
O. anthropi is an emerging pathogen and there is an increase in the frequency of orthopaedic infection, this report suggests the ability of Onchycobacter anthropi to cause pyomyositis in immunocompetent patients.
Dr. Adnan Qamar, Department of Orthopaedic, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, Porur, India. E-mail: dmchadnan@gmail.com
Introduction:Ochrobactrum anthropi is an unusual low virulence emerging pathogen that rarely causes orthopedic infection and its clinical picture is not well described. It usually causes infection in immunocompromised hosts with indwelling catheters or foreign bodies, such as the central venous catheters.
Case Report:We reported a case of O. anthropi pyomyositis in a 22-year-old immunocompetent male patient not on any invasive procedure presented with raised temperature, left shoulder pain, and restriction of movements. Diagnosis was confirmed with the help of MRI and biopsy. He was successfully managed with surgical debridement and appropriate antibiotics.
Conclusion:Our case highlights the ability of O. anthropi to cause pyomyositis in immunocompetent individuals and its relevance in the field of orthopaedic infection.
Keywords:Ochrobactrum anthropi, pyomyositis, immunocompetent host.
Onchycobacter anthropi is a Gram-negative bacilli rarely implicated as human pathogen. This infection has been described in renal dialysis patients and immunocompromised individuals. We report a case of successfully treated O. anthropi pyomyositis in a 22-year-old immunocompetent patient.
A 22-year-old male presented to medicine OPD with a history of fever and body pain for 20 days duration. Fever was high grade and intermittent with chills. He also complained of the left shoulder pain and restriction of the left shoulder movements. Pain was insidious in onset, gradually progressive, non-radiating, aggravated on the left shoulder movements, and no relieving factor. On examination, his left shoulder warm, tender joint, was noted with severe restriction of shoulder movements. Laboratory finding shows white blood cell count of 5600. Blood culture was sent and the left shoulder MRI was done. He was started empirically on intravenous cefoperazone-sulbactam but he continued to have persistent high-grade fever (103 F).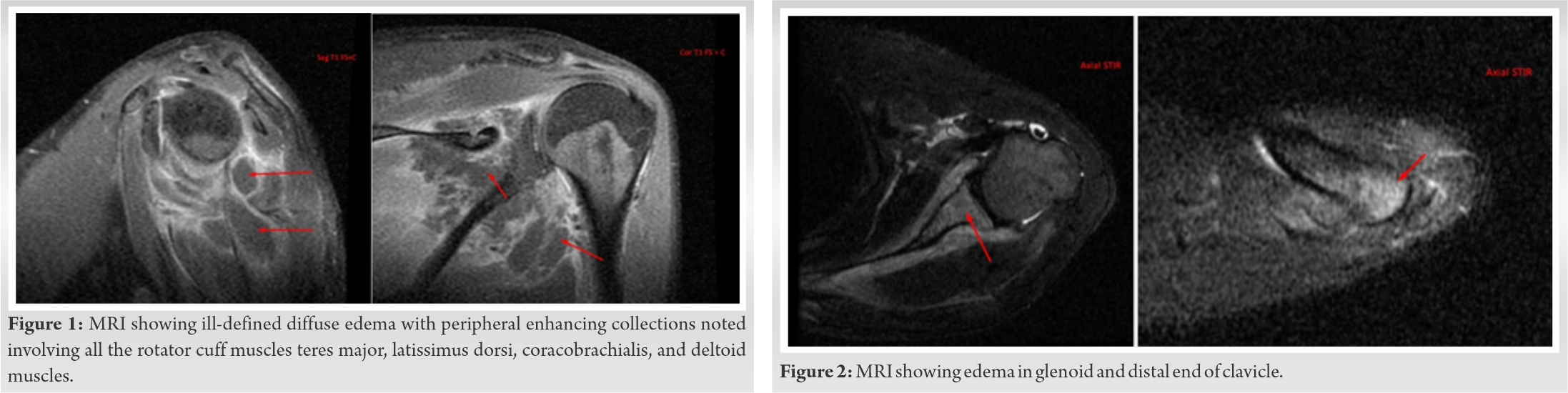
MRI shows ill-defined diffuse edema with peripheral enhancing collection involving all the rotator cuff muscles, teres major, latissimus dorsi, coracobrachialis and deltoid muscles with provisional diagnosis of pyomyositis with abscess (Fig. 1). MRI also shows marrow edema with patchy enhancement of glenoid, coracoid process, spine of scapula, distal end of clavicle, and acromion suggestive of osteomyelitis (Fig. 2). He was planned for surgical debridement. Surgical debridement was done and frank pus was evacuated. Tissue and pus were taken for biopsy, Genexpert MTB/RIF, Gram staining, and culture-sensitivity. Biopsy confirms pyomyositis (Fig. 3). Genexpert came out to be negative. Direct smear – Gram stain shows Gram-positive cocci in pairs. Organisms isolated in blood and pus culture-sensitivity as Ochrobactrum anthropi showing susceptibility testing of the organism to be sensitive to cotrimoxazole, imipenem, meropenem, tetracycline, tigecycline, piperacillin-tazobactam and resistance to amikacin, cefotaxime, ciprofloxacin, ceftazidime, cefepime, gentamicin, and levofloxacin. He was started on intravenous cotrimoxazole and meropenem. He had an uneventful recovery.
