
Open reduction and fixation with non-absorbable braided polyester sutures augmented with circumferential wiring are effective in the management of severely comminuted patella fractures and multi-fragmentary lower pole patella fractures, both of which are not amenable to the traditional techniques such as tension band wiring and screw fixation.
Dr. Shrihari L Kulkarni, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Shri Dharmasthala Manjunatheshwara University, Dharwad - 580 009, Karnataka, India. E-mail: shrihari1711@gmail.com
Introduction:Patella fractures account for about 1% of all musculoskeletal injuries. Modified tension band wiring (TBW) is the most commonly used technique for the management of patella fractures. However, all patella fractures are not-amenable to TBW. In this series, we present nine cases managed with open reduction and internal fixation using non-absorbable braided polyester suture (Ethicon Ethibond Excel 5-0) with circumferential stainless-steel wiring.
Case Series: This series included nine patients with fractured patella and managed with open reduction and internal fixation with non-absorbable sutures and circumferential wiring. Patient demographics, fracture type, time to union, functional outcome, and complications were recorded. Patients were followed up for minimum of 6 months (11.6 ± 3.7 months). All fractures went on to unite with average fracture healing time of 13.8 weeks. Mean Lyshom and Bostman score were 83 and 25.6, respectively. Seven patients had excellent to good outcome. One each had fair and poor outcomes. One patient developed superficial infection and knee stiffness.
Conclusion:Open reduction and fixation with non-absorbable sutures augmented with circumferential wiring are an efficient method for the management of severely comminuted and multi-fragmentary lower pole patella fractures with minimum complications.
Keywords:Patella fracture, non-absorbable sutures, Lyshom score, Bostman score.
Patella fractures account for about 1% of all musculoskeletal injuries and the age group of 20–50 years being most commonly affected. About 70–80% of them are the transverse fractures and 20–25% are comminuted. Inferior pole involvement is observed in about 5% of patella fractures [1]. Non-surgical or conservative management is reserved for fractures with intact extensor mechanism and minimal intra-articular step or displacement (<2 mm). Displaced patella fractures are managed surgically, modified tension band wiring (TBW) using longitudinal K-wires, and 18-gauge stainless steel wire being the gold standard procedure [2, 3]. However, all patellar fractures cannot be effectively managed with TBW. Multi-fragmentary lower pole fractures and severely comminuted fractures due to high energy trauma are always challenging to manage for every orthopedic surgeon as it is difficult to attain anatomical reduction of the patellar articular surface as the K-wires fail to hold the smaller fragments and fix them rigidly resulting in poor functional outcomes [4]. Sometimes, these fractures would require partial patellectomy with advancement and repair of patellar tendon, which impacts the extensor mechanism of the knee joint. Thus, preservation of as much bone stock as possible should always be the priority. In this series, we present nine such patients who were managed with open reduction and fixation using non-absorbable braided polyester sutures (Ethicon Ethibond Excel 5-0) with circumferential wiring.
