
We get to learn a fracture type which is more coronally oriented compared with a fracture line in typical spondylolysis, which is a new fracture type.
Dr. Clevio Desouza, Department of Orthopaedics, Dr. D.Y. Patil Medical College, Hospital and Research Centre, Pune. Maharashtra. India. E-mail: ceviod@gmail.com
Introduction: The leading cause of low back pain in our country like India in children and in adolescent has been found to be lumbar spondylolysis. This affects approximately 6–8% of adults in the general population which includes a large number of asymptomatic cases. The main cause in this disease is found to be that of fatigue features which are found in 10% of young adults during heavy labor work, sports, and athletic activities.
Case Report: A 25-year-old, left hand dominant, cricket player was referred to Dr. DY Patil Hospital and Research Centre, Pimpri, Pune with complaint of low back pain while playing cricket with no neurological symptoms. His symptoms started 6 months back to this visit and have worsened despite conservative treatment with medications and rehabilitation. No obvious line was seen on the X-rays, but a right non-isthmic spondylolysis was noted at L5 on computed tomography scan. Based on our imaging findings and clinical examination, we made a diagnosis of non-isthmic spondylolysis. As the patient desired an early return to activity, we did not aim for bone union and provided pain relieving treatment which included temporary wearing of soft brace. As a result his pain improved.
Conclusion:In our case, the fracture type is more coronally oriented compared with a fracture line in typical spondylolysis. Furthermore, lifting weights transmit a force from the upper limb to lower limbs, it is likely that high loading causes this type of fracture. From a view of biomechanics, reducing extension loading should be an effective means in the treatment of this type of fracture.
Keywords:Non-isthmic, Spondylolysis, Low back pain, Fracture.
The leading cause of low back pain in our country like India in children and in adolescent has been found to be lumbar spondylolysis. This affects approximately 6–8% of adults in the general population which includes a large number of asymptomatic cases [1]. The main cause in this disease is found to be that of fatigue features [2] which are found in 10% of young adults during heavy labor work, sports, and athletic activities [3]. Although this condition is typically detected as a defect in the pars inter-articularis, there have been several variations in the fracture line as in the literature [4, 5, 6].
