooning deformity of the humeral bone after a periprosthetic humeral fracture nonunion.
Case Report: A 79-year-old woman underwent hemiarthroplasty 19 years ago for her proximal humerus fracture. She injured her right humeral diaphysis (stem distal end fracture) 6 years ago. She underwent revision hemiarthroplasty with long stem, but bony union was not obtained, and her right upper limb function was subsequently abolished due to extreme instability and pain in her right upper arm. She was then referred to our hospital for further treatment. X-ray showed nonunion in the humeral diaphysis and a severe ballooning deformity in the distal humeral bone fragment. Due to the advanced age and low activity of the patient, we chose total humerus replacement surgery instead of osteosynthesis. After the surgery, her upper arm pain and instability immediately improved. Three years after the last surgery, there have been no implant failures, and the upper arm is stable and painless.
Conclusion:Although there are some reports of total humerus replacement as surgical treatment for humeral tumor and severe periprosthetic fracture, we found no reports of such ballooning deformity around the nonunion site. Total humerus replacement can be one of the treatment options in cases where nonunion surgery is extremely difficult, depending on the patient’s age and activities of daily living.
Keywords:Ballooning deformity, nonunion, periprosthetic fracture, total humeral replacement.
As the elderly population increases, the number of arthroplasty cases has been growing in recent years [1]. Along with that, the number of periprosthetic fractures is increasing. Periprosthetic fractures are often more difficult to treat than normal fractures, and we often encounter non-unions and re-fractures after surgery [2]. That are difficult to treat. We report a rare case of nonunion in which the humeral bone exhibited severe ballooning deformity after nonunion around the hemiarthroplasty stem.
