
Luxatio Erecta Femoris needs anticipatory knowledge, timely intervention and proper reduction methods for better outcome.
Dr. A S Arun Kumar, Associate Professor, Department of Orthopaedics, Travancore Medical College Hospital, Thattamala, P.O.Kollam - 691 020, India. E-mail: arun.acme8.kottayam@gmail.com
Abstract
Introduction: Luxatio erecta femoris or inferior hip dislocation is the rarest type of hip dislocation. It can be caused by a severe trauma to the hip and the mechanism of injury is often very complex. Very few cases have been reported in the literature, and often associated with other musculoskeletal injuries. Overall about 3026 cases were reported till recently.
Case Presentations: We came across five cases of Luxatio erecta femoris from our six year study period from 2015 to 2020. All five cases were males (mean age-28.4 years, age range 20–40 years). All of them were isolated injuries (pure dislocation without any associated femur, acetabular, or pelvic fractures). We will present the details of these cases along with review of literature, trying to unravel the mechanism of such an injuries.
Conclusion: With the increase in high energy road traffic accidents, the incidence of luxatio erecta femoris in adults has increased. We could identify all those injuries and treated it with excellent clinical outcome. This type of rare dislocations if properly identified, we can manage it without much delay and very minimal complications.
Keywords: Luxatio erecta femoris, dislocation, trauma.
In our present scenario, there is a significant incidence of Road Traffic Accidents (RTA). These high energy traumas are associated with increased incidence of hip dislocations. Posterior hip dislocations are the most common type encountered, but inferior dislocations can also occur and it is the rarest type of all the dislocations encountered [1]. Luxatio erecta is the term commonly used to describe the inferior dislocation of shoulder and similarly in the hip region, the inferior dislocation is described as luxatio erecta of the hip or luxatio erecta femoris [2]. The mechanism of such an injury is very complex. Patient can rarely recollect exactly what had happened and also there might be other injuries too. There are very limited numbers of case reports in the literature and most of them are about pediatric hip dislocations and the mechanism of injury is entirely different from that of high energy trauma in an adult [3]. In our tertiary care center, we came across five such cases in a time frame of 6 years, from 2015 to 2020, all of them were isolated luxatio erecta femoris. In this study, we are discussing the details of these cases along with the essential review of literature.
Case 1
A 40 year old male sustained left hip injury following a RTA. He was the pillion rider on a motorcycle. A car hit the motorcycle and the pillion rider fell on his knee, the motorcycle and the rider fell on top of his back. He was brought to the emergency room (ER) with the lower limb flexed at the hip and knee, and thigh was supported with his own hands (Fig. 1). Any movements attempted were refused by the patient due to pain. Radiologically, the hip was found dislocated inferiorly. A few attempts were made under sedation in the ER to reduce it, but failed. So closed reduction under general anesthesia was done.
Case 2
A 28-year- old male brought to the emergency room ER with history of injury to left hip while engaged in a well digging work. He was crushed under the falling rubble from a well he was digging. He sustained blunt chest injury also. He was brought to the ER by co-workers with his lower limb flexed and supported by hands under the thigh. Clinically and radiologically diagnosed to have left inferior hip dislocation. So closed reduction under general anesthesia was performed.
Case 3
A 30-year- old male sustained a RTA while traveling in a car. He was driving the vehicle when hit by a pickup lorry from the front. Details of the injury mechanism were not available. On presentation to the hospital, the attitude of the right lower limb was flexion, abduction at the hip and flexion at knee joint. Associated head injury was managed non operatively. Radiographs of the hip showed typical inferior hip dislocation (Fig. 2), which was treated by closed reduction under general anesthesia.
Case 4
A 24-year-sold male was climbing a tree to trim its branches and leaves. One of the branches on which he stepped on broke off. Patient fell to the ground and landed on a flexed knee. He was brought to the ER with both hips and knees flexed. During examination one of the hips could be extended while the other was held tight by the patient. After doing clinical and radiological evaluation, patient was diagnosed with to have isolated inferior hip dislocation. Patient had a calcaneal fracture on the opposite limb as well which was treated conservatively. The hip was reduced under general anesthesia.
