
Elderly patients with comorbidities, patella fracture and knee OA can be managed in a single sitting Total Knee Arthroplasty and does not require two stage management, thus avoiding complications associated with multiple surgeries and juxta-articular presence of hardware other than knee arthroplasty implants.
Dr. Srisanat Srinivasan Rao, Department of Joint Replacement and Reconstruction, Deenanath Mangeshkar Hospital and Research Center, Erandwane, Pune - 411 004, Maharashtra, India. E-mail: srisanat@gmail.com
Introduction:Total knee arthroplasty (TKA) is one of the most successful procedures for osteoarthritis (OA), but when associated with an old patella fracture, the knee arthroplasty becomes complex due to discontinuity in extensor mechanism. Moreover, in elderly patients, early mobilization and avoiding multiple surgeries are important to prevent associated morbidity. This is the first instance of a case series being reported where an untreated patella fracture >3-months-old with knee OA has been managed with single stage TKA.
Case Report:Two patients, both with OA of knee and untreated patellar fractures, presented to us with knee pain. A 74-year-old lady having 6-months-old untreated right patella fracture without extensor lag was our first patient and a 57-years-old lady having 2-years-old patella fracture non-union with extensor lag of 30° was our second patient. Both were assessed and a decision to perform total knee replacement was taken. Patient with extensor lag required reconstruction of the extensor mechanism whereas the one without extensor lag was treated as a normal routine total knee replacement.
Conclusion: Elderly patients with untreated patella fracture and degenerative knee OA can be considered for single stage TKA, with decision on patella management based on the presence or absence of extensor lag. Rehabilitation is faster with single surgery and also there are decreased risks and complications associated with multiple surgeries.
Keywords: Untreated patella fracture with knee OA, single stage TKA, TKA in extensor lag
Total knee arthroplasty (TKA) surgery for knee osteoarthritis (OA) is beneficial in the medium and long-term to improve quality of life resulting in better pain relief, patient satisfaction, and function [1]. However, OA of the knee associated with patella fracture is a complex scenario due to affection of extensor mechanism. We had two patients who presented to us with old untreated patella fracture with knee OA. This could have been treated in two ways: 1) Single stage TKA with simultaneous patella management and 2) two stage management involving fixation of patella in the first stage followed by TKA in the second stage after patellar union. However, the patient has to undergo two surgeries in the second scenario and this may increase the overall complications associated with anesthesia as well as multiple surgeries. Since, intact extensor mechanism is a prerequisite for TKA, patella fractures with knee OA have to be suitably managed. We decided to achieve it in a single surgery with two patients presenting to us.
Case 1
First patient was a 74-year-old female with both knee OA and 6-month-old untreated right patella fracture in fibrous union. She had comorbidity of hypertension and advanced age. She already had long standing OA of both knees when she sustained a closed right patella fracture following a domestic fall 6 months back. On evaluation, she was found to have a two-part patella fracture. Patient was advised surgery, but did not undergo surgery because of apprehension of hospitalization and undergoing surgery during COVID pandemic. Eventually, she was treated only with long knee brace and gradual weight bearing as per tolerance. She continued to have progressively increasing knee pain. She presented to us with bilateral knee OA with 20° knee varus without extensor lag or fixed flexion deformity. Patient could perform an active straight leg raise. Bilateral knee range of motion was 0–90°. Grade 4 OA in both the knees along with right patella two part transverse fracture was revealed on X-rays (Fig. 1). As the patient did not have any extension lag, we decided to do single-stage TKA without any intervention for patella fracture. Exposure was done through standard anterior midline incision and arthrotomy was medial parapatellar. As expected, extensor retinaculum was seen intact with fibrous tissue bridging the fractured fragments of patella. Routine TKA was performed. Patella was evaluated after final component placement, and patellar tracking was found satisfactory. Post-operative radiographs were satisfactory with patella in fibrous union (Fig. 1). In the early post-operative period, full weight bearing and up to 90° of knee flexion was allowed. She was also able to perform active straight leg raise (Fig. 2). At 3 months follow up, there was no extension lag and the patient could walk full weight bearing.