A 79-year-old woman presented with right upper arm pain and instability. She underwent a cementless hemiarthroplasty at another hospital for her proximal humerus fracture, when she had a motorcycle accident 19 years ago. Ten years later, she had a motorcycle accident again and suffered a fracture around her right humerus stem distal end, and revision surgery with a cementless long stem hemiarthroplasty was performed at the former hospital. Regular follow-up for 8 years, but bone union was not obtained, and she was referred to our hospital for further treatment because of her right arm pain and dysfunction. She has a history of diabetes mellitus (HgbA1c 6.7%). Physical findings at the first visit to our hospital were swelling and pain in the right humerus. Active movement of her shoulder joint was 10° of flexion, 5° of extension, and 10° of abduction. Her nonunion site was unstable and had minimal function. X-ray at the time of referral showed a nonunion at the fracture and a severe ballooning deformity in the distal bone fragment (Fig. 1a).Computed tomography showed similar findings, and a thinned bone cortex was found at the same site (Fig. 1b). 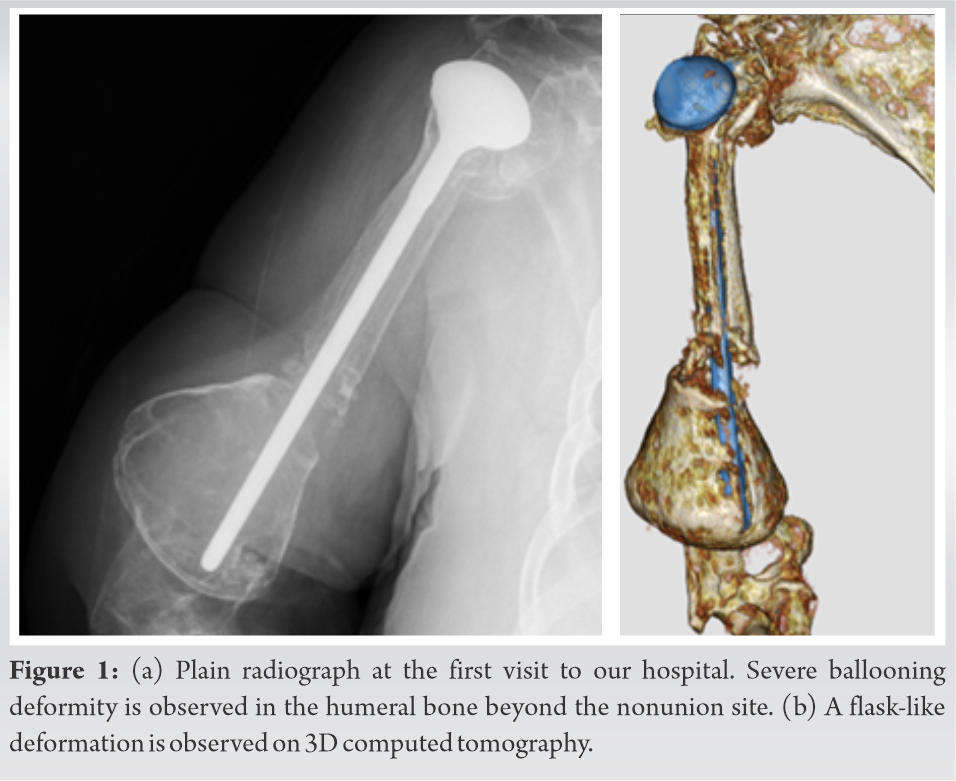
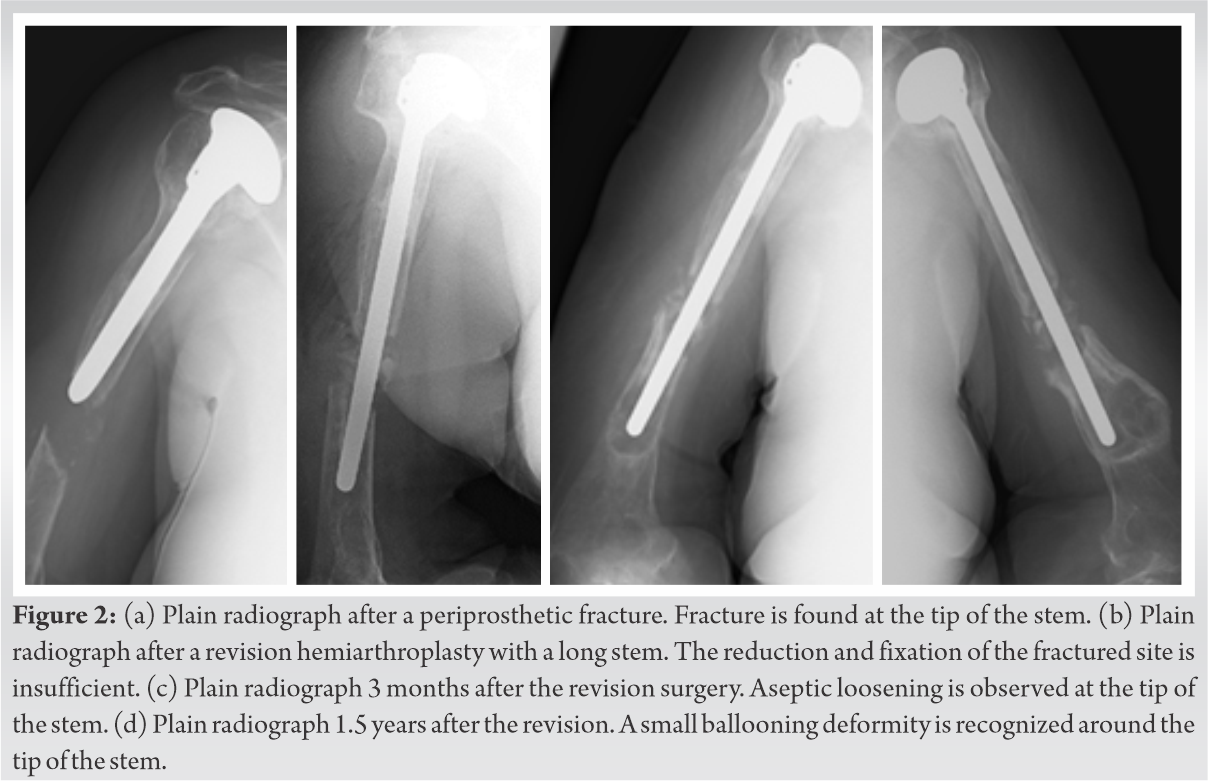 When we observed the images from the previous hospital for confirmation, we found that the ballooning deformation was gradually progressive (Fig. 2). We decided that nonunion surgery was difficult and chose total humerus replacement (Stryker Howmedica Modular Resection System) (Fig. 3).