Case 5
A 20- year-sold female attempted suicide by jumping from about 50 ft height, brought to the emergency department with severe pain in the left hip, and deformity of left hip about 90o flexion, 15o abduction, and about 20o external rotation. No distal neurovascular impairment was there. She was having associated head injury and blunt trauma abdomen and chest. Radiologically diagnosed as inferior hip dislocation. After stabilizing her general condition, closed reduction of the dislocation under sedation was done.
Management Aand outcome. After stabilizing the general condition of patients in ER, computed tomography (CT) evaluation of hip was done to rule out any fractures. (Fig. 3). Closed reduction of hip under general anesthesia or intravenous sedation was done. Post- reduction review CT scan was done to rule out any intra-articular fragments or iatrogenic fractures. Skin traction for a period of 4 weeks was used in all the patients. Gradual supervised physiotherapy was initiated immediate post reduction period, for functional recovery in the follow- up period. All the cases were followed up for a period of 6 months. There was no pain, deformity, limitation of motion or features of avascular necrosis (AVN) in the radiographs, at the end of 6 months (Fig. 4a and 5b).
The hip joint is a ball-and-socket joint that’s inherently stable due to its bony architecture and powerful ligaments, allowing it to resist the abnormal destabilizing forces. The depth of the acetabulum, the labrum, joint capsule, muscular support, and surrounding ligaments contribute to the anatomical stability. The main ligaments stabilizing the joint from directional forces include the iliofemoral ligament and ischiofemoral ligament which are located anteriorly and the posteriorly, respectively (Fig. 5, 6). Dynamic muscular support includes the rectus femoris, gluteal muscles, and short external rotators [4]. Because the anterior ligaments are stronger, trauma to the hip commonly presents as a posterior dislocation (85%). Traumatic anterior dislocation accounts about 10% of dislocations [5]. Luxatio erecta femoris is a sub-type of anterior dislocation [6,7]. In the literature, it has been reported to occur generally following high-energy trauma and commonly seen with a concomitant femoral head or neck fracture. Isolated luxatio erecta is the rarest form [8,9].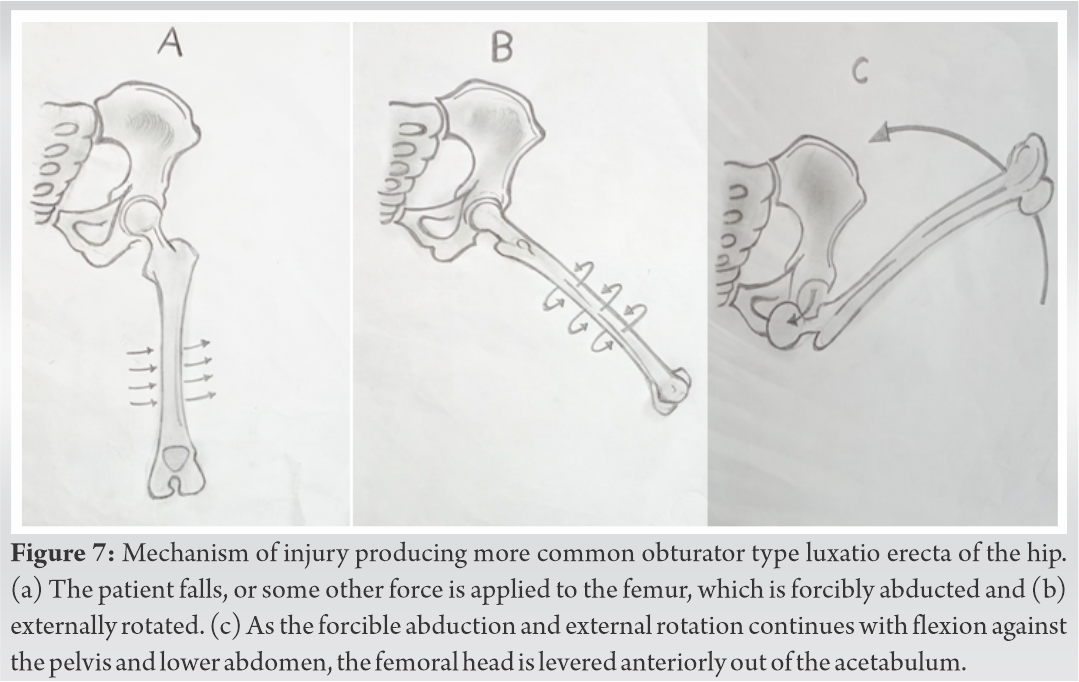