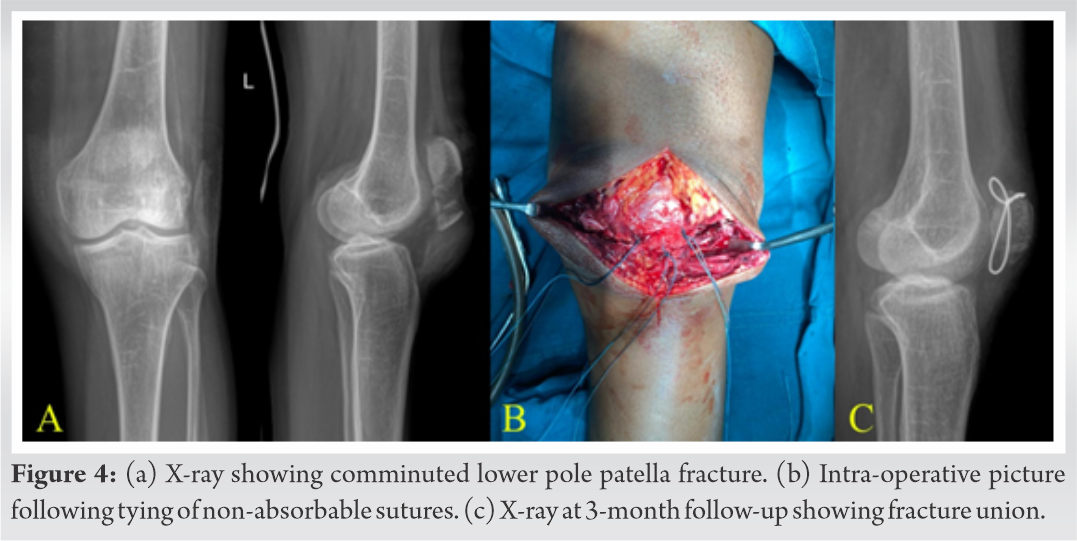
This case series included nine patients (six males and three females) with patella fracture which were managed by open reduction and fixation using non-absorbable sutures with circumferential wiring after taking informed consent (Table 1). Patient demographics, fracture type, time to union, functional outcome, and complications were recorded. Five patients presented following road traffic accident and four of them had fallen on knee. Three patients presented with comminuted lower pole fracture and others had severely comminuted displaced fracture. The management of these fractures was challenging and as it was difficult to get anatomical reduction and fixation with modified TBW was improbable (Fig. 1b, 2a, 3b, 4a).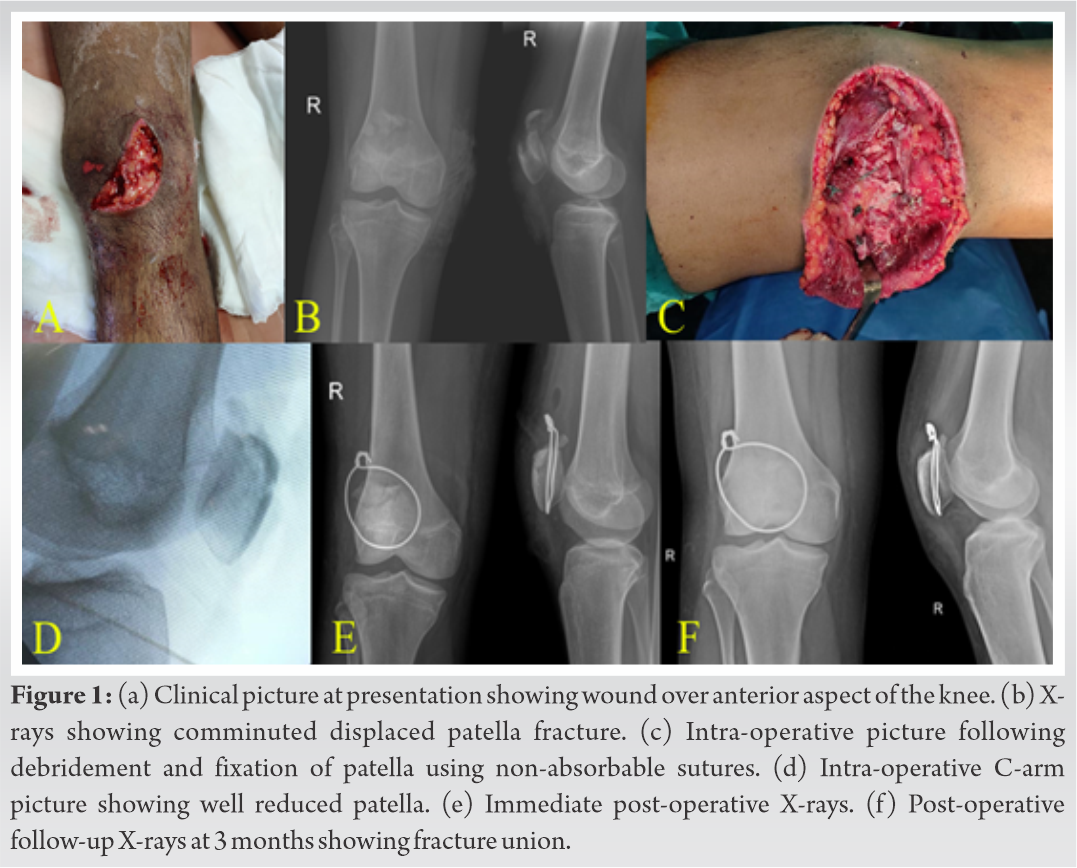
Operative procedure
All patients were operated under spinal anesthesia with pneumatic torniquet in situ. In patients with open fractures (three), thorough wound debridement and joint lavage were performed. A midline incision over the knee joint was taken in all patients. Fracture site was visualized and hematoma was let out. With the meticulous handling of the soft tissue, the fracture ends were cleaned of blood clots. Care was taken to not to detach the smaller fragments attached to the major fragments with some soft tissue. Knee joint was inspected for intra-articular loose fragments. Keeping intact as much bone stock as possible, with knee extension, major fragments were reduced temporarily and reduction was checked in the C-arm. The underside of the patella was palpated to ensure the reduction of the articular surface and to rule out the presence of any loose osteochondral fragments.