Case 2
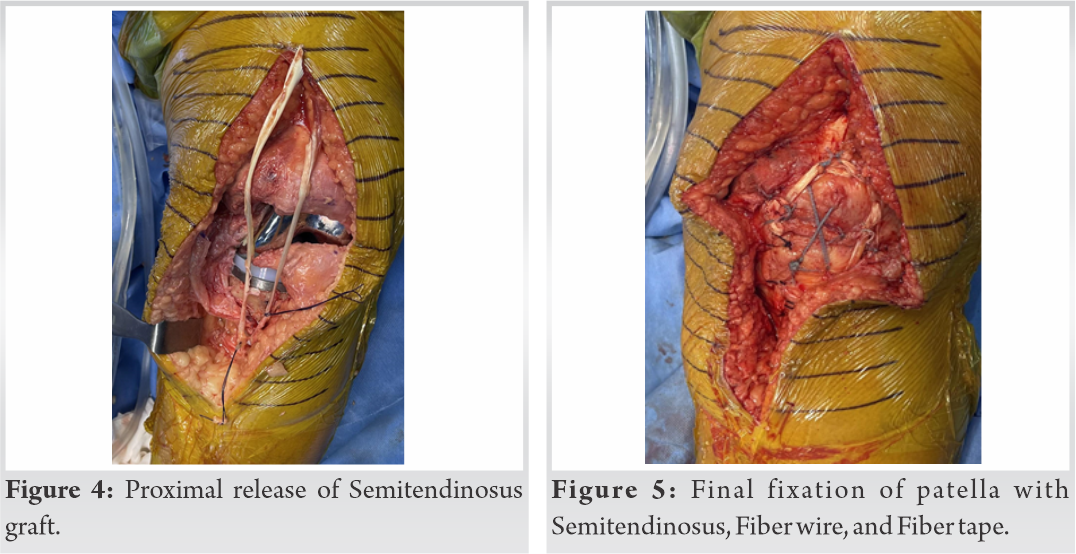
Second patient was a 57-year-old female with both knee OA and 2-years-old left patella fracture in non-union. She was hypertensive with morbid obesity (BMI-40.9). She already had long standing OA of both knees when she sustained a closed two part transverse left patella fracture following a domestic fall 2 years back. Patient was advised surgery, but the patient neglected it. Patient was bed ridden when she presented to us. On evaluation, the patient had bilateral knee OA, left more painful than right. Left knee had 30° of extensor lag with further flexion possible up to 90° with a varus of 20°. X-rays revealed grade 4 knee OA along with the left patella two part transverse fracture (Fig. 3). As the patient had extension lag, we decided to reconstruct the extensor mechanism during TKA surgery. Standard midline incision and medial parapatellar arthrotomy was performed. Patella fracture was exposed using transverse incision over extensor retinaculum. All the femoral and tibial cuts were performed as routine and trial implants were placed. Fibrous tissue at patella fracture site was excised, fracture edges were freshened and fracture reduced with help of towel clips. Two parallel drill holes were made superoinferiorly through patella to pass No.2 fiber tape in figure of eight fashion. Semitendinosus was identified near insertion and released proximally using open ended tendon stripper (Fig. 4). Semitendinosus tendon was passed around patella in a cerclage manner. This was reinforced with No.2 fiber wire. The lax extensor retinaculum was double breasted with No.2 fiber wire (Fig. 5). Patellar tracking was evaluated and found satisfactory. Final components were implanted. Post-operative X-rays were satisfactory (Fig. 3). Three days after left TKA, the patient underwent right TKA uneventfully. Protected weight bearing on an above knee cast applied to the left lower limb was allowed for the first 3 postoperative months. After 3 months, knee bending and weight bearing were started as per tolerance on the left side after X-ray evaluation. At 4 months follow-up, left knee range of motion was 10–70° and right was 0–110°.
