
Not only congenital but also developmental pathogenesis should be considered for hypoplasia of the anterior portion of the vertebral body.
Dr. Kohei Takahashi, Department of Orthopaedic Surgery, Tohoku University School of Medicine, 1-1 Seiryo-machi, Aoba-ku, Sendai 980-8574, Japan. E-mail: kohei.takahashi.c1@tohoku.ac.jp
Abstract
Introduction: Hypoplasia of the anterior portion of the vertebral body is a relatively rare subtype of juvenile vertebral deformity. The common manifestations of this type of deformity are scoliosis and kyphoscoliosis, while kyphosis without scoliosis is rare. Here, we present a very rare case of adolescent-onset local kyphosis with anterior column hypoplasia and subluxation of the facet joints of the lumbar spine, as demonstrated by dynamic lateral radiograms, which was successfully treated by spine-shortening osteotomy.
Case Report: A 16-year-old male adolescent presented with low back pain with progressive protrusion of the lumbar spinous process 3 years before the first visit. The protrusion was not found in his back until the age of 13 years. His chief complaint was lower back pain and a protruding spinous process in the upper lumbar spine. The anteroposterior radiogram of the whole spine revealed no obvious scoliosis. The lateral radiogram showed hypoplasia of the anterior portion of the L2 vertebral body with local kyphosis at L1–3 of 23°. The global alignment was posteriorly shifted, with hypokyphosis of the thoracic spine and hyperlordosis of the lower lumbar spine. In the dynamic lateral radiograms, the facet joints at the L2–3 spinal level were subluxated in the flexed position. Computed tomography showed symmetrical hypoplasia of the anterior portion of the vertebral body of L2. Spine-shortening osteotomy at L2 and L1–3 posterior fusion was performed for local stabilization and correction of sagittal malalignment. The lateral radiogram at the 2-year post-operative follow-up demonstrated that the global alignment was normal, with local kyphosis at L1–3 of -2°. The improvement of hypokyphosis of the thoracic spine and hyperlordosis of the lower lumbar spine was achieved.
Conclusions: Adolescent-onset local lumbar kyphosis with anterior column hypoplasia and segmental subluxation of the facet joints is very rare. Local correction by spine-shortening osteotomy with short fusion can also improve the global alignment.
Keywords: Anterior column hypoplasia, congenital, developmental, kyphosis.
Hypoplasia of the anterior portion of the vertebral body is a relatively rare subtype of juvenile vertebral deformity. The common manifestations of this type of deformity are scoliosis and kyphoscoliosis; while kyphosis without scoliosis is rare [1] McMaster et al. reported in their retrospective study that only 36 of 586 (6%) consecutive cases with congenital spinal deformity had pure kyphosis [1]. Infantile thoracolumbar segmental subluxation of the spine is another pathology that can present kyphosis without scoliosis, by hypoplastic vertebral body with subluxation at the corresponding spinal level. The diagnosis was made during infancy and the hypoplastic vertebral body was restored in all reported cases [2,3].
Here, we present a very rare case of adolescent-onset local lumbar kyphosis with anterior column hypoplasia and segmental subluxation of facet joints, as demonstrated by dynamic lateral radiograms, which was successfully treated by spine-shortening osteotomy with only two-spinal segment instrumented fusion. Written informed consent was obtained from the patient and his parents for publication of his clinical data.