MEDLINE, PubMed, and Google Scholar were searched using the key words: “‘Hip”’ and “‘inferior dislocation”’ or “‘luxatio erecta femoris”’ or “‘infracotyloid dislocation’.” A total of 21 articles reporting on 24 men and 6 women aged 5– to 56 (mean, 25) years with 28 unilateral and one bilateral inferior dislocation of the hip were reviewed (Table 1) [2,3,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27]. Two patients had a concurrent displaced fracture of the ipsilateral proximal femur [18]. 1 One patient had an ipsilateral greater trochanter fracture post reduction which was managed surgically [22]. One patient had ipsilateral superior pubic rami fracture [23]. Six patients were children, [2,3,10,12,13], of whom 2 two were injured when another child fell onto their back as they fell [3,13]. Dislocation in children is usually secondary to low-energy trauma, owing to increased joint laxity and a shallow acetabulum [3]. The mechanism of injury included road traffic accidents (n = 13), falling while running (n = 4), sports related (n = 4), falling from a height (n = 5), falling from a bicycle (n = 1), and falling from a tree branch onto a leg (n = 1), and fall of wall over the body (n = 2). Most patients presented with an ischial-type dislocation, with extreme hip flexion, prominence of the greater trochanter, and the thigh touching the anterior abdominal wall, [10,11,12,13,14,3,15,16,19], whereas some presented with varying degrees of flexion, abduction, and external rotation, indicating an associated fracture, a chronic injury, or an obturator-type dislocation [17,18,20]. All dislocations were treated with closed reduction under sedation or general anaesthesia, followed by varying regimens of traction and restricted weight bearing. One patient with a chronic, neglected inferior dislocation of the hip underwent total hip arthroplasty and regained normal activity by 3 months [20]. One patient with a concurrent intertrochanteric proximal femoral fracture underwent open reduction (with the aid of a Schanz pin) and internal fixation (with a compression hip screw) [18]. One patient had a recurrent dislocation after a fall from a standing height one 1 year later. Two patients underwent operative treatment for shaft of femur fracture (inter locking nailing) [9,26] . All patients eventually achieved a full and pain-free range of hip motion, with no evidence of avascular necrosis of the femoral head. All children achieved normal hip development. Four patients were lost to follow- up [13,14,16,27,28]. A limitation of this study was that meta-analysis was not performed and that only case reports and case series were reviewed. 
