
All patients who have undergone bipolar hemiarthroplasty even though they are asymptomatic should be followed closely for early diagnosis of erosive polyethylene induced fatigue failure of the outer metal dome of the monobloc shell of bipolar prosthesis
Dr. Sachin Upadhyay, Department of Orthopaedics, NSCB Medical College, Jabalpur, Madhya Pradesh, India. E-mail: drsachinupadhyay@gmail.com
Introduction: We report a rare case of transmural wear-through of the polyethylene inner liner leading to fatigue failure of polished outer metallic dome of bipolar monoblock shell in cemented hemiarthroplasty 5-years after the index surgery.
Case Presentation: A 62-year-old active man reported with 6 months of worsening right hip pain. He had undergone cemented bipolar hemiarthroplasty for sub-capital fracture of the right femur 5 years back. Radiographs demonstrate significant full-thickness wear-through of the Cobalt-Chromium head through the polyethylene inner liner and outer metal dome into the acetabulum. Biomechanics study revealed inadequate thickness of outer metallic dome of monoblock shell. Revision Total hip arthroplasty was performed. At the 5-year follow-up, radiographs show stable components and no clinical abnormality.
Conclusion: Albeit rare, this failure mode aimed to raised awareness, routine follow-up, and quality assurance.
Keywords: Bipolar hemiarthroplasty, revision total hip arthroplasty, bipolar monoblock shell, polyethylene inner liner.
Paralleling trends of demographic projections, the incidence of intra-capsular femoral neck fractures in elderly will continue to grow in near-future poses significant challenges. Due to the lack of consensus in the literature, it remains controversial whether to do hemiarthroplasty or otherwise primary total hip arthroplasty (THA) in these cases. Monoblock unipolar prosthesis though offered a cost-effective ambulatory alternative, were encountered with poor quality of life in the long-term follow-up [1]. Bipolar hemiarthroplasty has been widely used for the treatment of geriatric population femoral neck fractures owing to less wear of the metal-cartilage inter-face, low rate of dislocation, increased range of motion, and lesser morbidity. Outcomes from bipolar hemiarthroplasty are usually consistent; relieve pain, providing better functional outcome and patient satisfaction. However, in some cases the polyethylene liner between the inner and outer bearings interface is invariably recognized as the weak link in the THA prosthetic design; leads to failure of bipolar arthroplasty [2, 3, 4]. Although usually associated with ceramic heads, fatigue failure of bipolar metal-dome is much rarer. There remains paucity of literature showing fracture of bipolar outer metallic-dome inciting a significant deterioration of activity of daily living. To the authors’ knowledge, present report appears to represent a rare case of a full-thickness wear-through of the polyethylene liner leading to fatigue failure of outer metal-dome of monobloc shell in cemented bipolar hemiarthroplasty. Informed consent concerning the publication was taken.
A 62-year-old active (indulged in athletic activities), mobile and independent male presented to the outpatient department with 6 months of progressively worsening right hip pain. 5-years before his reporting, our patient underwent right side cemented bipolar hemiarthroplasty for fracture neck of femur elsewhere; the components included a cemented bipolar (Sony) stainless steel size 12.5 length 150 mm. There had been no post-operative complications. He had been advised to follow-up every 6–12 months but he was lost to follow up until he had agonizing right hip pain. The patient had not experienced any pain or issues with the right hip until about 6 months before the presentation when he began to notice the increase in pain with physical activity. In the ensuing months, he was able to continue his day-to-day activities. However, a month before the presentation, he noted a rapid worsening of the pain of the right hip, which makes ambulation more and more difficult. The pain occurred in the groin, buttock, and while abducting the leg. The examination was note worthy for severe pain with any movement, and there was leg-length discrepancy of 1 cm. Movements were painfully restricted. Standard antero-posterior and lateral radiograph revealed a stable femoral stem with complete wear-through of the femoral head through the inner polyethylene liner and the outer dome into the postero-superior weight-bearing roof of the osseous acetabulum. A piece of metal chip can also be seen at the margin of Bipolar Head (Fig. 1a, 1b).  The routine complete blood cell count and basic laboratory markers were within normal range. Given the severe pain and functional impairment, patient was counseled and assured for complete revision THA. After appropriate pre-operative planning, patient underwent right-side THA through the posterior approach. Upon entry into the hip capsule, there was a small amount of dark-colored metallic debris, which was thoroughly debrided and lavaged from the hip (Fig. 2).