Using 1.8 mm K-wire pilot holes were done in both proximal and distal major fracture fragments through the fracture site, dividing patella into four equal parts. Non-absorbable braided polyester sutures were passed through the three tunnels made by the K-wire proximally and distally in the major fragments of the patella using a straight needle (Fig. 2b, 3c). All three sutures were tied one by one with the reduction held by an assistant. Care was taken while tying the knots not to apply excessive pressure which would result in the sutures cutting through the fragile cancellous bone (Fig. 1c, 2c, 3c, and 4b). The fixation was then augmented with circumferential wiring using 18-gauge stainless steel wire. This step was found to be especially important in the presence of small loose fragments even after suturing of the fracture fragments with non-absorbable sutures. The circumferential wire was passed transversely through the quadriceps tendon just above the superior pole of patella, taken around medial border of the patella, then taken through the mass of patellar tendon just adjacent to the inferior pole of patella, then taken along the lateral border to be tightened, and buried over the superolateral pole of the patella. Care was taken to pass the wire as close to the bone for better hold on the patella. Reduction and fixation were confirmed with intra-operative C-arm images (Fig. 1d and 3e). Retinacular tears were repaired using Vicryl 1-0. Tourniquet was released and hemostasis was achieved.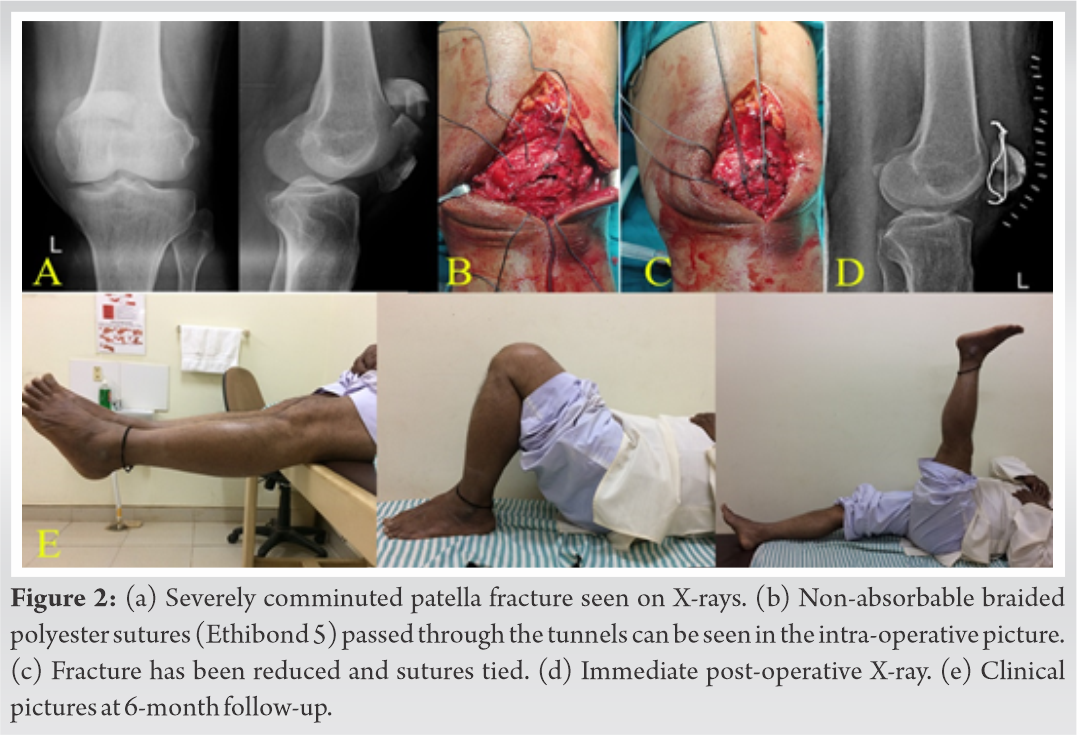
Post-operative protocol
