
Shoulder injuries related to vaccine administration are not a common condition but, when present, they have a prolonged and torpid evolution.
Dr. Daniel Moya, Department of Orthopaedics, Hospital Británico de Buenos Aires, Argentina. E-mail: drdanielmoya@yahoo.com.ar
Abstract
Introduction: To confront the SARS-CoV-2 pandemic, a large share of the population must be immunized. Intramuscular vaccination of the shoulder is the preferred technique as it is easily exposed and guarantees a good immune reaction. Local side effects, such as pain and swelling, are common after deltoid inoculation. They usually resolve within 3 days. Shoulder injury related to vaccine administration (SIRVA) should be considered if the symptoms persist. The aim of this presentation is to describe a typical case of SIRVA after SARS-CoV-2 vaccination and provide information to the general orthopedic surgeon to properly diagnose, report, and treat these cases.
Case Report: To confront the SARS-CoV-2 pandemic, a large share of the population must be immunized. Intramuscular vaccination of the shoulder is the preferred technique as it is easily exposed and guarantees a good immune reaction. Local side effects, such as pain and swelling, are common after deltoid inoculation. They usually resolve within 3 days. Shoulder injury related to vaccine administration (SIRVA) should be considered if the symptoms persist. The aim of this presentation is to describe a typical case of SIRVA after SARS-CoV-2 vaccination and provide information to the general orthopedic surgeon to properly diagnose, report, and treat these cases.
Conclusion: SIRVA cases may occur and should be suspected in all individuals without a history of shoulder symptoms or dysfunction who experience sudden pain and reduced ROM following deltoid muscle vaccination. Treatment must be initiated early with corticosteroids and rehabilitation. The low probability of this complication does not outweigh the advantages of vaccination.
Keywords: SIRVA, subacromial subdeltoid bursitis, SARS-CoV-2, vaccination, shoulder injury.
To bring SARS-CoV-2 pandemic to an end, a large share of the world’s population needs to be immune to the virus. Around 40 million vaccines are now being administered daily [1]. The shoulder is easily exposed and thus the deltoid muscle is considered the preferred site for vaccination. Intramuscular inoculation optimizes the ability of the vaccine to generate an immune response, minimizes adverse reactions at the injection site, and has low association with local pain.
Local side effects are common after deltoid inoculation. These include pain at the injection site, erythema, swelling, bruising, tenderness, itching, and skin induration [2,3,4,5]. These minor complications are frequent, although they are most often mild and transient. They usually resolve in 2–3 days after the injection [2,3,4,5]. If the symptoms do not resolve, a Shoulder Injury Related to Vaccine Administration (SIRVA) should be considered [3,4,6,7,8,9,10]. SIRVA is a medicolegal term that describes a group of musculoskeletal conditions caused by improper administration of a vaccine in the deltoid muscle [10]. Certain clinical conditions must be present to define a complication as SIRVA [9,10]:
1. Pain onset <48 h after injection.
2. Symptomatology duration of at least 7 days.
3. Restricted range of motion (ROM).
4. No symptoms before vaccination.
Patients who meet these conditions are often diagnosed with inflammatory injuries such as bursitis and adhesive capsulitis, and rotator cuff tears. Other less frequent side effects are bicipital tendinopathy, glenohumeral synovitis, myositis, intramuscular sterile abscess, humeral osteitis, deltoid and rotator cuff effusion, erosive arthritis, septic arthritis, osteomyelitis, and osteonecrosis [3,4,5,6,7,8,9,10,11,12]. There have also been reports of nerve injuries, including the anterior branch of the axillary nerve, C6 radiculopathy, complete radial palsy, and Parsonage-Turner syndrome [13,14,15].
Since SIRVA’s initial description in 2010 [6], there is experience gained on the subject, especially in relation to the influenza vaccine. The massive vaccination campaign against COVID-19 is associated with the appearance of local complications related to the application of the vaccine. The aim of this presentation is to describe a typical case of SIRVA after SARS-CoV-2 vaccination and provide information to the general orthopedic surgeon to properly diagnose, report, and treat these cases.