Discussion
OA is a degenerative joint condition commonly affecting the weight bearing joints in the body including the knee and results in progressive deterioration of activities of daily living. About 10% of the population aging more than 50 years suffers from OA [2]. Being the largest sesamoid bone, the function of patella is to decrease the force required for knee extension by increasing the lever arm at the knee joint. About 1% of all the fractures in the body are patellar fractures [3]. According to Danish national registry data, patella fractures are more common in women. Low impact trauma especially in women accounted for approximately 75% of all patella fractures in elderly population [4, 5]. We had two patients who were above 50 years with both knee OA with neglected patella fractures. In general, the treatment of a patella fracture in a pre-existing osteoarthritic knee is fixation of patella fracture first followed by TKA at a later stage. Various surgical methods including stainless-steel cerclage wiring, tension band wiring and arthroscopy assisted fixation are available for fracture management [6]. Among these, the modified tension band wiring using AO principles, is the most widely used and accepted technique for patella fracture fixation. One study has reported use of fiber wire instead of stainless steel wire in comminuted patella fracture fixation which resulted in less incidence of irritation and hardware breakage. In addition, early rehabilitation could be allowed [7]. Symptomatic hardware is one of the most frequently reported complications after patella fracture fixation using metallic implants. The incidence reported in literature ranges from 10% to 60% necessitating implant removal at a later stage [8, 9, 10]. As compared to metal implants the reoperation rate for symptomatic implants was lesser for fixation using fiber wires [11]. On reviewing literature, we found only two cases of simultaneous patellar fracture fixation surgery and TKA [12, 13]. Surendran et al. [12] reported the case of an elderly diabetic patient with knee OA who sustained a fresh patellar fracture, and Patel et al. [13] described an elderly male with knee OA and 1-month-old patella fracture. In contrast to this, both our patients had >3-months-old untreated patella fractures. Considering the COVID pandemic, elderly age group and comorbidity, we decided to tackle both the patella fracture and knee OA in single sitting, thereby decreasing the risk associated with anesthesia, immobilization, and multiple surgical procedures. In the first patient, since the extensor retinaculum was intact and there was no extensor lag pre-op, decision was taken to leave the 2-part patella fracture as such. In the second patient, although the extensor retinaculum was intact, the patient had a significant pre op extensor lag of about 30°. Hence, a decision was taken to restore the extensor mechanism using fiber wire, fiber tape, and semitendinosus graft and avoid use of metal constructs.
In summary, the advantage of addressing patella fracture with fiber wire and fiber tape is avoidance of problems associated with hardware. Performing simultaneous TKA along with patella fracture fixation avoids multiple surgical events and associated complications especially in elderly patients. The outcome of both these patients suggests that, for patella fracture in an elderly patient with concomitant knee OA, single-stage suture fixation of the patella along with TKA can be performed if there is significant extensor lag.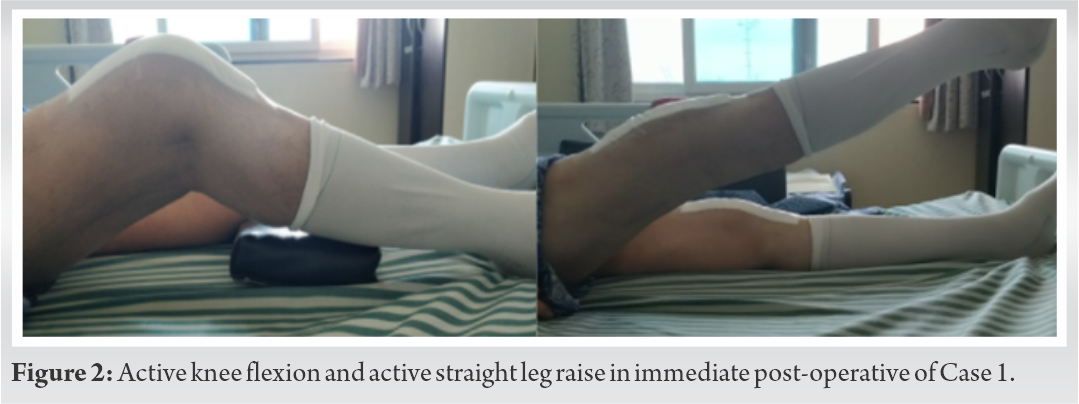
A limitation of patella fracture fixation with simultaneous TKA is that one cannot perform patella resurfacing in the presence of patellofemoral arthritis.
