
This is an alternative method not previously described in the literature that can be used in managing isolated distal distal radioulnar joint dislocations.
Dr. Sachith Sreenivasan, Department of Orthopaedics, Furness General Hospital, Barrow-in-Furness, United Kingdom. E-mail: sachithsreenivasan@hotmail.co.uk
Introduction: Isolated distal radioulnar joint dislocations are rare and commonly missed on radiographs. Knowledge of the management of these injuries, therefore, has room for improvement. We present a case with an alternative method of closed reduction.
Case Presentation:A young Caucasian male presented with severe pain and deformity of the left wrist, following a collision while playing rugby. This was easily diagnosed using plain radiographs and the initial attempted reduction methods in the Emergency Department failed. The patient was subsequently anesthetized in theatre, yet reduction by an accepted method of palmar to dorsal pressure over the interosseous membrane with simultaneous distraction of the wrist failed. A further attempt to manipulate the dislocated ulnar head was successful, with the same force applied, while the wrist was maximally flexed and pronated – thereby avoiding an open reduction.
Conclusion:This technique has not previously been described in the literature and may be used in similar injuries in the future.
Keywords:Orthopedics, trauma, distal radioulnar joint, dislocation, volar, reduction, closed.
Dislocations of the distal radioulnar joint are common and usually occur with a fracture. Isolated dislocations are less well documented [1, 2]. Volar distal radioulnar joint (DRUJ) dislocations in isolation are rare, with only 36 cases reported by 2019 [3, 4]. In our case, we have a young adult who suffered an isolated volar dislocation with no fracture. From a literature review, we have will discuss that various blockades to closed reduction and with our case have established a previously unreported blockade, subsequently describing a modification to previous reduction techniques.