A 69-year-old lady was referred to the senior author for persistent severe left shoulder pain and limited ROM 3 months after COVID-19 vaccination. The patient is a dentist with no history of shoulder pain, neurological, or rheumatoid conditions related to the scenario. On February 18, 2021, she received the first dose of the Sputnik V vaccine without any complications. Three weeks later, she was given the second dose, although this time, she noticed an improper application technique, claiming that the site of injection and the direction of the needle were too high (Fig. 1). Immediately after the application, she suffered intense pain and loss of active (ROM). She self-rated the pain as 10 out of 10 on the visual analog scale. The patient consulted several doctors who prescribed nonsteroidal anti-inflammatory drugs, intramuscular ketorolac, and pregabalin for 3 months, and she underwent rehabilitation with poor results.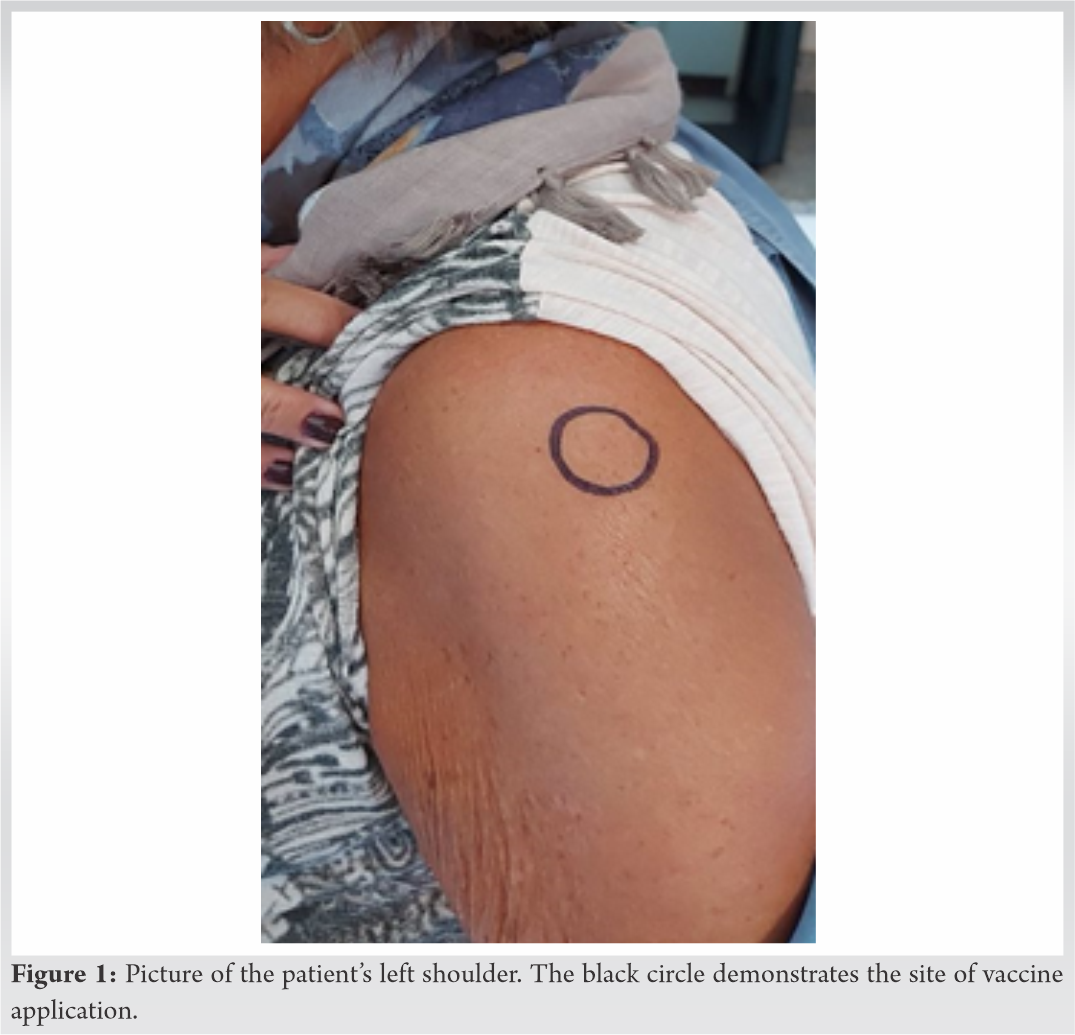
At the time of first consult with senior author, 3 months after the event, she complained of ongoing pain extending from the injection site to the mid upper arm with nocturnal exacerbation. She referred disability for most daily activities, including changing clothes. Her Simple Shoulder Test score was 0/12 = 0.0%. Physical examination revealed no visible swelling at injection site and neurovascular examination was normal. Active forward flexion was 80°, external rotation 10°, and internal rotation at the level of the sacroiliac joint. Neer and Hawkins’ tests were positive.