Quadriceps strengthening exercises were stared from day 1. Drain was removed on day 3 and sutures were removed at post-operative day 10. All patients were immobilized with above knee slab for 3 weeks. At 3 weeks, knee was mobilized with range of movements (ROM) exercises and partial weight bearing mobilization with walker support was started. Full weight bearing mobilization was started at 6 weeks. All patients were followed up regularly with clinical and radiological assessment for minimum of 6 months. Fracture union and ROM were assessed. Lyshom and Bostman scoring were used for assessment of functional outcome.
Results
Patients were followed up regularly in our out-patient department for 6–18 months (11.6 ± 3.7 months). All fractures went on to unite well in 12–16 weeks (13.8 ± 1.39 weeks). One patient with Type II open comminuted lower pole fracture developed superficial infection, anterior knee pain, and knee stiffness (ROM: 10–90°). Another patient with the lower pole fracture developed anterior knee pain. The average range of knee flexion was 110° (range 90–130°). Lyshom score ranged from 54 to 96 (83 ± 13.1) and Bostman score ranged from 20 to 29 (25.6 ± 2.6). Seven patients had excellent to good outcome, one patient had fair and poor outcome each.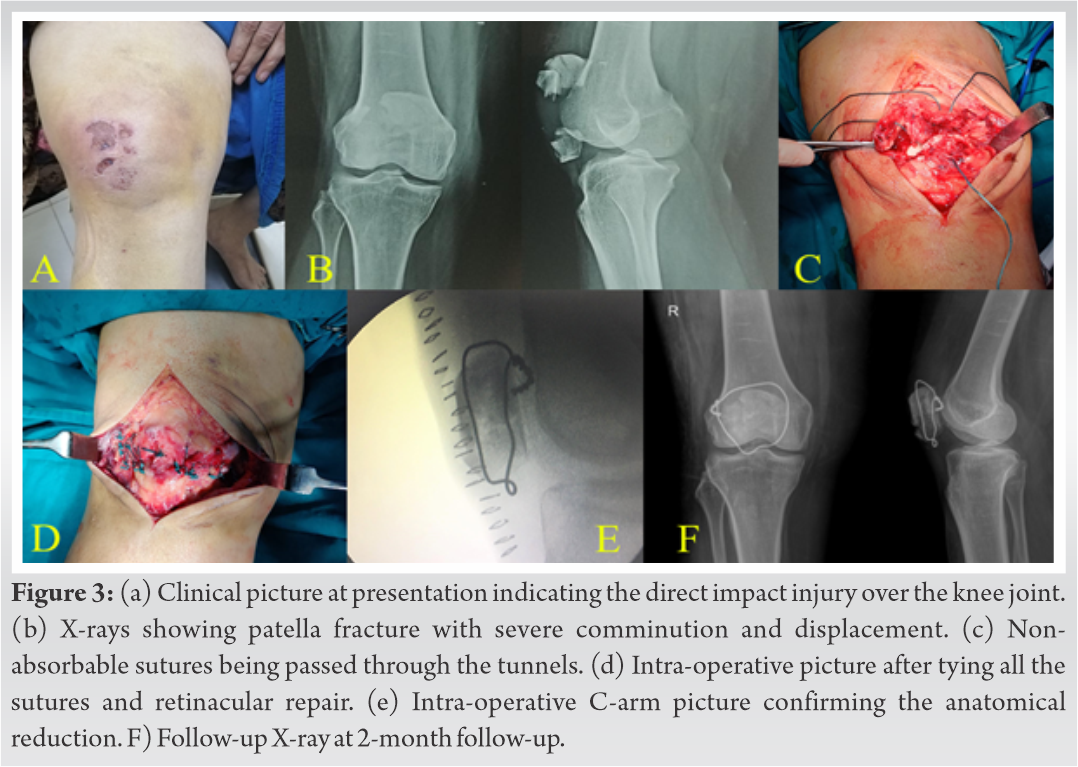
Patella is the largest sesamoid bone in the body embedded in the quadriceps tendon. Patella fractures can lead to severe restriction of the knee movements and in turn affects the knee function as it plays very important role in the extensor mechanism and biomechanical function of the knee. Primarily acts as an anatomical pulley for the quadriceps muscle. Biomechanically, it increases the effective lever arm of the quadriceps in effective knee extension or resistance of knee flexion, thus, improving the efficiency of the quadriceps muscle [5].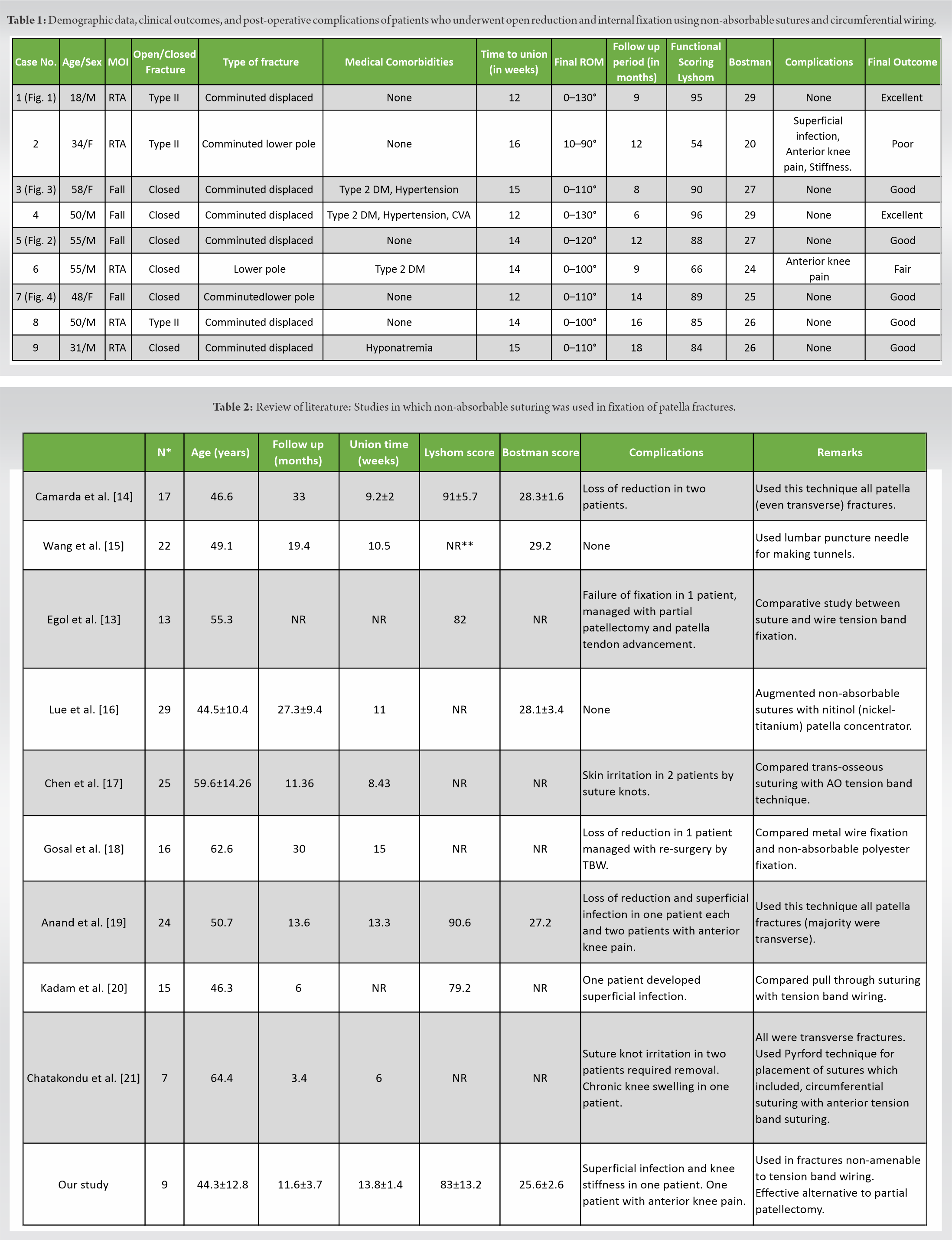