A 26-year-old male presented to the Emergency Department with a left wrist deformation, after being tackled in a game of rugby, with his arm held against his body. He had pain at rest and movement, and a reduced range of movement generally. The vascularity of the limb was intact and the only neurological abnormality was a mildly reduced sensation to the ring and middle fingers on light touch, with no paresthesia.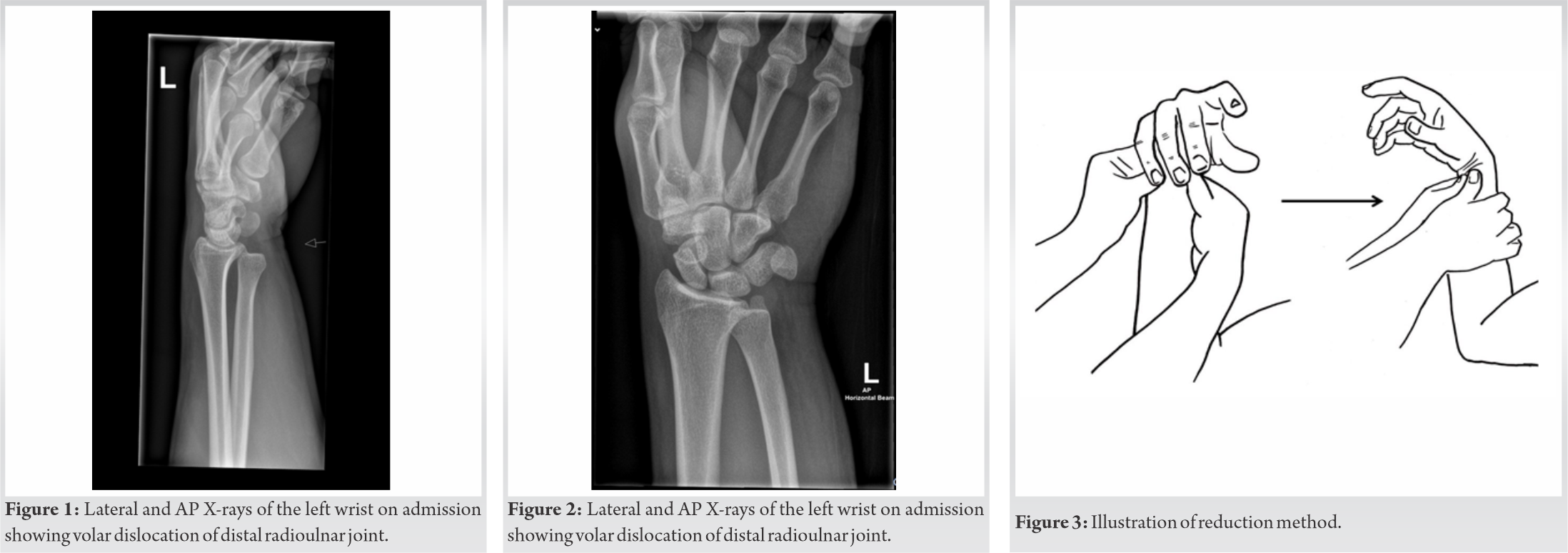 The patient was able to flex and extend the fingers with pain. There was no elbow tenderness on palpation; however, there was tenderness around the ulnar region of the wrist. PA and lateral X-rays Figures 1 and 2 of the left wrist showed a malalignment of the distal radioulnar joint, with the ulnar head appearing volarly displaced, indicating disruption of the DRUJ with no acute fracture. Attempted manipulation in the Emergency Department was unsuccessful as shown on repeat XR. The patient was put in an above elbow back slab and sling to be admitted for manipulation under anesthetic the next morning.
The patient was able to flex and extend the fingers with pain. There was no elbow tenderness on palpation; however, there was tenderness around the ulnar region of the wrist. PA and lateral X-rays Figures 1 and 2 of the left wrist showed a malalignment of the distal radioulnar joint, with the ulnar head appearing volarly displaced, indicating disruption of the DRUJ with no acute fracture. Attempted manipulation in the Emergency Department was unsuccessful as shown on repeat XR. The patient was put in an above elbow back slab and sling to be admitted for manipulation under anesthetic the next morning.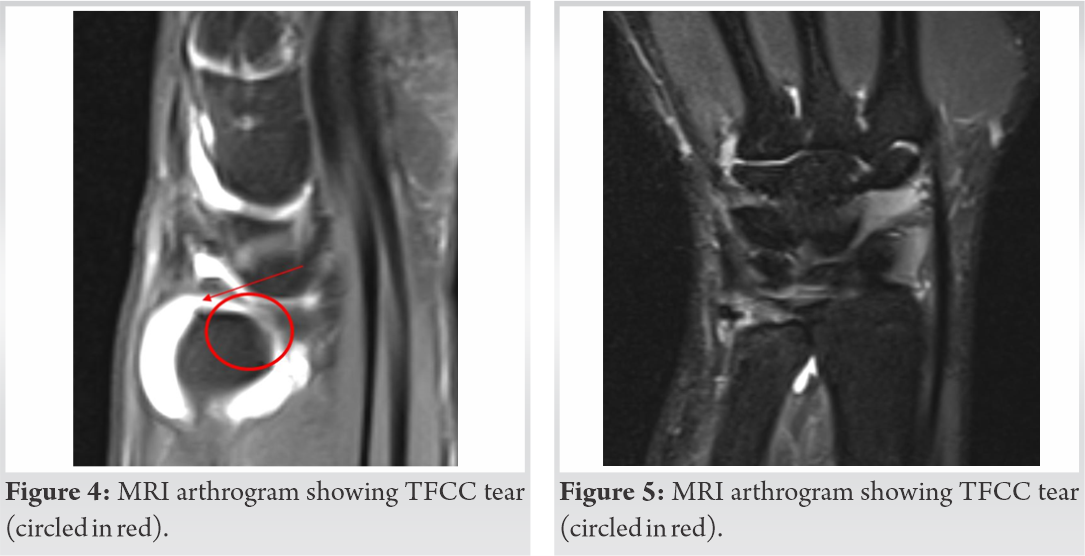
Left distal radioulnar joint dislocation (Volar).