When we observed the images from the previous hospital for confirmation, we found that the ballooning deformation was gradually progressive (Fig. 2). We decided that nonunion surgery was difficult and chose total humerus replacement (Stryker Howmedica Modular Resection System) (Fig. 3). 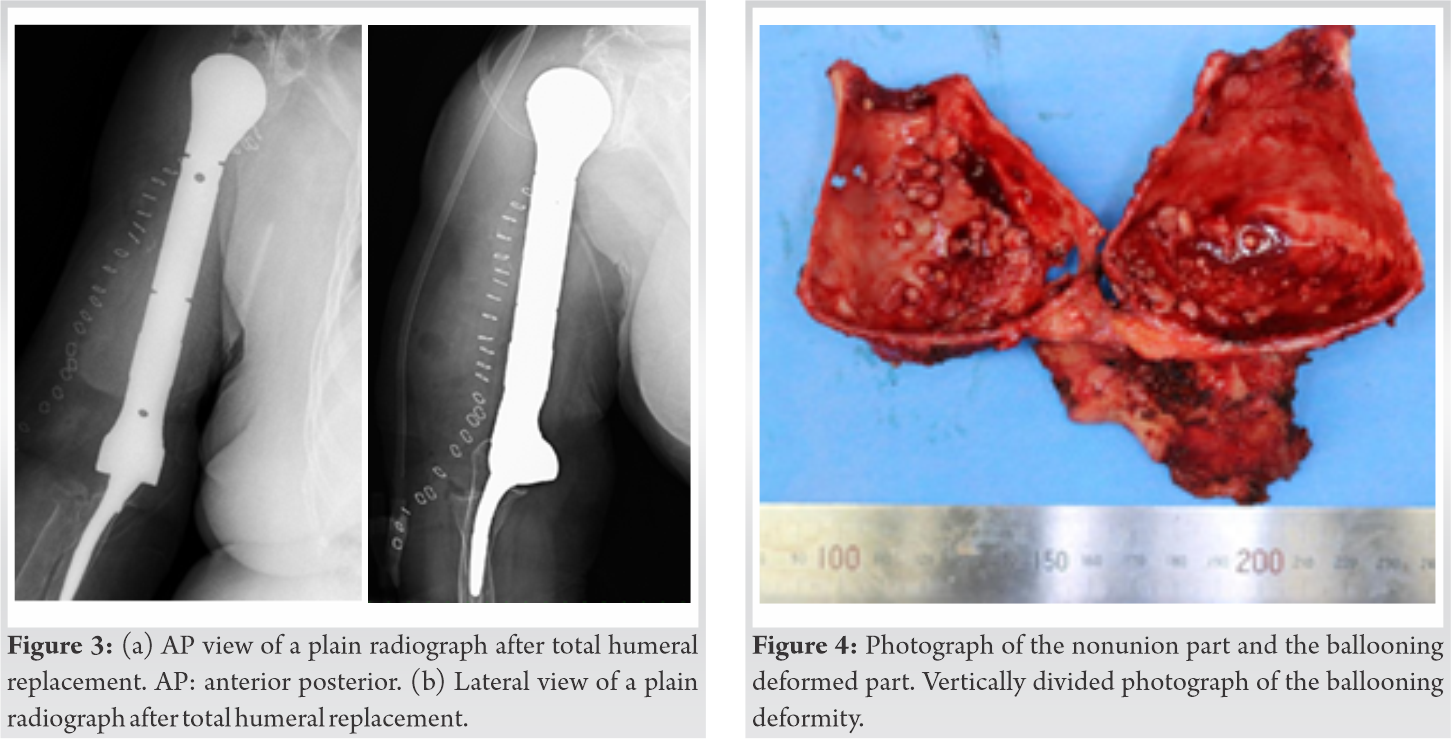 Surgical findings confirmed the nonunion and ballooning deformity of the distal humeral bone fragment and the cavity inside it (Fig. 4). No malignancy was found histopathologically in the deformed part of the ballooning. Three years after the total humeral replacement surgery, the patient has a stable upper arm and no pain. There was a slight improvement in active movement of her shoulder joint, but elbow joint function is maintained (Fig. 5).