The exact mechanism of injury is still debatable .The sequence of events resulting in the deformity are not always recollected as they are high energy injuries and the condition of the patient at the time of injury. When the hip dislocates inferiorly, it is flexed to an extent that the distal end of the femur rises above the horizontal plane of the pelvis at the acetabular fossae level. Two mechanisms of injury have been identified producing two different subtypes of inferior hip dislocation, that is, i.e. obturator subtype and ischial subtype [9]. The obturator dislocation has characteristic limb position and mechanism of injury. Kolar Kolar et al. suggested that extreme hip flexion coupled with lateral pressure might make head of the femur pushed through gap between ischiofemoral and pubofemoral ligaments with iliofemoral ligament acting as hinge [19] (Fig 7). Ischial subtype could result from a fall from height, leading to an axial load to the femur in a flexed position or from an injury that forces the hip into wide abduction, the femur inverted and the head lying below the acetabulum alongside and lateral to the ischial tuberosity [26] (Fig. 8). The obturator type is the most commonest type [19]. Patients usually complain of pain and keep the thigh flexed. The long axis of the femur may vary in alignment with respect to the spine from parallel to an angle almost 90° away from the axis. A variety of circumstances have been mentioned in the literature which lead to inferior hip dislocation — fall from height to curb or the pavement below, falling while running, a heavy object falls over the back of the falling victim, etc. [9]. In our case 2, the impact was upon a flexed knee with the hip also in flexion. The knee impacted on the well floor and was then fixed. The body was flexed on the hip and its weight and the momentum of the fall were transmitted to the shaft of the femur, which was fixed at the knee. The forward momentum of the body and the weight of well wall falling over the body added to the loading of the femur, which was dissipated by escape of the femoral head through the relatively rimless inferior margin of the acetabulum. The femoral head came to rest lateral to the ischium. 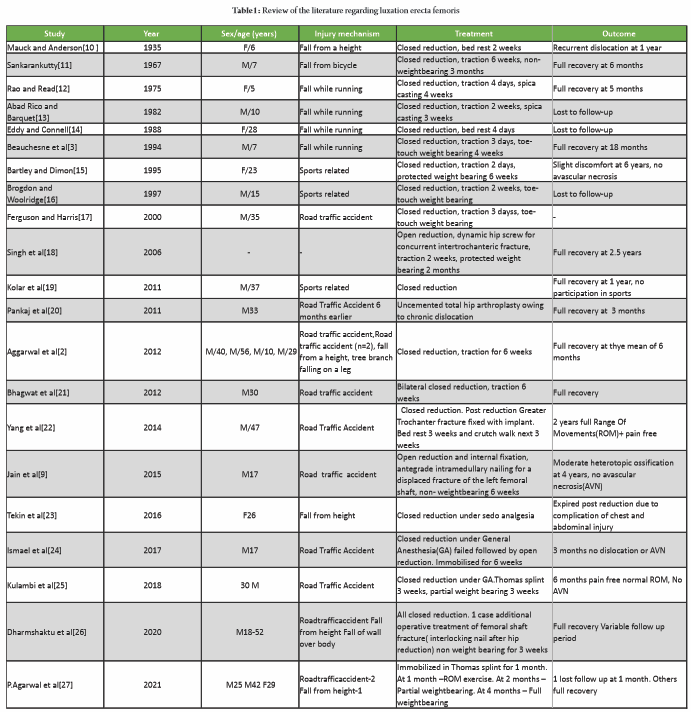 In the treatment of traumatic luxatio erecta femoris, closed reduction is recommended through muscle relaxation under general anaesthesia or sedation, but at times open reduction is the next option [26]. Reduction can be attained by maintaining traction toward the head end of patient while gradually extending the thigh, sometimes with additional internal rotation. [2,29]. The hip is usually immobilized for 4 weeks followed by partial weight bearing. The results of the dislocation in most studies have been found good with good range of motion and no features of avascular necrosis in most reports [30].
In the treatment of traumatic luxatio erecta femoris, closed reduction is recommended through muscle relaxation under general anaesthesia or sedation, but at times open reduction is the next option [26]. Reduction can be attained by maintaining traction toward the head end of patient while gradually extending the thigh, sometimes with additional internal rotation. [2,29]. The hip is usually immobilized for 4 weeks followed by partial weight bearing. The results of the dislocation in most studies have been found good with good range of motion and no features of avascular necrosis in most reports [30].