In our article, we reported a new fracture type.
A 25-year-old, left hand dominant, cricket player was referred to our hospital Dr. D.Y. Patil Hospital and Research Centre, Pimpri, Pune with a complaint of low back pain while playing cricket with no neurological symptoms. His symptoms started 6 months back to this visit and have worsened despite conservative treatment with medications and rehabilitation.
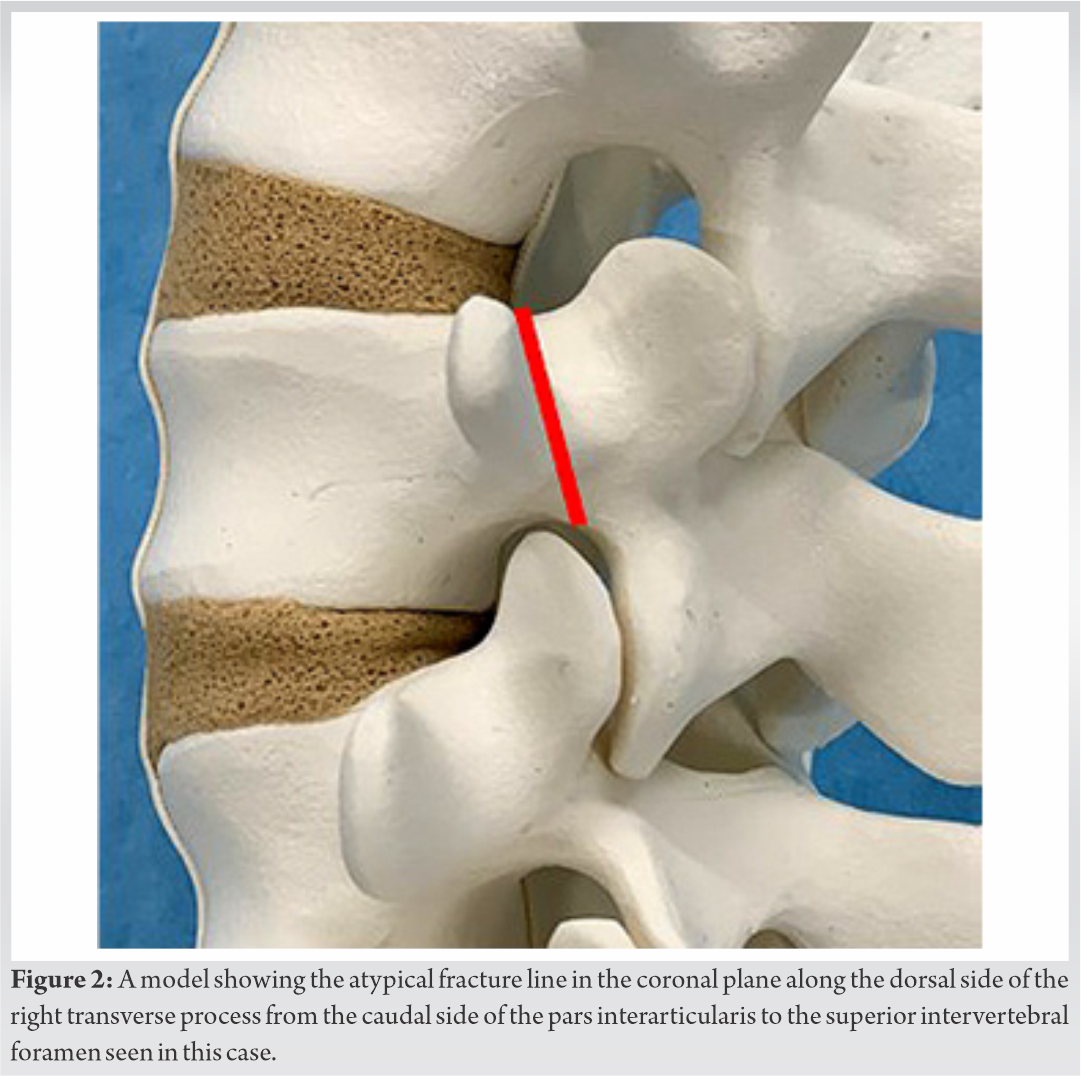
No obvious line was seen on the X-rays, but a right non-isthmic spondylolysis was noted at L5 on computed tomography scan (Fig. 1). A 3D reconstruction of the bone provided further classification, direction against right transverse process of the pars interarticularis from caudal side to superior intervertebral foramen (Fig. 2), short tau inversion recovery MRI showed an area of increased signal intensity in the superior articular process and the pedicle around the fracture line (Fig. 3). Based on our imaging findings and clinical examination, we made a diagnosis of non-isthmic spondylolysis. As the patient desired an early return to activity, we did not aim for bone union and provided pain relieving treatment which included temporary wearing of soft brace and analgesics with rest. As a result, his pain improved.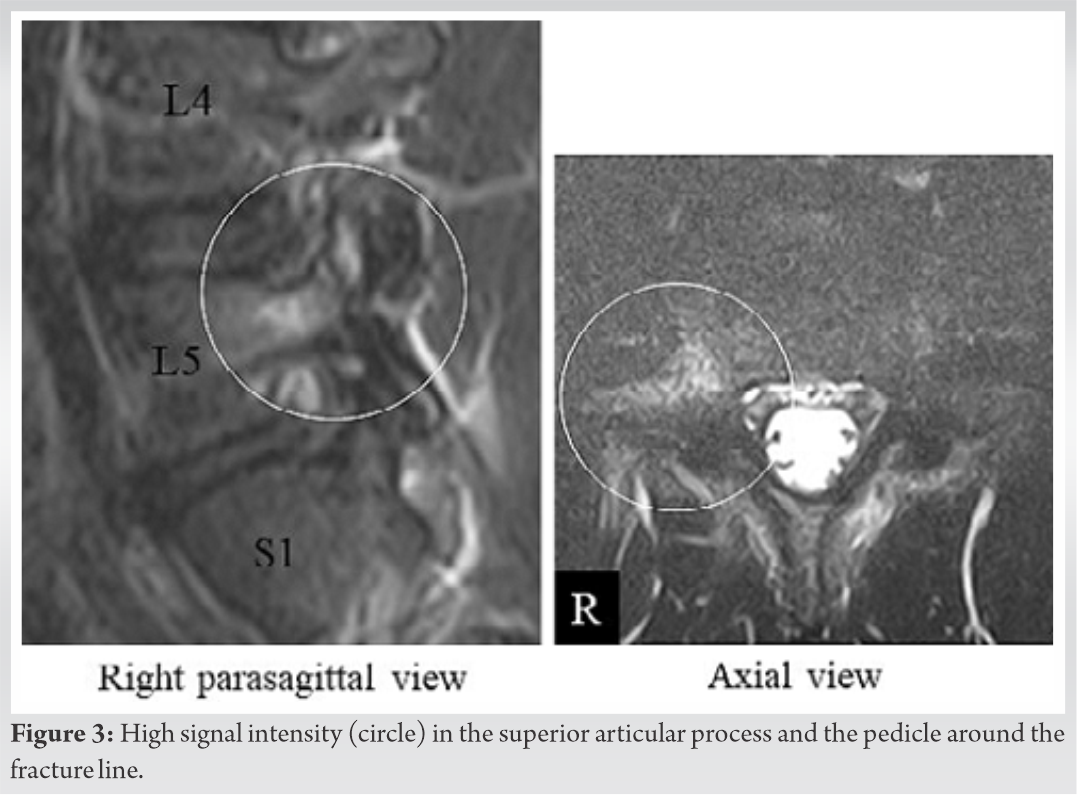
Six types of atypical imaging presentation have been previously reported as non-isthmic spondylolysis (Fig. 4). These may be classified into two main types: Pediculolysis in which the fracture line can be observed in the pedicle anterior to pars interarticularis and the second type is laminolysis which is seen in the lamina posterior to the pars interarticularis. However, the fracture type seen in the present case does not fall under these main types or any of the atypical presentations reported in the literature. Cases of laminolysis are considered to be congenital malformations and pediculolysis has been reported to occur after unilateral spondylolysis; however, the mechanism remains unknown.
The fracture in this case presented with a rare unilateral separation of spine on the side contralateral to the dominant side. Sairyo et al., in his study, demonstrated that maximum load is exerted on the pars interarticularis during lumbar extension with rotation and that extension loading causes a more coronally oriented fracture line as seen on images [7-10].