Plain film radiograph revealed only a mild acromioclavicular osteoarthritis, which was asymptomatic. Magnetic resonance imaging (MRI) results of the left shoulder done 5 days after the vaccination showed a mild subacromial-subdeltoid bursitis. A second MRI, done 2 months later, revealed distention of the subacromial-subdeltoid and subcoracoid bursas with associated synovial hypertrophy. After administration of intravenous contrast, intense synovial enhancement was observed (Fig. 2). These findings showed evidence of inflammatory changes. No glenohumeral joint effusion or rotator cuff tears were noted. No laboratory studies were requested at that time.
We rule out infection and neurological injuries and prescribed an intramuscular dose of depot betamethasone and a home-based program of gentle exercises. She had a quick initial response to treatment, with a marked decrease in pain, and improvement in active ROM. However, after two months of treatment, her recovery slowed and still requires NSAIDs and physical therapy several (pondría los meses) months of treatment, she presented no improvements in ROM and persisted with shoulder pain. New MRI results showed signs of adhesive capsulitis at the rotator interval and subdeltoid bursitis (Fig. 3). We performed arthroscopic bursectomy and arthrolysis at the rotator interval. Tissue samples taken for histopathological analysis showed the presence of chronic inflammation of the subdeltoid bursa. Three months after surgery, the patient has shown a substantial decrease in pain and improvements in ROM, especially in external rotation and abduction and has been able to return to her professional activity.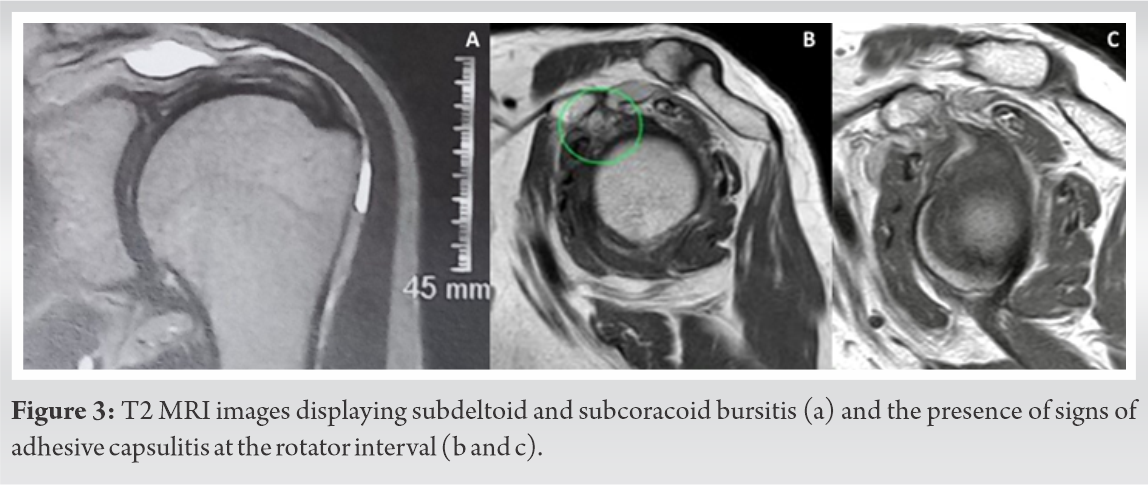
Experience with influenza shows that an estimated 60–80% of the people who receive the vaccine report shoulder tenderness, swelling, and pain [11]. The exact rate of severe local complications secondary to vaccination in the shoulder area is not known. In 2018, there were 10,230 reported influenza vaccination-related complications of varying severity, representing only 0.006% of influenza-vaccinated population. Of these reports, 27 individuals (0.000017%) described self-limited shoulder pain or synovitis [16]. The complication rates are currently unknown for the SARS-CoV-2 vaccine.