A 16-year-old male adolescent presented with low back pain with progressive protrusion of the lumbar spinous process 3 years before the first visit. The protrusion in his back was not noticed from his neonatal period to early childhood by his parents, until it was discovered around the age of 13 years. After playing basketball caused his lower back pain to worsen, he visited a nearby clinic and was found to have an abnormality in the L2 vertebral body. The patient was then referred to our department. He had no medical history, including congenital diseases or spinal trauma. His chief complaint was lower back pain, which was exacerbated by exercise. He was 173 cm tall and weighed 60 kg at his first visit. The spinous process protruded in the upper lumbar spine, with tenderness in the bilateral paravertebral muscles at the same level. Neither symptoms in the lower extremities nor abnormal neurological findings were observed. The Japanese Orthopaedic Association (JOA) score for lumbar spinal disorders was 27 points out of 29.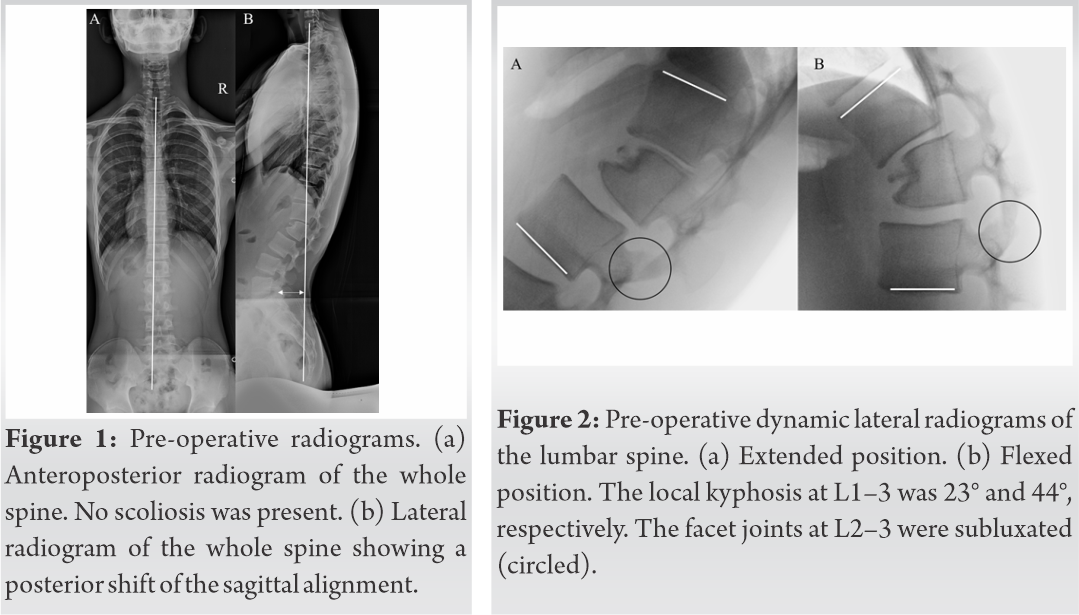
The anteroposterior (AP) radiogram of the whole spine revealed no obvious scoliosis, with bone maturity of Risser Grade 4 (Fig. 1a). The lateral radiogram of the whole spine showed hypoplasia of the anterior portion of the L2 vertebral body with a sagittal vertical axis (SVA) of −60 mm (Fig. 1b). The AP diameters measured at the center of the L1, L2, and L3 vertebral bodies were 36 mm, 27 mm, and 41 mm, respectively. The spinal parameters measured in the lateral radiogram were as follows: Thoracic kyphosis (TK) at T5–12, 17°; local kyphosis at L1–3, 23°; lumbar lordosis (LL) at L1–S1, 38°; LL at L3–S1, 59°; and pelvic incidence (PI), 34° (Fig. 1b). In the dynamic lateral radiograms, local kyphosis at L1–3 was 23° in the extended position (Fig. 2a) and 44° in the flexed position (Fig. 2b).