Surgical findings confirmed the nonunion and ballooning deformity of the distal humeral bone fragment and the cavity inside it (Fig. 4). No malignancy was found histopathologically in the deformed part of the ballooning. Three years after the total humeral replacement surgery, the patient has a stable upper arm and no pain. There was a slight improvement in active movement of her shoulder joint, but elbow joint function is maintained (Fig. 5).  She is happy with her stable and painless upper arm.
She is happy with her stable and painless upper arm.
There are some reports on the treatment of non-unions for periprosthetic humerus fracture. If there is no looseness in the prosthesis, performing internal fixation by using a locking plate is recommended. If there is looseness, revision with a longer stem by using a plate and/or bone graft is recommended [3]. There are some reports recommending revision using strut bone allograft and internal fixation using a plate or cable system when the bone is fragile due to loosening [4, 5, 6]. In this case, as well, we examined options including osteosynthesis using bone grafts such as autograft and allograft. However, we decided that osteosynthesis was difficult due to the severe ballooning deformity and the patient’s age and activities of daily living, and we performed total humeral replacement instead. The number of cases of total humeral replacement for tumor patients is increasing [7, 8]. In addition, case reports of total humeral replacement are also found in treatments for conditions other than tumors, such as periprosthetic fractures in patients with rheumatism [9]. In this case, total humeral replacement was performed on humeral nonunion with severe ballooning deformity. There are few reports of aseptic loosening around elbow replacement [10], but to the best of our knowledge, there has not been a report of severe ballooning deformity as in this case. It is presumed that the stem continued to move in the distal bone fragment as a result of the lack of fixation around the stem and the continued instability caused by the nonunion.
A total humeral replacement was performed on a nonunion around the periprosthetic humeral fracture that had ballooning deformity. Total humeral replacement can be a treatment option for some non-unions such as in this case.
Total humeral replacement can be one of the treatment options in cases where nonunion surgery is extremely difficult, considering the patient’s age and activities of daily living.
References
- 1.Kurtz S, Ong KL, Lau E, Mowat F, Halpern H. Projections of primary and revision hip and knee arthoplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 2007;89:780-5. [Google Scholar]
- 2.Capone A, Congia S, Civinini R, Marongiu G. Periprosthetic fractures: Epidemiology and current treatment. Clin Cases Miner Bone Metab 2017;14:189-96. [Google Scholar]
- 3.O’Driscoll SW, Morrey BF. Periprosthetic fractures about the elbow. Orthop Clin North Am 1999;30:319-25. [Google Scholar]
- 4.Sanchez-Sotelo J, O’Driscoll SW, Morrey BF. Periprosthetic humeral fractures after total elbow arthroplasty: Treatment with implant revision and strut allograft augmentation. J Bone Joint Surg Am 2002;84:1642-50. [Google Scholar]
- 5.Jo YH, Lee SG, Kook I, Lee BG. Intramedullary fibula strut bone allograft in a periprosthetic humeral shaft fracture with implant loosening after total elbow arthroplasty. Clin Shoulder Elb 2020;23:152-5. [Google Scholar]
- 6.Andersen JR, Williams CD, Cain R, Mighell M, Frankle M. Surgically treated humeral shaft fractures following shoulder arthroplasty. J Bone Joint Surg Am 2013;95:9-18. [Google Scholar]
- 7.Gosheger G, Gebert C, Ahrens H, Steitbuerger A, Winklelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res 2006;450:164-71. [Google Scholar]
- 8.Bernthal NM, Upfill-Brown A, Burke ZD, Greig D, Hwang R, Crawford B, et al. Long term outcomes of total humeral replacement for oncological reconstructions: A single institution experience. J Surg Oncol 2020;122:778-86. [Google Scholar]
- 9.Tanagho A, Morgan B, Ravenscroft M. Total humeral endoprosthesis replacement to salvage periosthetic fractures in rheumatoid arthritis. Orthopedics 2017;40:e363-6. [Google Scholar]
- 10.Rhee YG, Cho NS, Parke CS. Impaction grafting in revision total elbow arthroplasty for aseptic loosening and bone loss. J Bone Joint Surg Am 2013;95:e741-7. [Google Scholar]