Luxatio erecta femoris is a rare injury and very few cases have been reported in the literature and a majority were in pediatric population. With the increase in high energy road traffic accidents, the incidence in adults has increased. Diagnosis is evident by the typical extremity position and by radiographs. Closed reduction by applying gentle extension and internal rotation with concurrent cephalad traction is usually possible under general anesthesia or intravenous sedation. The prognosis after reduction is excellent.
Luxatio erecta femoris, if properly identified and managed without delay, the clinical outcome will be excellent.
References
- 1.Abad Rico JI, Barquet A. Luxatio erecta of the hip: A case report and review of the literature. Arch Orthop Trauma Surg 1982;99:227-9. [Google Scholar | PubMed]
- 2.Aggarwal S, Kumar V, Bhagwat KR, Shashikanth VS, Ravikumar HS. Inferior dislocation of the hip: A case series and literature review. Chin J Traumatol 2012;15:317-20. [Google Scholar | PubMed]
- 3.Beauchesne R, Kruse R, Stanton RP. Inferior dislocation (luxatio erecta) of the hip. Orthopedics 1994;17:72-5. [Google Scholar | PubMed]
- 4.Dawson-Amoah K, Raszewski J, Duplantier N, Waddell BS. Dislocation of the hip: A review of types, causes, and treatment. Ochsner J 2018;18:242-52. [Google Scholar | PubMed]
- 5.Bastian JD, Turina M, Siebenrock KA, Keel MJ. Long-term outcome after traumatic anterior dislocation of the hip. Arch Orthop Trauma Surg 2011;131:1273-8. [Google Scholar | PubMed]
- 6.Chadha M, Agarwal A, Singh AP. Traumatic anterior dislocation of the hip joint with posterior acetabular wall fracture. Acta Orthop Belg 2005;71:111-4. [Google Scholar | PubMed]
- 7.Sultan A, Dar TA, Wani MI, Wani MM, Shafi S. Bilateral simultaneous anterior obturator dislocation of the hip by an unusual mechanism-a case report Ulus. Travma Acil Cerrahi Derg 2012;18:455-7. [Google Scholar | PubMed]
- 8.Reigstad A. Traumatic dislocation of the hip. J Trauma 1980;20:603-6. [Google Scholar | PubMed]
- 9.Jain S, Haughton BA, Grogan RJ. Inferior dislocation of the hip: A case report and literature review. J Orthop Surg (Hong Kong) 2015;23:123-6. [Google Scholar | PubMed]
- 10.Mauck HP, Anderson RL. Infracotyloid dislocation of the hip. J Bone Joint Surg 1935;17:1011-3. [Google Scholar | PubMed]
- 11.Sankarankutty M. Traumatic interior dislocation of the hip (luxatio erecta) in a child. J Bone Joint Surg Br 1967;49:145. [Google Scholar | PubMed]
- 12.Rao JP, Read RB. Luxatio erecta of the hip. An interesting case report. Clin Orthop Relat Res 1975;110:137-8. [Google Scholar | PubMed]
- 13.Abad Rico JI, Barquet A. Luxatio erecta of the hip. A case report and review of the literature. Arch Orthop Trauma Surg 1982;99:277-9. [Google Scholar | PubMed]
- 14.Eddy RJ, Connell DG. Luxatio erecta of the hip. AJR Am J Roentgenol 1988;151:412. [Google Scholar | PubMed]
- 15.Bartley RE, Dimon JH. Traumatic inferior hip dislocation in an adult (luxatio erecta). Orthopedics 1995;18:1173-4. [Google Scholar | PubMed]
- 16.Brogdon BG, Woolridge DA. Luxatio erecta of the hip: A critical retrospective. Skeletal Radiol 1997;26:548-52. [Google Scholar | PubMed]
- 17.Ferguson KL, Harris VV. Inferior hip dislocation in an adult: Does a rare injury now have a common mechanism? Am J Emerg Med 2000;18:117-8. [Google Scholar | PubMed]