Basket plating, separate vertical wiring, wiring through cannulated screws, TBW, and partial patellectomy are various surgical procedures used for fixation of patella fractures. Modified TBW has been the gold standard procedure but multi-fragmentary lower pole fractures and severe comminuted fractures pose a challenge in fixation. The challenges are three-fold. First, it is not possible to hold all the fragments with K-wires. Second, as the stainless-steel wire is tightened, the K-wire holding the fragile comminuted distal fragments tends to either bend or cut through the bone resulting in an unusually palpable implant postoperatively. Third, poor bone purchase results in early backing-out of the K-wires from the stainless-steel loop resulting in loss of fixation. For the above reasons, the surgeon is always wary about mobilizing the patient which paradoxically results in non-application of the tension band principle. Osteosynthesis using non-absorbable suture material with circumferential wiring is an accepted procedure for fixation of such difficult fractures [6, 7].
Apart from the difficulties faced during fixation of comminuted and lower pole fractures with TBW, complications due to irritation surrounding soft tissues by k-wires, especially after the maximum knee flexion achieved by the patients, leading to resurgeries for removal of implants in about 40–60% of the patients. In this regard, non-absorbable sutures have lower rate of resurgeries and higher patient tolerance as they do not irritate soft tissues. In addition, this procedure can be performed quickly and is easier to perform resulting in reduced operative time and blood loss than the traditional TBW procedure [2, 8].