The routine complete blood cell count and basic laboratory markers were within normal range. Given the severe pain and functional impairment, patient was counseled and assured for complete revision THA. After appropriate pre-operative planning, patient underwent right-side THA through the posterior approach. Upon entry into the hip capsule, there was a small amount of dark-colored metallic debris, which was thoroughly debrided and lavaged from the hip (Fig. 2).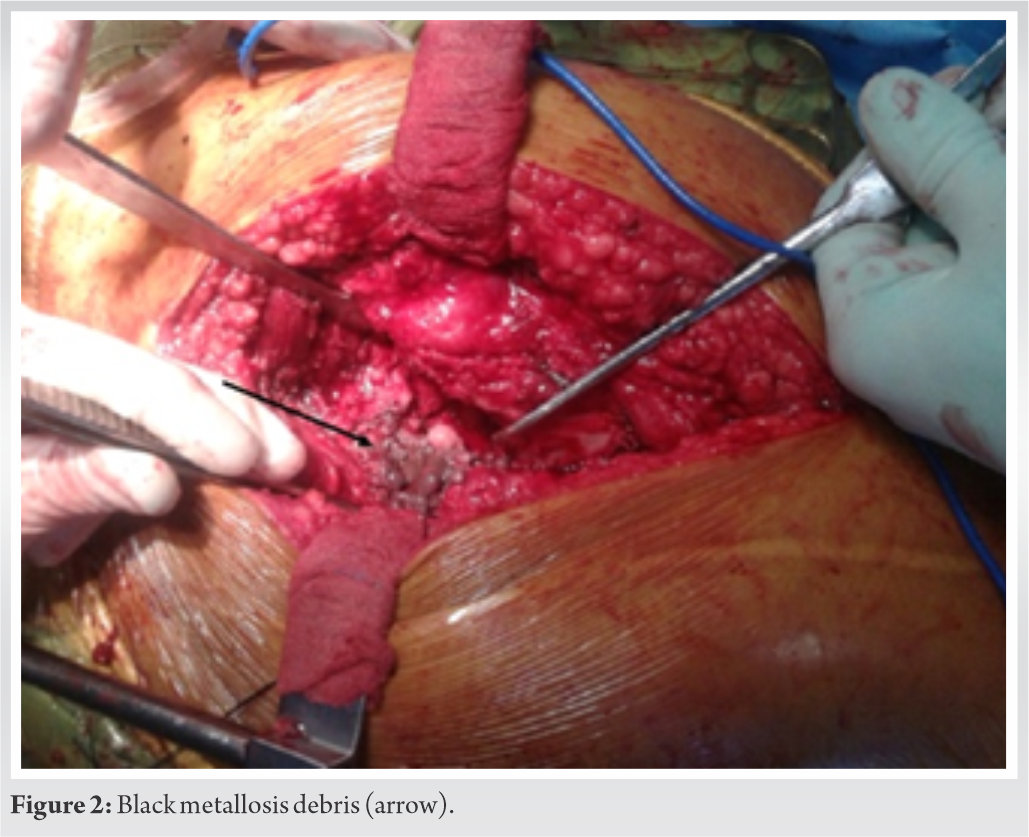 The bipolar head was dissociated and removed (Fig. 3). The femoral head component had almost no naked eye visible signs of wear. The cemented femoral stem was removed and cement removed through endo-femoral approach. Three microbiological specimens were taken for culture methods and gram staining. The Gram stain was negative, and all three culture specimens did not grow any organisms. The acetabulum was adequately reamed to bleeding bone. Trial component was checked for stability and finally, a 52 mm acetabular cup was implanted with 2 cancellous screws to augment fixation. A Duraloc cup (Depuy, Warsaw, Indiana) and a highly cross-linked polyethylene liner 28 mm with posterior lip were used. Femoral canal was reamed with solution reamers upto size 15 mm and fully coated solution stem (Depuy, Warsaw, Indiana) of size 13.5 mm was used. The polyethylene liner was impacted and a 28 mm metal femoral head (Depuy, Warsaw, Indiana) was impacted onto the femoral stem. The hip was reduced and stability checked. The closure was done in routine fashion and the patient was transferred to respective ward bed in stable condition. Post-op protocol was strictly followed.