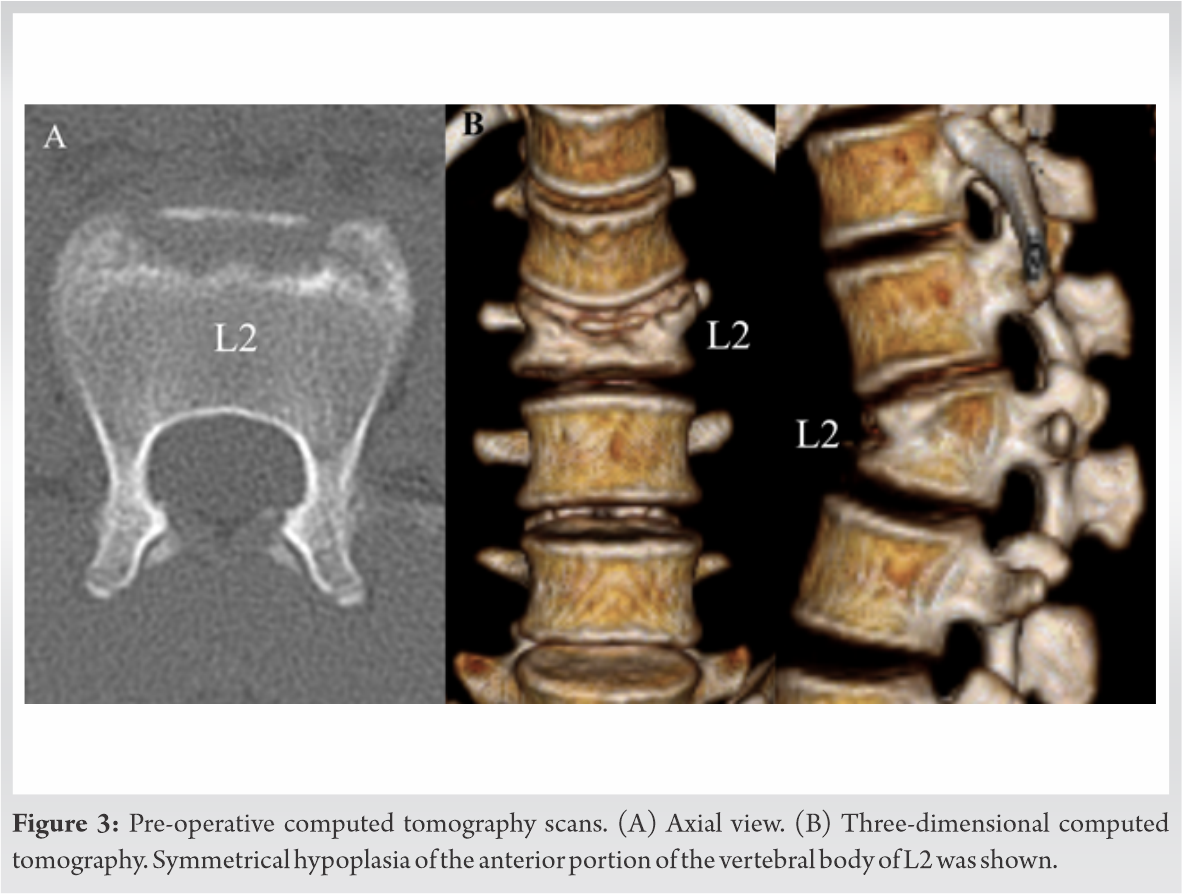 In addition, the facet joints at the L2–3 spinal level were subluxated in the flexed position (Fig. 2b). Computed tomography showed symmetrical hypoplasia of the anterior portion of the vertebral body of L2 (Fig. 3). Based on these radiological findings, the patient was diagnosed with L1–3 local kyphosis, with anterior column hypoplasia and subluxation of the facet joints at L2–3.
In addition, the facet joints at the L2–3 spinal level were subluxated in the flexed position (Fig. 2b). Computed tomography showed symmetrical hypoplasia of the anterior portion of the vertebral body of L2 (Fig. 3). Based on these radiological findings, the patient was diagnosed with L1–3 local kyphosis, with anterior column hypoplasia and subluxation of the facet joints at L2–3.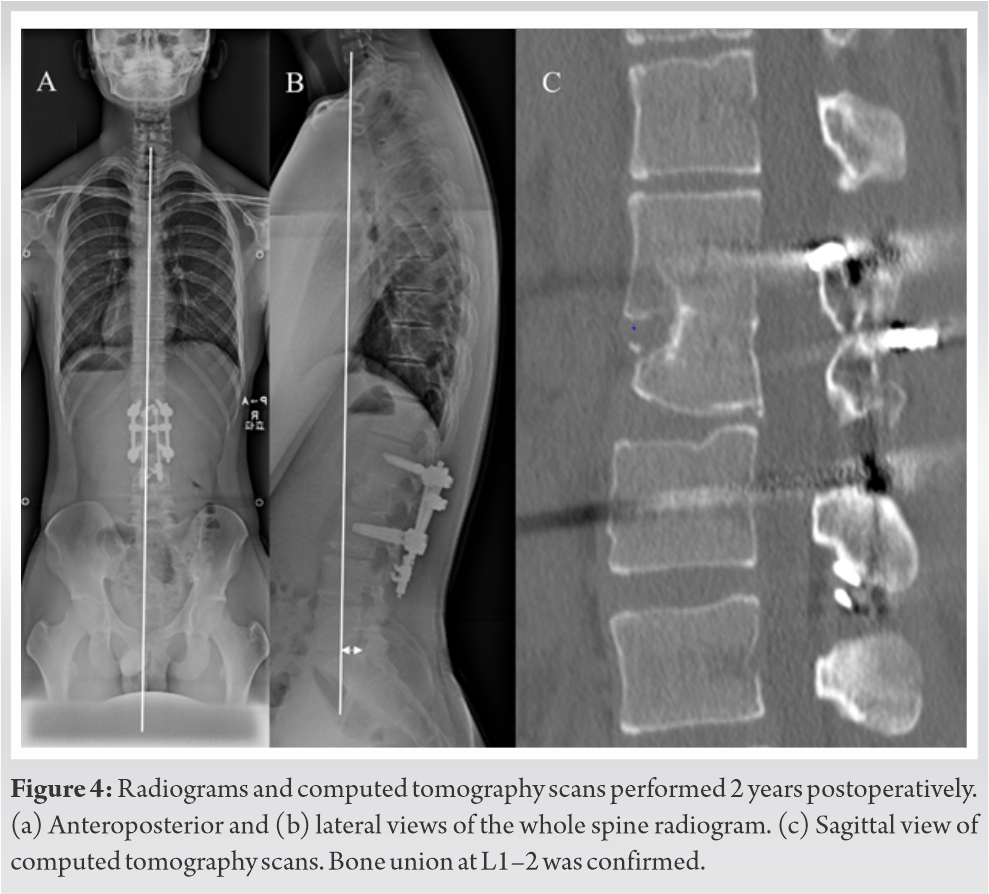
Spine-shortening osteotomy at L2 and L1–3 posterior fusion was performed for local stabilization and correction of the sagittal malalignment, using a pedicle screw and rod system with compression laminar hooks, as reported previously [4,5]. This procedure is equivalent to Grade-4 osteotomy by anterior column realignment classification [6]. First, the laminae and transverse processes of the L1–3 vertebrae were exposed. Polyaxial pedicle screws were placed bilaterally at the L1 and L3 vertebrae, parallel to each upper endplate (EXPEDIUM VERSE System®, DePuy Synthes, Raynham, MA). The lower half of the L1 lamina, the L1–2 facet joints, and the upper half of the L2 lamina were resected