Most SIRVA cases are middle-aged women [6] with pain starting within the first 48 h after vaccination [7,9,10,17]. In general, the injury is generated by an inadequate inoculation technique [3,4,5,6,8,9]. In our case, the patient, who is a health-care professional, informed a misplaced and abrupt application of the vaccine. The described mistake was a superior and oblique placement of the needle in relation with the subacromial space. It has been postulated that when the vaccine solution is inadvertently injected into a synovial space, pre-existing antibodies from previous infections or vaccines can lead to an excessive inflammatory reaction [4,9]. Although several studies support the possibility of SIRVA being an immune response, a definitive clinical study to support this theory has not been done [7].
Typically, SIRVA patients present with severe pain and decreased ROM after inoculation of the vaccine [6,10,17,18]. The pain is moderate to severe, is localized within the deltoid area, extends to the lateral aspect of the arm, and is usually greater than would be expected from simple needle trauma [4,6]. Initially, any neurological injury and infection should be ruled out. Radiographs are often non-specific and generally do not provide useful diagnostic information [18]. Increased fluid within the subacromial/subdeltoid bursa is a common finding on ultrasound and MRI [9]. It is recommendable to request laboratory tests including complete blood count, erythrocyte sedimentation rate, and acute-phase reactants, regardless of the onset of symptoms.
The diagnosis of a SIRVA in the deltoid region may seem obvious and simple, but the patient is not always initially evaluated by an orthopedic surgeon, therefore, a variety of usual orthopedic diseases may be overlooked. A case reported by Smith et al. [11] was treated with gabapentin with a prior diagnosis of Parsonage-Turner’s disease, but it turned out to be proximal humerus osteomyelitis. In our case, the patient was diagnosed as a neurological disorder and prescribed with pregabalin for 3 months without clinical response.
There is no consensus in the literature on how to manage SIRVA. Once the infection has been ruled out, while considering that it is an acute inflammatory process that can affect different structures of the shoulder, it is ideal to immediately start the administration of corticosteroids [4,5,6,7,10,17]. Rehabilitation with gentle exercises, including a home exercise program, is essential [7,18]. Its early and progressive implementation contributes to pain control and prevents the development of frozen shoulder. This injury should not be underestimated, as the process of healing can take from weeks to years [4,6]. In the series published by Atanasoff et al. [6], 31% of the cases required surgical intervention and even a second surgery in half of them. The treating physician has the duty to report to the health authorities these cases of adverse events that are supposedly attributable to vaccination and immunization, according to the legislation of each country.
SIRVA cases are rare, but when they occur, their evolution is torpid and their management complicated. This condition should be suspected in all individuals without a history of shoulder symptoms or dysfunction who experience sudden pain and reduced ROM after deltoid inoculation. Neurological lesions and infection should be ruled out. Treatment must be initiated early, and it includes the use of corticosteroids and rehabilitation. However, the low probability of this complication occurring does not outweigh the enormous advantages of vaccination.
The COVID-19 pandemic brought the need for massive global vaccination. The vaccine is applied in the deltoid muscle and is associated with a range of specific complications that must be known to the general orthopedist. Shoulder injury related to vaccine administration may occur after an improper application technique and should be suspected and treated accordingly when symptoms persist after 7 days.