O. anthropi is an emerging pathogen even in immunocompetent patients and there may be an increase in the frequency of orthopedic infection caused by these organisms. This report suggests the ability of O. anthropi to cause pyomyositis in immunocompetent patients. Surgical debridement and treatment with appropriate antibiotics will produce successful results.
This case report underlines the importance of diagnosing pathology causing Onchycobacter anthropi pyomyositis in immunocompetent patients and it’s management. It should be kept in mind that an immunocompetent host does not rule out the Onchycobacter anthropi infection as previously thought.
References
- 1.Holmes B, Popoff M, Kiredjian M, Kersters K. Ochrobactrum anthropi gen. nov. from human clinical specimens and previously known as Group Vd. Int J Syst Bacteriol 1988;38:406-16. [Google Scholar]
- 2.Cieslak TJ, Robb ML, Drabick CJ, Fischer GW. Catheter associated sepsis caused by Ochrobactrum anthropi: Report of a case and review of related nonfermentative bacteria. Clin Infect Dis 1992;14:902-7. [Google Scholar]
- 3.Kämpfer P, Citron DM, Goldstein EJ, Scholz HC. Difficulty in the identification and differentiation of clinically relevant Ochrobactrum species. J Med Microbiol 2007;56:1571-3. [Google Scholar]
- 4.Gransden WR, Eykyn SJ. Seven cases of bacteremia due to Ochrobactrum anthropi. Clin Infect Dis 1992;15:1068-9. [Google Scholar]
- 5.Ezzedine H, Mourad M, Ossel MV, Logghe C, Squifflet P, Renault F, et al. An outbreak of Ochrobactrum anthropi bacteraemia in five organ transplant patients. J Hosp Infect 1994;27:35-42. [Google Scholar]
- 6.Vaidya S, Citron DM, Fine MB, Murakami G, Goldstein EJ. Pelvic abscess due to Ochrobactrum intermedium corrected in an immunocompetent host: Case report and review of the literature. J Clin Microbiol 2006;44:1184-6. [Google Scholar]
- 7.Kettaneh A, Weill F, Poilane I, Fain O, Thomas M, Hocqueloux L. Septic shock caused by Ochrobactrum anthropi in an otherwise healthy host. J Clin Microbiol 2003;41:1339-41. [Google Scholar]
- 8.Gill MV, Ly H, Mueenuddin M, Schoch PE, Cunha BA. Intravenous line infection due to Ochrobactrum anthropi (CDC group Vd) in a normal host. Heart Lung 1997;26:335-6. [Google Scholar]
- 9.Alnor D, Frimodt-Møller N, Espersen F, Frederiksen W. Infections with the unusual human pathogens Agrobacterium species and Ochrobactrum anthropi. Clin Infect Dis 1994;18:914-20. [Google Scholar]
- 10.Delière E, Vu-Thien H, Lévy V, Barquins S, Schlegel L, Bouvet A. Epidemiological investigation of Ochrobactrum anthropi strains isolated from a haematology unit. J Hosp Infect 2000;44:173-8. [Google Scholar]
- 11.Romano S, Aujoulat F, Jumas-Bilak E, Masnou A, Jeannot J, Falsen E, et al. Multilocus sequence typing supports the hypothesis that Ochrobactrum anthropi displays a human-associated subpopulation. BMC Microbiol 2009;18:267. [Google Scholar]
- 12.Elsaghir AF, James EA. Misidentification of Brucella melitensis as Ochrobactrum anthropi by API 20NE. J Med Microbiol 2003;52:441-2. [Google Scholar]