Two patients having knee OA and untreated patella fractures in COVID pandemic were operated for single stage total knee replacement with patella management in the same sitting. One patella was fixed with fiber wire, fiber tape, and semitendinosus graft. Another patella was left as such. The main aim of single stage TKA is to avoid multiple surgeries in elderly patients and avoid multiple hospital visits during COVID pandemic. This can help both arthroplasty and trauma surgeons to take informed decisions regarding patella fracture with knee OA.
This case series puts forth that elderly patients with comorbidities, patella fracture and knee OA can be managed in a single sitting and does not require two stage management. This avoids complications associated with multiple surgeries and juxta-articular presence of metallic hardware other than knee arthroplasty implants.
References
- 1.Canovas F, Dagneaux L. Quality of life after total knee arthroplasty. Orthop Traumatol Surg Res 2018;104:S41-6. [Google Scholar]
- 2.Lawrence RC, Helmick CG, Arnett FC, Deyo RA, Felson DT, Giannini EH, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum 1998;41:778-99. [Google Scholar]
- 3.Heusinkveld MH, den Hamer A, Traa WA, Oomen PJ, Maffulli N. Treatment of transverse patellar fractures: A comparison between metallic and non-metallic implants. Br Med Bull 2013;107:69-85. [Google Scholar]
- 4.Sim JA, Joo YB, Choi W, Byun SE, Na YG, Shon OJ, et al. Patellar fractures in elderly patients: A multicenter computed tomography-based analysis. Arch Orthop Trauma Surg 2021;141:1439-45. [Google Scholar]
- 5.Larsen P, Court-Brown CM, Vedel JO, Vistrup S, Elsoe R. Incidence and epidemiology of patellar fractures. Orthopedics 2016;39:e1154-8. [Google Scholar]
- 6.Lefaivre KA, O’Brien PJ, Broekhuyse HM, Guy P, Blachut PA. Modified tension band technique for patella fractures. Orthop Traumatol Surg Res 2010;96:579-82. [Google Scholar]
- 7.Lee BJ, Chon J, Yoon JY, Jung D. Modified tension band wiring using fibrewire for patellar fractures. Clin Orthop Surg 2019;11:244-8. [Google Scholar]
- 8.Hoshino CM, Tran W, Tiberi JV, Black MH, Li BH, Gold SM, et al. Complications following tension-band fixation of patellar fractures with cannulated screws compared with Kirschner wires. J Bone Joint Surg Am 2013;95:653-9. [Google Scholar]
- 9.LeBrun CT, Langford JR, Sagi HC. Functional outcomes after operatively treated patella fractures. J Orthop Trauma 2012;26:422-6. [Google Scholar]
- 10.Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183-7. [Google Scholar]
- 11.Shea GK, So KH, Tam KW, Yee DK, Fang C, Leung F. Comparing 3 different techniques of patella fracture fixation and their complications. Geriatr Orthop Surg Rehabil 2019;10:2151459319827143. [Google Scholar]
- 12.Surendran S, Pengatteeri YH, Park SE, Gopinathan P, Chang JD, Han CW. Osteoarthritis knee with patellar fracture in the elderly: Single-stage fixation and total knee arthroplasty. J Arthroplast 2007;22:1070-3. [Google Scholar]
- 13.Patel KH, Reddy AV, Eachempati K, Muralidhar S, Jungele A. A patient with osteoarthritis knee and prior patella fracture: Single stage fixation and total knee arthroplasty: A case report. J Orthop Case Rep 2018;8:67-70. [Google Scholar]