References
- 1.1. Our World in Data. Coronavirus (COVID-19) Vaccinations. Available from: https://www.ourworldindata.org/covid-vaccinations [Google Scholar | PubMed]
- 2.2. Martín Arias LH, Sanz Fadrique R, Sáinz Gil M, Salgueiro-Vazquez ME. Risk of bursitis and other injuries and dysfunctions of the shoulder following vaccinations. Vaccine 2017;35:4870-6. [Google Scholar | PubMed]
- 3.3. Szari S, Belgard A, Adams K, Freiler J. Shoulder injury related to vaccine administration: A rare reaction. Fed Pract 2019;36:380-4. [Google Scholar | PubMed]
- 4.4. Cantarelli Rodrigues T, Hidalgo PF, Skaf AY, Serfaty A. Subacromial-subdeltoid bursitis following COVID-19 vaccination: A case of shoulder injury related to vaccine administration (SIRVA). Skeletal Radiol 2021;50:2293-7. [Google Scholar | PubMed]
- 5.5. Massel DH, Haziza S, Rivera S, Mohile N, Subhawong TK, Hernandez VH. Septic arthritis of the shoulder after SARS-CoV-2 pfizer vaccination: A case report. JBJS Case Connect 2021;11:90. [Google Scholar | PubMed]
- 6.6. Atanasoff S, Ryan T, Lightfoot R, Johann-Liang R. Shoulder injury related to vaccine administration (SIRVA). Vaccine 2010;28:8049-52. [Google Scholar | PubMed]
- 7.7. Cagle PJ Jr. Shoulder injury after vaccination: A systematic review. Rev Bras Ortop (Sao Paulo) 2021;56:299-306. [Google Scholar | PubMed]
- 8.8. Chuaychoosakoon C, Parinyakhup W, Tanutit P, Maliwankul K, Klabklay P. Shoulder injury related to Sinovac COVID-19 vaccine: A case report. Ann Med Surg (Lond) 2021;68:102622. [Google Scholar | PubMed]
- 9.9. Natanzi N, Hebroni F, Bodor M. Teres minor injury related to vaccine administration. Radiol Case Rep 2020;15:552-5. [Google Scholar | PubMed]
- 10.10. Hibbs BF, Ng CS, Museru O, Moro PL, Marquez P, Woo EJ, et al. Reports of atypical shoulder pain and dysfunction following inactivated influenza vaccine, Vaccine Adverse Event Reporting System (VAERS), 2010-2017. Vaccine 2020;38:1137-43. [Google Scholar | PubMed]
- 11.11. Smith SS, Lee Y, Wang L. Adolescent with osteomyelitis after intramuscular administration of a vaccine: A case report. J Am Pharm Assoc 2020;60:e357-60. [Google Scholar | PubMed]
- 12.12. Kuether G, Dietrich B, Smith T, Peter C, Gruessner S. Atraumatic osteonecrosis of the humeral head after influenza A-(H1N1) v-2009 vaccination. Vaccine 2011;29:6830-3. [Google Scholar | PubMed]
- 13.13. Meirelles H, Filho GR. Axillary nerve Injury caused by deltoid muscle intramuscular injection: Case report. Rev Bras Ortop 2004;39:615-9. [Google Scholar | PubMed]
- 14.14. Ling CM, Loong SC. Injection injury of the radial nerve. Injury 1976;8:60-2. [Google Scholar | PubMed]
- 15.15. Mahajan S, Zhang F, Mahajan A, Zimnowodzki S. Parsonage turner syndrome after COVID-19 vaccination. Muscle Nerve 2021;64:E3-4. [Google Scholar | PubMed]
- 16.16. Littrell LA, Leslie DF, Bierle DM, Wenger DE. Progressive monoarticular inflammatory arthritis following influenza vaccination. Mayo Clin Proc Innov Qual Outcomes 2021;5:204-9. [Google Scholar | PubMed]
- 17.17. Macomb CV, Evans MO, Dockstader JE, Montgomery JR, Beakes DE. Treating SIRVA early with corticosteroid injections: A case series. Mil Med 2020;185:e298-300. [Google Scholar | PubMed]
- 18.18. Wright A, Patel R, Motamedi D. Influenza vaccine-related subacromial/subdeltoid bursitis: A case report. J Radiol Case Rep 2019;13:24-31. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 10, 2021 Inversed V-shaped High Tibial Osteotomy for Severe Varus Deformity due to Blount Disease: A Case Report
September 10, 2021 Inversed V-shaped High Tibial Osteotomy for Severe Varus Deformity due to Blount Disease: A Case Report June 10, 2024 What the Physician Needs to Know about Charcot Arthropathy and Ankle Fracture Treatment Dilemma: A Case Report and a Possible Medical Approach and Treatment Algorithm
June 10, 2024 What the Physician Needs to Know about Charcot Arthropathy and Ankle Fracture Treatment Dilemma: A Case Report and a Possible Medical Approach and Treatment Algorithm December 10, 2022 The Use of External Fixator and Iliac Crest Bone Graft in Traumatic Metacarpal Bone Defect
December 10, 2022 The Use of External Fixator and Iliac Crest Bone Graft in Traumatic Metacarpal Bone Defect November 10, 2023 Ipsilateral Knee Dislocation and Ankle Fracture Dislocation
November 10, 2023 Ipsilateral Knee Dislocation and Ankle Fracture Dislocation