using a high-speed burr and chisels. Then, the upper half of the L2 pedicles was removed using a high-speed burr. Subsequently, a wedge-shaped osteotomy of the upper part of the L2 vertebral body was performed together with the removal of the L1–2 intervertebral disc. The wedge-shaped osteotomy was performed with the preoperatively designed osteotomy line, with the starting point at 8 mm caudal from the posterosuperior edge of the L2 vertebral body, cutting up toward the anterosuperior endplate at an angle of 30° to the lower endplate of L1 to set local kyphosis between L1 and L3 to 0° after correction. For correction, the screws were converted from polyaxial to monoaxial screws by semi-locking the set screws. After placing bilateral temporary rods on the screws, the posterior portions of the L1 and L3 vertebral bodies were compressed gradually using a hook system (DYNACORE®, Mizuho Corporation, Tokyo, Japan) [7]. The alignment and bone-on-bone contact were confirmed by fluoroscopy and the screws were connected to the final rods. Finally, autologous local bone pieces from the posterior vertebral elements were grafted between L1 and L3. A whole-spine AP radiogram at 2-year post-operative follow-up revealed no obvious scoliosis (Fig. 4a). The lateral radiogram demonstrated that SVA improved to 9 mm, TK to 35°, local kyphosis at L1–3 to −2°, LL to 40°, and LL at L3–S1 to 34° (Fig. 4b). In addition, bone union was confirmed at L1–2 vertebral bodies by computed tomography (Fig. 4c). His lower back pain was completely relieved and his JOA score showed a maximum 29 points. Two years postoperatively, the patient had no symptoms, bony fusion was completed, and no correction loss was detected.