The bipolar head was dissociated and removed (Fig. 3). The femoral head component had almost no naked eye visible signs of wear. The cemented femoral stem was removed and cement removed through endo-femoral approach. Three microbiological specimens were taken for culture methods and gram staining. The Gram stain was negative, and all three culture specimens did not grow any organisms. The acetabulum was adequately reamed to bleeding bone. Trial component was checked for stability and finally, a 52 mm acetabular cup was implanted with 2 cancellous screws to augment fixation. A Duraloc cup (Depuy, Warsaw, Indiana) and a highly cross-linked polyethylene liner 28 mm with posterior lip were used. Femoral canal was reamed with solution reamers upto size 15 mm and fully coated solution stem (Depuy, Warsaw, Indiana) of size 13.5 mm was used. The polyethylene liner was impacted and a 28 mm metal femoral head (Depuy, Warsaw, Indiana) was impacted onto the femoral stem. The hip was reduced and stability checked. The closure was done in routine fashion and the patient was transferred to respective ward bed in stable condition. Post-op protocol was strictly followed.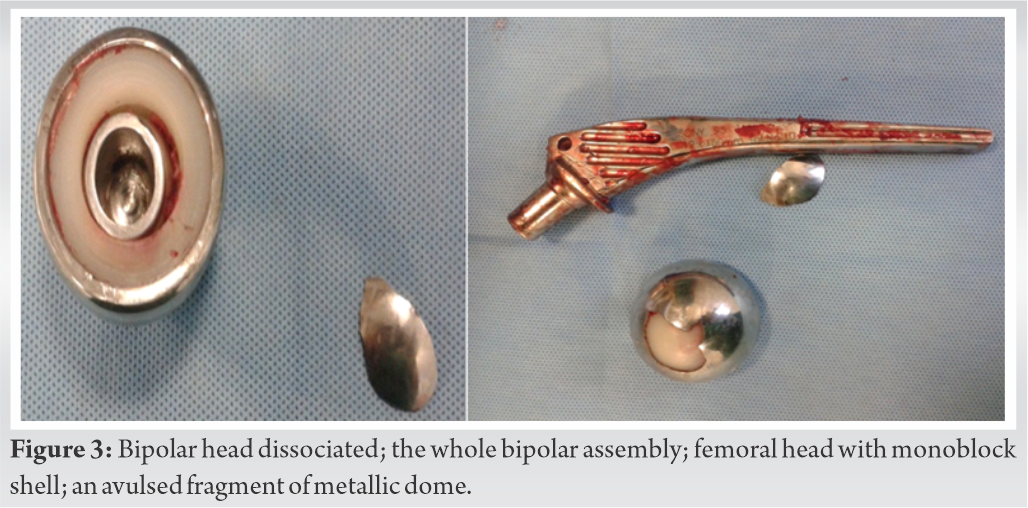
The bipolar monobloc shell was sent to our biomechanics laboratory for critical analysis (Fig. 4). Femoral head had penetrated total thickness of polyethylene, and also damaged metallic outer dome leading to fatigue failure. Metallic broken piece was identified and removed. There could be two possibilities of this catastrophic failure, one excessive wear and second thickness of metal case was in-adequate (metal defect).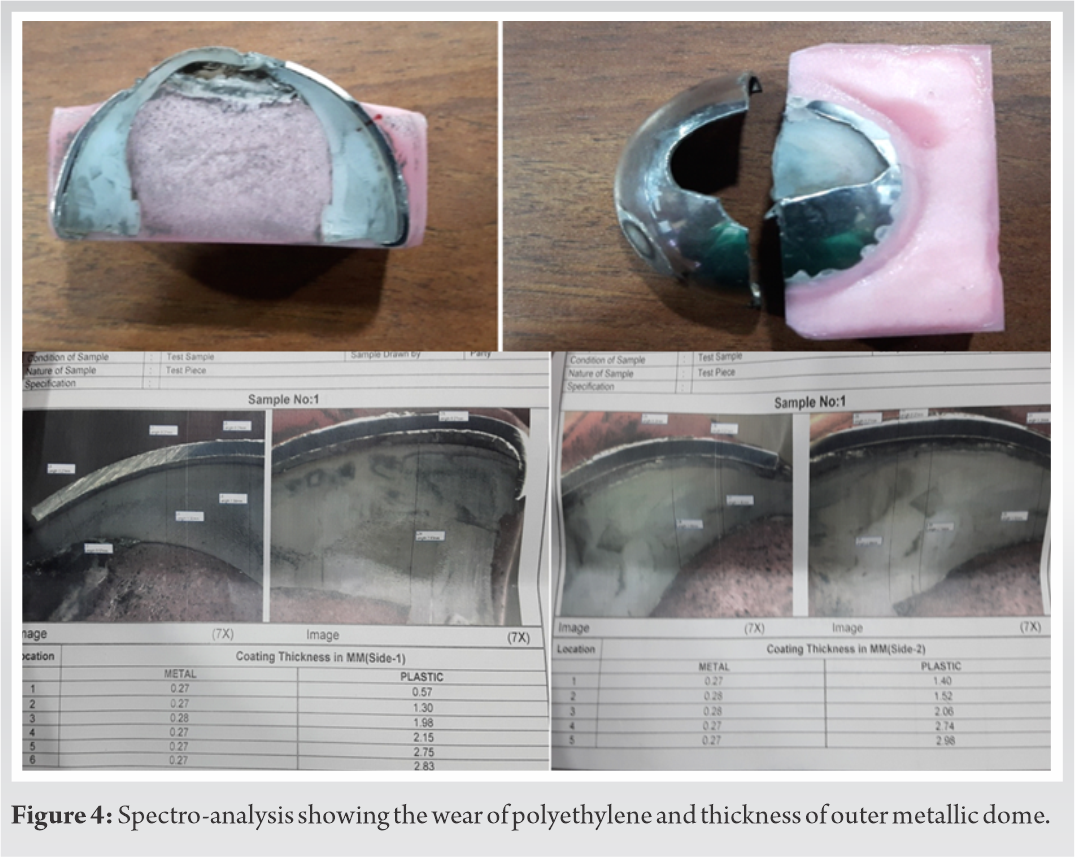
At 3 months after revision, he was allowed to do full weight-bearing walking and routine activities of daily living. His recovery was good. Few months postoperatively, he was pain free and had returned to his routine activities. During his last follow-up, 5-years post-surgery, Harris Hip score was improved from poor to excellent, radiographs show both components stable, and clinical examination did not reveal any abnormality (Fig. 5).