The main concern with fixation using non-absorbable sutures would be the strength of fixation compared to the regular K-wire and stainless-steel TBW fixation. Patel et al. concluded that both stainless-steel wire and high resistance non-absorbable polyester suture were equal in strength and provided excellent quality of fixation and in a similar study, Wright et al. demonstrated that non-absorbable sutures were more resistant than the stainless-steel wire. In another study, McGreal et al. subjected the cadaveric patella for 20,000 cycles of alternating flexion and extension cycles and concluded that braided polyester suture material can be an effective alternative to stainless-steel wire in fixation of patella [9, 10, 11].
Comminuted lower pole fractures are the main indication for partial patellectomy and resuturing of the patellar tendon. However, it causes early onset osteoarthritis secondary to patella baja due to reduced distance between the patella and the tibial tuberosity leading to increased patellofemoral contact pressure [12]. Various studies validate the use of non-absorbable sutures in such cases and they have concluded that the fixations done by sutures were of similar strength to that of stainless-steel wire fixation. Hence, comminuted lower pole fractures which otherwise needed excision or partial patellectomy can be preserved with this technique [10, 13].
Our results are compared with various other studies (Table 2). One of our patients had poor results as she presented with open fracture at first place and developed superficial infection postoperatively which was managed by intravenous antibiotics. She further developed stiffness and anterior knee pain as mobilization was delayed. None of our patients had complications like loss of reduction secondary to suture breakage and none of them required removal of fixation material due to knot prominence or any other reason as compared to other studies [21].