- 18.Singh R, Sharma SC, Goel T. Traumatic inferior hip dislocation in an adult with ipsilateral trochanteric fracture. J Orthop Trauma 2006;20:220-2. [Google Scholar | PubMed]
- 19.Kolar MK, Joseph S, McLaren A. Luxatio erecta of the hip. J Bone Joint Surg Br 2011;93:273. [Google Scholar | PubMed]
- 20.Pankaj A, Sharma M, Kochar V, Naik VA. Neglected, locked, obturator type of inferior hip dislocation treated by total hip arthroplasty. Arch Orthop Trauma Surg 2011;131:443-6. [Google Scholar | PubMed]
- 21.Bhagwat KR, Garg B, Aggarwal S, Dhillon MS. Bilateral inferior dislocation of the hip-a case report. Chin J Traumatol 2012;15:121-3. [Google Scholar | PubMed]
- 22.Yang JH, Pandher DS, Oh KJ. Fracture of the greater trochanter during closed reduction of obturator type hip dislocation. Hip Pelvis 2014;26:275-8. [Google Scholar | PubMed]
- 23.Tekin AÇ, Çabuk H, Büyükkurt CD, Dedeoǧlu SS, İmren Y, Gürbüz H. Inferior hip dislocation after falling from height: A case report. Int J Surg Case Rep 2016;22:62-5. [Google Scholar | PubMed]
- 24.Ismael S, Vora J, Thomas P. Adult traumatic inferior hip dislocation: Rare case ended with open reduction. J Orthop Case Rep 2017;7:101-4. [Google Scholar | PubMed]
- 25.Kulambi V, Chaudhary K, Pethapara V. Anterior hip dislocation in young patient obturator (inferior) type: A rare case report. Int J Res Orthop 2018;4:523-6. [Google Scholar | PubMed]
- 26.Dharmshaktu GS, Adhikari N, Singh B. Luxatio erecta of the hip-a report of five cases and the literature review. J Orthop Dis Traumatol 2020;3:13-6. [Google Scholar | PubMed]
- 27.Agarwal P, Khadilkar S, Handralmath S, Khadilkar M. 74Anterior inferior hip dislocation: Report of three cases and review of literature. J Orthop Case Rep 2021;11:71-4. [Google Scholar | PubMed]
- 28.El Hajj Moussa M, Tawk C, Hoyek F, Lahoud JC. Traumatic inferior hip dislocation: A rare adult case with ipsilateral bifocal hip fracture. J Surg Case Rep 2016;4:1-3. [Google Scholar | PubMed]
- 29.Yang EC, Cornwall R. Initial treatment of traumatic hip dislocations in the adult Clin Orthop Relat Res 2000;377:24-31. [Google Scholar | PubMed]
- 30.Zeytin AT, Kaya S, Kaya FB, Ozcelik H. Traumatic inferior hip dislocation. J Med Sci (North America) 2015;6:238-9. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2020 A Rare Case of Bilateral Fracture Neck Femur Treated with Bilateral Distal Loading Stem Total Hip Arthroplasty, in a Single Sitting
August 10, 2020 A Rare Case of Bilateral Fracture Neck Femur Treated with Bilateral Distal Loading Stem Total Hip Arthroplasty, in a Single Sitting October 10, 2023 Trans sacral Endoscopic Laser Decompression – A Case Report, Technical Note and Literature review
October 10, 2023 Trans sacral Endoscopic Laser Decompression – A Case Report, Technical Note and Literature review January 10, 2023 Chondroblastoma of Metacarpal Masquerading as Enchondroma – A Case Report
January 10, 2023 Chondroblastoma of Metacarpal Masquerading as Enchondroma – A Case Report June 13, 2021 Gossypiboma and Total Hip Arthroplasty-A Rare Accidental Finding Following a Periprosthetic Infection
June 13, 2021 Gossypiboma and Total Hip Arthroplasty-A Rare Accidental Finding Following a Periprosthetic Infection