Procedure
Closed manipulative reduction was attempted under general anesthetic (GA) with traction, with the forearm in a pronated position. Due to suspected buttonholing of the distal ulna through the volar soft tissue, the initial attempt failed. A further gentle manipulation with the wrist in flexion was attempted to clear the soft tissue, and this resulted in complete reduction Figure 3. Post-reduction, the DRUJ was stable in supination and pronation. Elbow was examined clinically and under image, and Essex-Lopresti injury was ruled out. The limb was immobilized in a long arm back slab at 90° of flexion at the elbow, in the mid prone (neutral) position. The immobilization was removed at 4 weeks post-reduction and the patient was given a futura splint support, with advice to start gentle ROM. An MRI was organized to assess for internal derangement, which showed a central tear of the triangular fibrocartilage complex (TFCC) Figures 4 and 5. The patient was completely asymptomatic at final follow-up with full range of motion. Repeat radiographs demonstrated satisfactory position of the ulna Figures 6 and 7.
The DRUJ is a uniaxial articulation between the ulnar notch of the radius and the ulnar head, allowing only one degree of motion – pronation and supination. The triangular fibrocartilage, the ulnocarpal ligaments, and the sheath of the extensor carpi ulnaris keep the distal radioulnar joint congruent. In addition to attachments at the base of the ulnar styloid, they are collectively known as the TFCC [5]. There are multiple other independent contributors to the stability of the joint and the pronosupination arc. These are the joint capsule, the dorsal and palmar radioulnar ligaments, the interosseous membrane, and the muscles – extensor carpi ulnaris and pronator quadratus. The DRUJ joint capsule is a separate entity to the TFCC [5, 6], and the most important stabilizer is the TFCC [7]. Injury to these, therefore, makes the distal radioulnar joint susceptible to instability.
The DRUJ capsule is a continuous tripartite structure that blends with the volar and distal radioulnar ligaments. The volar and dorsal DRUJ capsule components are clinically different. There is a significant relationship between supination and the volar capsule. The volar leaf accepts the distal ulna during rotation and is thin and “folded as drapery in its midsection in an oblique orientation” [8].
A tear to the TFCC, or a rupture to the proximal interosseous membrane is almost required to produce a volar dislocation of the DRUJ, as found by Watanabe et al. using cadaveric studies [9]. Hagert has described that the dorsal radioulnar ligament and volar joint capsule are disrupted in a volar dislocation [10].
As noted by Larrivée et al., there are usual causal mechanisms of a volar DRUJ dislocation, such as a fall on outstretched hand, direct blow to the wrist or hypersupination of the forearm [3, 11]. In our patient’s case, the mechanism was a direct blow to the wrist. Often with volar DRUJ dislocations, the diagnosis is initially missed [12]. However, the early diagnosis prompted a higher likelihood of a closed reduction [1].
Diagnosing a DRUJ dislocation, as stated above, can be missed initially in up to 50% of cases and appropriate radiographic technique is vital, as is a high index of suspicion and satisfactory clinical information [13]. Sufficient imaging to make a diagnosis may be standard posteroanterior and true lateral X-rays, [12] as seen in our case. However, axial CT scans would be recommended to avoid missing ulnar impaction fractures [1]. The early treatment is critical to avoid chronic DRUJ disorders [12], and there are various options for management in the literature. These depend on any associated injuries; however, simple dislocation cases can be reduced with palmar to dorsal pressure on the distal part of the ulna [5, 14], combined with forceful pronation [5] or with distraction of the wrist [14]. There are multiple reported causes for irreducibility, namely, a displaced extensor carpi ulnaris tendon, or spasm of the pronator quadratus, which required full muscle relaxation under GA to reduce with distraction of the DRUJ, direct pressure on the ulnar head, and passive pronation [7]. Other blocks include interposition of the torn TFCC [3, 11] or impaction of the ulnar head, which generally requires open reduction; although a closed reduction technique modification was described involving pressure over the IOM [3]. A case of ulna impaction that required open reduction noted that on exploration the ulna head had ruptured through the volar capsule [15]. We are therefore potentially describing a previously unreported blockade to reduction, in that the ulna could have button holed through the volar capsule, requiring a modified technique to current methods to avoid open reduction.