A long-term multicenter study with a greater number of patients is required to prove the benefits of this technique and to know the incidence of patellofemoral arthritis in these patients.
Open reduction and fixation with non-absorbable braided polyester sutures augmented with circumferential wiring are an effective method for the treatment of severely comminuted patella fractures and multifragmentary lower pole patella fractures which are not amenable to the traditional methods of internal fixation such as TBW and screw fixation. This technique can provide sturdy and firm fixation with good clinical, radiological, and functional outcomes with minimum complications.
This article highlights the use of simple technique with the use of non-absorbable braided polyester sutures with circumferential stainless-steel wiring in cases of severely comminuted patella fractures and lower pole fractures of patella when the gold standard modified TBW becomes a real technical challenge. It is a better alternative to the partial patellectomy as well. With good functional outcome and minimum complications, this technique can thus be an effective tool in the management of difficult patella fractures.
References
- 1.Galla M, Lobenhoffer P. Patella fractures. Chirurg 2005;76:987-97. [Google Scholar]
- 2.Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183-7. [Google Scholar]
- 3.Boström A. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand 1972;143 Suppl:1-80. [Google Scholar]
- 4.Henrichsen JL, Wilhem SK, Siljander MP. Treatment of patella fractures. Orthopaedics 2018;41:ae747-55. [Google Scholar]
- 5.Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop 1979;144:9-15. [Google Scholar]
- 6.Yang KH, Byun YS. Separate vertical wiring for the fixation of comminuted fractures of the inferior pole of the patella. J Bone Joint Surg Br 2003;85:1155-60. [Google Scholar]
- 7.Ong TK, Chee EK, Wong CL, Thevarajan K. Fixation of comminuted patellar fracture with combined cerclage and tension band wiring technique. Malays Orthop J 2008;2:40-2. [Google Scholar]
- 8.Wild M, Thelen S, Jungbluth P. Fixed-angle plates in patella fractures-a pilot cadaver study. Eur J Med Res 2011;16:41-6. [Google Scholar]
- 9.Patel VR, Parks BG, Wang Y, Ebert FR, Jinnah H. Fixation of patella fractures with braided polyester suture: A biomechanical study. Injury 2000;31:1-6. [Google Scholar]
- 10.Wright PB, Kosmopoulos V, Cote RE, Tayag TJ, Nana AD. FiberWire is superior in strength to stainless steel wire for tension band fixation of transverse patellar fractures. Injury 2009;40:1200-3. [Google Scholar]
- 11.McGreal G, Reidy D, Joy A, Mahalingam K, Cashman. The biomechanical evaluation of polyester as a tension band for the internal fixation of patellar fractures. J Med Eng Technol 1999;23:53-6. [Google Scholar]
- 12.Koval KJ, Kim YH. Patella fractures. Evaluation and treatment. Am J Knee Surg 1997;10:101-8. [Google Scholar]
- 13.Egol K, Howard D, Monroy A, Crespo A, Tejwani N, Davidovitch R. Patella fracture fixation with suture and wire: You reap what you sew. Iowa Orthop J 2014;34:63-7. [Google Scholar]
- 14.Camarda L, Morello S, Balistreri F, D’Arienzo A, D’Arienzo M. Non-metallic implant for patellar fracture fixation: A systematic review. Injury 2016;47:1613-7. [Google Scholar]
- 15.Wang P, Han X, Wang X, Yu J, Yuan Y, Tan H. Clincal observation of non-absorbable suture cerclage combined with patella claw fixation for treatment of inferior patella fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2020;34:1243-7. [Google Scholar]
- 16.Lue TH, Feng LW, Jun WM, Yin LW. Management of comminuted patellar fracture with non-absorbable suture cerclage and Nitinol patellar concentrator. Injury 2014;45:1974-9. [Google Scholar]
- 17.Chen CH, Huang HY, Wu T, Lin J. Transosseous suturing of patellar fractures with braided polyester a prospective cohort with a matched historical control study. Injury 2013;44:1309-13. [Google Scholar]
- 18.Gosal HS, Singh P, Field RE. Clinical experience of patellar fracture [Google Scholar]