Compared with internal fixation, arthroplasty as a primary treatment for displaced femoral neck fractures in elderly populations has lower risk of long-term complications and re-operation rates [5]. Likewise, Keating et al. showed a clear advantage for arthroplasty over internal fixation in fit elderly patients [6]. However, what is still a matter of argument is the best ambulatory alternative for socially independent, alert, and active patient [7]. Patients with dependency and limited mobility simply do not require THA. Hemiarthroplasty is considered as an easier and simpler alternative to THA. However, owing to metal-cartilage articulation, acetabular cartilage erosion has a reported incidence of up to 5–24% [8]. Bipolar hemiarthroplasty is the preferred alternative for displaced intra-capsular fractures in geriatric population with low functional demands [7]. Bipolar hemiarthroplasty in active and socially independent patient exposed the prosthesis to early wear. Messieh et al., described wear debris originating from the femoral neck-cup impingement [9]. Similarly, other reports have illustrates acetabular osteolysis following bipolar hemiarthroplasty [10]. Polyethylene wears and subsequent osteolysis have also been noted as serious problems in bipolar hemiarthroplasty [3]. Factors such as oxidation, crystallization, and mechanical stress weaken the polyethylene and may lead to the production of polyethylene debris [11]. Polyethylene wear is a crucial factor that limits the longevity of bipolar hemiarthroplasty. Some of the available literature has reported cases of polyethylene failure following bipolar arthroplasty [2, 3, 4]. The presumed failure mechanism was attributed to mechanical design and cyclic loading of varus aligned cup. Overuse, obesity, and active lifestyle were associated factors. Bipolar components are also susceptible to bearing surface failure and its sequelae [3]. In the present report, the patient was relatively active before and after the index surgery. Patient had not returned for the recommended follow-up as he was pain free and had normal day-to-day activity. However, pain after few years which increased on prolong activity and later restricting mobilization lead the patient for further consultation. Delayed recognition of erosive polyethylene wear resulted in the need for complete THA. In this case, we did complete revision inspite of stable femoral component as track record of this implant was unknown. THA is recommended treatment option in relatively active, independent individual and in those with the longest life expectancy [12]. On the other hand, hemiarthroplasty has a potential risk for deteriorating functional outcome, in these populations [12]. From a biomaterial perspective, the wear-through of the polyethylene liner eventually caused the head to articulate in direct contact with the outer metal dome and further activity of the femoral head leading to fatigue failure of the metal dome with a metal chip avulsion. We compared the polyethylene liner thickness and the bipolar metal dome thickness of the prosthesis used in this patient with a standard bipolar prosthesis (Depuy, Warsaw, Indiana). The polyethylene thickness in failed implant was equal to standard bipolar prosthesis however the outer metal dome thickness was less compared to standard bipolar prosthesis. This discrepancy in hardness is underscored which leads to fatigue fracture of metallic shell further by the fact that the femoral head revealed no obvious signs of wear. These findings corroborate the observation made by other reports [13, 14].
The contributing factors for present catastrophic failure include physiological young patient age leading to excessive and early wear; lack of appropriate follow-up causes delayed recognition of erosive polyethylene wear. Over time, the outer metallic dome lost its intended movement and assumed a fixed position. We assumed that this fixed position caused asymmetric load carriage affects with stress concentration effect at the center, compounded by repeated articulation of the compatible modular femoral head with the inner liner that leads to transmural wear-through of polyethylene and ultimately fatigue fracture of the outer metallic dome. Furthermore, inadequate thickness of outer metal-dome as suggested by biomechanical analysis also contributes significantly to this rare complication.