In our case, the traction applied to aid reduction failing under GA indicated the pronator quadratus was less likely to be the blockade. Applying digital pressure and pronation with pressure in the IOM space are documented; however, the flexion of the wrist using gravity simultaneously does not appear to have been reported as a modification in reduction technique. The success of this method would indicate more likely the ulna that was buttonholing through the volar capsule. The advantage of using this simple method would prevent an open reduction and the risks that come with it.
1. Isolated volar DRUJ dislocations may occur with wrist injury caused by blunt trauma
2. There are multiple different blockades to closed reduction. The complex anatomy in the area should be noted due to the possibility of a buttonhole or physical block
3. Regardless of the blockade, a new method of closed reduction proposed is to attempt manipulation while allowing the wrist to flex, as opposed to distracting.
References
- 1.Mulford JS, Jansen S, Axelrod TS. Isolated volar distal radioulnar joint dislocation. J Trauma 2010;68:E23-5. [Google Scholar]
- 2.Garrigues GE, Aldridge JM. Acute irreducible distal radioulnar joint dislocation. J Bone Joint Surg 2007;89:1594-7. [Google Scholar]
- 3.Larrivée S, Matthewson G, Barron L. Closed reduction of an acute volar dislocation of the distal radio-ulnar joint by a modified technique. Case Rep Orthop 2018;2018:1-5. [Google Scholar]
- 4.Starnoni M, Colzani G, Santis GD, Acciaro AL. Management of locked volar radio-ulnar joint dislocation. Plast Reconstruct Surg Global Open 2019;7:e2480. [Google Scholar]
- 5.Szabo RM. Distal radioulnar joint instability. J Bone Joint Surg Am 2006;88:884-94. [Google Scholar]
- 6.Kleinman WB, Graham TJ. The distal radioulnar joint capsule: Clinical anatomy and role in posttraumatic limitation of forearm rotation. J Hand Surg 1998;23:588-99. [Google Scholar]
- 7.Bouri F, Fuad M, Abdolenour AE. Locked volar distal radioulnar joint dislocation. Int J Surg Case Rep 2016;22:12-4. [Google Scholar]
- 8.Gelberman R. The Wrist. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2009c. p. 418-9. [Google Scholar]
- 9.Watanabe H, Berger RA, Berglund LJ, Zobitz ME, An KN. Contribution of the interosseous membrane to distal radioulnar joint constraint. J Hand Surg 2005;30:1164-71. [Google Scholar]
- 10.Hagert CG. Distal radius fracture and the distal radioulnar joint--anatomical considerations. Handchir Mikrochir Plast Chir 1994;26 22-6. [Google Scholar]
- 11.Paley D, Rubenstein J, McMurtry RY. Irreducible dislocation of distal radial ulnar joint. Orthop Rev 1986;15:228-31. [Google Scholar]
- 12.Kumar A, Iqbal M. Missed isolated volar dislocation of distal radio-ulnar joint: A case report. J Emerg Med 1999;17:873-5. [Google Scholar]
- 13.Duryea DM, Payatakes AH, Mosher TJ. Subtle radiographic findings of acute, isolated distal radioulnar joint dislocation. Skeletal Radiol 2016;45:1243-7. [Google Scholar]
- 14.Rainey RK, Pfautsch ML. Traumatic volar dislocation of the distal radioulnar joint. Orthopedics 1985;8:896-900. [Google Scholar]
- 15.Tang CY, Cheung JP, Fung B. A rare combination: Locked volar distal radio-ulnar joint dislocation with isolated volar capsule rupture. Hand Surg 2014;19:413-7. [Google Scholar]