In our case, the fracture type is more coronally oriented compared with a fracture line in typical spondylolysis. Furthermore, lifting weights transmit a force from the upper limb to lower limbs, it is likely that high loading causes this type of fracture [9, 10]. Our patient received conservative treatment including rest, abstinence from work, and orthosis. From a view of biomechanics, reducing extension loading should be an effective means in the treatment of this type of fracture.
In our article, we reported a new fracture type. From a view of biomechanics, reducing extension loading should be an effective means in the treatment of this type of fracture.
References
- 1.Sakai T, Sairyo K, Takao S, Nishitani H, Yasui N. Incidence of lumbar spondylolysis in the general population in Japan based on multidetector computed tomography scans from two thousand subjects. Spine (Phila Pa 1976) 2009;34:2346-50. [Google Scholar]
- 2.Wiltse LL, Widell EH Jr., Jackson DW. Fatigue fracture: The basic lesion is inthmic spondylolisthesis. J Bone Joint Surg Am 1975;57:17-22. [Google Scholar]
- 3.Micheli LJ, Wood R. Back pain in young athletes. Significant differences from adults in causes and patterns. Arch Pediatr Adolesc Med 1995;149:15-8. [Google Scholar]
- 4.Viana SL, Viana MA, de Alencar EL. Atypical, unusual, and misleading imaging presentations of spondylolysis. Skeletal Radiol 2015;44:1253-62. [Google Scholar]
- 5.Nakayama T, Ehara S. Spondylolytic spondylolisthesis: Various imaging features and natural courses. Jpn J Radiol 2015;33:3-12. [Google Scholar]
- 6.Miyagi R, Sairyo K, Sakai T, Yoshioka H, Yasui N, Dezawa A. Two types of laminolysis in adolescent athletes. J Orthop Traumatol 2012;13:225-8. [Google Scholar]
- 7.Sairyo K, Katoh S, Sasa T, Yasui N, Goel VK, Vadapalli S, et al. Athletes with unilateral spondylolysis are at risk of stress fracture at the contralateral pedicle and pars interarticularis: A clinical and biomechanical study. Am J Sports Med 2005;33:583-90. [Google Scholar]
- 8.Sairyo K, Katoh S, Komatsubara S, et al. Spondylolysis fracture angle in children and adolescents on CT indicates the facture producing force vector: A biomechanical rationale. Internet J Spine Surg 2004;1:???. [Google Scholar]
- 9.Oshikawa T, Morimoto Y, Kaneoka K. Unilateral rotation in baseball fielder causes low back pain contralateral to the hitting side. J Med Invest 2018;65:56-9. [Google Scholar]
- 10.Conte SA, Thompson MM, Marks MA, Dines JS. Abdominal muscle strains in professional baseball: 1991-2010. Am J Sports Med 2012;40:650-6. [Google Scholar]