On the basis of our experience, we recommend that all patients who have undergone bipolar hemiarthroplasty even though they are asymptomatic should be followed closely for early diagnosis of erosive polyethylene induced fatigue failure of the outer metal dome of the monobloc shell of the bipolar prosthesis.
In light of the present case report, it might be prudent to search for the optimal prosthesis bearing surface and to reconsider the indications for bipolar hemiarthroplasty. The present report emphasis over routine follow-up as early recognition of erosive polyethylene wear will avoid unnecessary complete revision hip arthroplasty.
Fatigue fracture of the outer metal dome of monobloc sell of bipolar prosthesis is an unusual and exceptional complication following hemiarthroplasty hip. While risk factors have been discussed, exact mechanisms of failure are not well understood. It is imperative to have periodic radiographic monitoring for active patients who have undergone bipolar hemiarthroplasty, to identify and manage early complications, and avoid inevitable propagation of metal defect and catastrophic fatigue failure.
References
- 1.Swiontkowski MF. Intracapsular fractures of the hip. J Bone Joint Surg Am 1994;76:129-38. [Google Scholar]
- 2.Barmada R, Mess D. Bateman hemiarthroplasty component disassembly. A report of three cases of high-density polyethylene failure. Clin Orthop Relat Res 1987;224:147-9. [Google Scholar]
- 3.Calton TF, Fehring TK, Griffin WL, McCoy TH. Failure of the polyethylene after bipolar hemiarthroplasty of the hip. A report of five cases. J Bone Joint Surg Am 1998;80:420-3. [Google Scholar]
- 4.Herzenberg JE, Harrelson JM, Campbell DC, Lachiewicz PF. Fractures of the polyethylene bearing insert in Bateman bipolar hip prostheses. Clin Orthop Relat Res 1988;228:88-93. [Google Scholar]
- 5.Dai Z, Li Y, Jiang D. Meta-analysis comparing arthroplasty with internal fixation for displaced femoral neck fracture in the elderly. J Surg Res 2011;165:68-74. [Google Scholar]
- 6.Keating J, Grant A, Masson M, Scott N, Forbes J. Displaced intracapsular hip fractures in fit, older people: A randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty. Health Technol Assess 2005;9:1-65. [Google Scholar]
- 7.Bhandari M, Devereaux PJ, Tornetta P, Swiontkowski MF, Berry DJ, Haidukewych G, et al. Operative management of displaced femoral neck fractures in elderly patients: An international survey. J Bone Joint Surg Am 2005;87-A:2122-30. [Google Scholar]
- 8.Park KS, Chan CK, Lee DH, Yoon TR. Midterm Results of Conversion from failed bipolar hemiarthroplasty to total hip arthroplasty. Indian J Orthop 2018;52:369-73. [Google Scholar]
- 9.Messieh M, Mattingly DA, Turner RH, Scott R, Fox J, Slater J. Wear debris from bipolar femoral neck-cup impingement: Acause of femoral stem loosening. J Arthroplasty 1994;9:89-93. [Google Scholar]
- 10.Nakata K, Ohzono K, Masuhara K. Acetabular osteolysis and migration in bipolar arthroplasty of the hip: 5 to 13-yearfollow-up study. J Bone Joint Surg 1997;79B:258-64. [Google Scholar]
- 11.Kaku N, Tsumura H, Torisu T. Qualitative analysis of polyethylene wear in a bipolar femoral prosthesis: A case report. J Orthop Surg (Hong Kong) 2001;9:71-6. [Google Scholar]
- 12.Keating JF, Grant A, Masson M, Scott NW, Forbes JF. Randomized comparison of reduction and fixation, bipolar hemiarthroplasty, and total hip arthroplasty: Treatment of displaced intracapsular hip fractures in healthy older patients. J Bone Joint Surg Am 2006;88-A:249-60. [Google Scholar]
- 13.Maheshwari AV, Chawla A, Osuji OU, Malhotra R, Gulati YP. Fracture of the outer metallic head of the bipolar hip prosthesis: An unusual bearing surface failure. J Arthroplasty 2012;27:323.e9-12. [Google Scholar]
- 14.Legaye J. Rupture of the metallic lining in bicentric hemi-arthroplasties of the hip. Apropos of 3 cases. Acta Orthop Belg 1992;58:411-6. [Google Scholar]