The major etiologies of juvenile thoracolumbar segmental kyphosis are congenital kyphosis, and infantile kyphosis with segmental subluxation. McMaster et al. stated that congenital kyphosis is potentially more harmful than congenital scoliosis, with a higher chance of developing spinal cord compression resulting in paraplegia [1]. They also defined the complete failure of formation of the anterior portion of the vertebral body as posterior hemivertebra, which presents sharply angled kyphosis with minor scoliosis of <20°. In their study, four cases of single posterior hemivertebra were reported in 112 consecutive patients with congenital kyphosis or kyphoscoliosis. These anomalies all occurred in the lower thoracic spine and were associated with severe kyphosis of 40° or more at the initial presentation or during follow-up. Among the four cases, two were diagnosed at birth, one at 3 years of age, and one after skeletal maturity. They also reported two cases with a single-wedged vertebra of patients aged 11 and 17 years. However, no detailed information about these cases of adolescents was noted in the report; therefore, the similarity between them and the present case was uncertain. Another entity, infantile developmental thoracolumbar kyphosis with segmental subluxation of the spine, is pathology reported only in the first and second lumbar vertebrae and is occasionally diagnosed during infancy [2,3]. Considering that the hypoplastic vertebrae were restored after posterior spinal arthrodesis or conservative treatment in all reported cases, segmental subluxation could be a developmental condition due to segmental spinal instability. The hypoplastic anterior portion of the L2 vertebral body with intact posterior elements in the present case was similar to the features of posterior hemivertebra and infantile thoracolumbar kyphosis with segmental subluxation. Regrettably, this adolescent-onset vertebral deformity could not be confirmed to be congenital or developmental, since radiographic images at birth and during infancy were unavailable. Meanwhile, according to the observation made by the patient’s parents, the protrusion in his back is supposed to have newly arisen around the age of 13 and became prominent during his growth period. Namely, anterior column hypoplasia, in this case, could be associated with developmental pathogenesis. To the best of our knowledge, adolescent-onset local kyphosis with anterior column hypoplasia and subluxation of the facet joints is rare and has not been precisely described in the previous reports. The disadvantage of segmental kyphosis of the upper lumbar area is not only the backward protrusion of the spinous process, but also consequent hyperlordosis of the lower lumbar spine. In the present case, the local kyphosis at L1–3 and spinal instability with facet joint subluxation at L2–3 were supposed to have required the hyperlordotic lower lumbar spine to maintain the upright standing position, resulting in a backward shift of the SVA. Hyperlordosis of the lumbar spine can cause irreversible degeneration of the facet joints, which could lead to recurring back pain in the future [8]. Surgical treatment is usually performed for this pathology because conservative treatment is ineffective after bone maturation [9].Several surgical procedures have been reported for thoracolumbar kyphosis, including instrumented posterior fusion, pedicle subtraction osteotomy, and posterior column resection [10,11]. Guo et al. reported a combination of forward shifting of the anterior column of the L1 wedge hemivertebra and circumferential fusion [12]. Including Guo’s procedure, all reported cases were treated with long spinal fusion. However, shorter spinal fusion would be suitable, if possible, especially in young, active patients. Then, L2 spine-shortening osteotomy with instrumented fusion between L1 and L3 using a pedicle screw/rod system with a compression laminar hook was chosen for the present case, in which, tethered cord syndrome was treated [4,5]. Local kyphosis was restored to almost 0°, and consequently, hyperlordosis in the lower lumbar spine improved and SVA moved from −60 mm to 9 mm postoperatively. Two years postoperatively, the patient had no symptoms, bony fusion was completed, and no correction loss was detected.
Adolescent-onset local lumbar kyphosis with anterior column hypoplasia and segmental subluxation of the facet joints is very rare. Local correction by spine-shortening osteotomy with short fusion can improve not only segmental kyphosis, but also the sagittal global alignment of the spinal column.
References
- 1.McMaster MJ, Singh H. Natural history of congenital kyphosis and kyphoscoliosis. A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-83. [Google Scholar | PubMed]
- 2.Tsirikos AI, McMaster MJ. Infantile developmental thoracolumbar kyphosis with segmental subluxation of the spine. J Bone Joint Surg Br 2010;92:430-5. [Google Scholar | PubMed]
- 3.Ganesan S, Karampalis C, Garrido E, Tsirikos AI. Infantile developmental thoracolumbar kyphosis with segmental subluxation of the spine: Report of five patients and review of the literature. Bone Joint J 2015;97:982-7. [Google Scholar | PubMed]
- 4.Kanno H, Aizawa T, Ozawa H, Hoshikawa T, Itoi E, Kokubun S. Spine-shortening vertebral osteotomy in a patient with tethered cord syndrome and a vertebral fracture. Case report. J Neurosurg Spine 2008;9:62-6. [Google Scholar | PubMed]
- 5.Kokubun S, Ozawa H, Aizawa T, Ly NM, Tanaka Y. Spine-shortening osteotomy for patients with tethered cord syndrome caused by lipomyelomeningocele. J Neurosurg Spine 2011;15:21-7. [Google Scholar | PubMed]
- 6.Uribe JS, Schwab F, Mundis GM, Xu DS, Januszewski J, Kanter AS, et al. The comprehensive anatomical spinal osteotomy and anterior column realignment classification. J Neurosurg Spine 2018;29:565-75. [Google Scholar | PubMed]
- 7.Wang B, Ozawa H, Tanaka Y, Matsumoto F, Aizawa T, Kokubun S. One-stage lateral rhachotomy and posterior spinal fusion with compression hooks for Pott’s paralysis in the elderly. J Orthop Surg (Hong Kong) 2006;14:310-4. [Google Scholar | PubMed]
- 8.Deane JA, Pavlova AV, Lim AK, Gregory JS, Aspden RM, McGregor AH. Is intrinsic lumbar spine shape associated with lumbar disc degeneration? An exploratory study. BMC Musculoskelet Disord 2020;21:433. [Google Scholar | PubMed]
- 9.Mayfield JK, Winter RB, Bradford DS, Moe JH. Congenital kyphosis due to defects of anterior segmentation. J Bone Joint Surg Am 1980;62:1291-301. [Google Scholar | PubMed]
- 10.Atici Y, Sökücü S, Uzümcügil O, Albayrak A, Erdoğan S, Kaygusuz MA. The results of closing wedge osteotomy with posterior instrumented fusion for the surgical treatment of congenital kyphosis. Eur Spine J 2013;22:1368-74. [Google Scholar | PubMed]
- 11.Zeng Y, Chen Z, Qi Q, Guo Z, Li W, Sun C, et al. The posterior surgical correction of congenital kyphosis and kyphoscoliosis: 23 cases with minimum 2 years follow-up. Eur Spine J 2013;22:372-8. [Google Scholar | PubMed]
- 12.Guo J, Guo Q, Li J, Fang Z, Liao H, Xiong W, et al. Wedge hemivertebra forward-shifting technique for treatment of congenital kyphosis: Case report, technical note, and literature review. World Neurosurg 2019;122:11-5. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2023 Non-metallic Fixation of Patella Fractures: A Paradigm Shift
August 10, 2023 Non-metallic Fixation of Patella Fractures: A Paradigm Shift February 10, 2024 Giant Cell Tumor of Patella with Secondary Aneurysmal Bone Cyst-A Rare Case Report of Anterior Knee Pain in Young Adults
February 10, 2024 Giant Cell Tumor of Patella with Secondary Aneurysmal Bone Cyst-A Rare Case Report of Anterior Knee Pain in Young Adults April 10, 2021 A Rare Case of Sphingomonas paucimobilis Spondylodiscitis Managed Surgically
April 10, 2021 A Rare Case of Sphingomonas paucimobilis Spondylodiscitis Managed Surgically January 1, 2025 Transformative Spinal Surgery: Lateral Position Unilateral Biportal Endoscopic Discectomy
January 1, 2025 Transformative Spinal Surgery: Lateral Position Unilateral Biportal Endoscopic Discectomy