
The case is rare, at the time of writing there are only a handful of published papers detailing a fracture through an Exeter stem implant. In patients having undergone arthroplasty and especially those reporting pain, we urge clinicians to consider the possibility of Exeter stem implant fracture.
Dr. Ahmed Daoub, Department of Orthopaedic Surgery, Hereford County Hospital, Wye Valley NHS Trust, Hereford, United Kingdom, The Robert Jones and Agnes Hunt Specialist Orthopaedic Hospital, Oswestry, United Kingdom. E-mail: ahmed.daoub@nhs.net
IntroductionThe Exeter stem by Stryker is a polished, double wedge, tapered,and stainless steel cemented implant that is known to have high mechanical strength, and therefore can carry a significant load.
Case ReportDue to the rare nature of fractures of this type of implant, its success and effectiveness within hip arthroplasty, the Exeter stem has become one of the most commonly used surgical treatment regimens for hip fractures. At present, there are only a handful of published papers detailing a fracture through an Exeter stem implant.
ConclusionThe current case report documents a rare case of a fractured Exeter V40 stem and its subsequent treatment.
KeywordsRevision arthroplasty, Exeter stem, Implant failure.
Fractures of first-generation femoral stems are relatively common, with incidence as high as 4.1% within some designs; and when they do occur can be the most problematic complication following primary hip arthroplasty [1]. More recently significant alterations to the materials used to make stems, as well as their design and the surgical procedures utilized have meant that stem failures have become a rare occurrence. The Exeter stem is a polished, double wedge, tapered cemented implant made with stainless steel. Although originally manufactured using polished ductile stainless steel, issues with subsidence meant the stem began to be made with a matte surface with 316L stainless steel, which was later changed to wrought high nitrogen Orthniox – a material known to have increased fatigue strength [1]. This change in material meant a reduction in the production of material debris around the interface of the implant and cement that could result in endosteal osteolysis, but increased rates of stem loosening. Despite this, it was found that controlled subsidence was beneficial, and the stem returned to being manufactured in polished material. Scheerlinck and Casteleyn noted that the Exeter implant utilizes a loaded-taper model within which the stem includes two or three tapered planes and reduces stress, in both the proximal and distal cement mantle, by the wedge of the stem becoming lodged in the cement mantle during the process of axial loading [2]. The current case report details a single incidence of a revision Exeter stem fracture within an elderly patient. Our hope is that this information can be used by surgeons to inform their decisions and improve patient outcomes.
An 83-year-old gentleman (90kg, 178cm, body mass index: 28.4kg/m2) presented with a 10 day history of pain in the right hip and a 4 day history of inability to fully weight bear following a fall. He originally had a right uncemented total hip replacement for osteoarthritis performed in May 2009. Due to aseptic loosening, the original replacement failed and was revised to a cemented Exeter V40 stem in 2012. A further revision was performed in 2017 for dislocation. On examination, his right leg was short and externally rotated. There was also tenderness in the right groin. Radiographs showed the hip still in joint and a fracture of the Exeter stem (Fig. 1). The patient had revision surgery through the posterior approach utilizing the old incision. Before this, he underwent aspiration of this right hip to exclude infection. Prophylactic antibiotics and tranexamic acid were administered at induction as per hospital protocol. Following dislocation of the hip, the acetabular component was found to be well fixed and was left in situ. The proximal fragment of the Exeter stem was removed with ease. The distal fragment was removed with difficulty following a 1cm × 3cm osteotomy distal to the tip of the stem, a drill to penetrate the cement mantle and explanted using a punch (Fig. 2). There was no overt sign of infection and the tissues looked healthy macroscopically. Five tissue samples were sent to microbiology for culture and sensitivity. Subsequently, the femur was prepared for a V40 Exeter revision stem (44 offset and 125mm length) after trial reduction. A 1.5 mixture of Palacos cement with gentamicin was used. The hip was reduced with a Dual mobility bearing using a 28mm Biolox Delta head and a 28/52mm X3 insert for modular dual mobility. Intraoperatively, the hip was stable and leg length restored.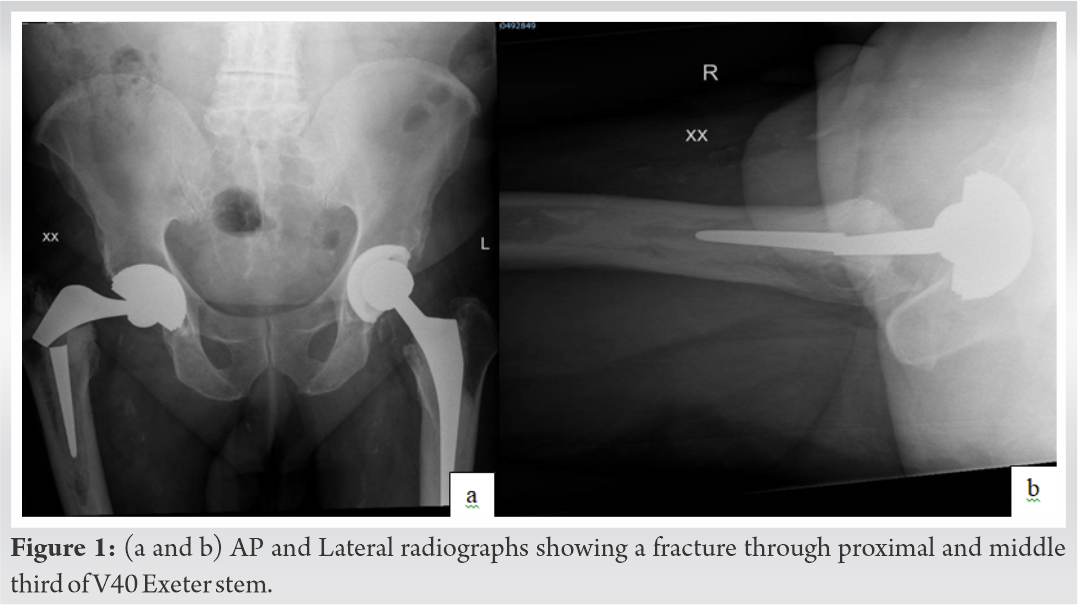
Post-operative care included routine observations, a further three doses of antibiotics, bloods, Venous thromboembolism prophylaxis and a check X-ray (Fig. 3). The patient was mobile with a frame day 1 postoperatively. At 6 week follow-up, he was fully weight bearing independently with full range of motion in the hip. We plan to review him again in 6 months’ time.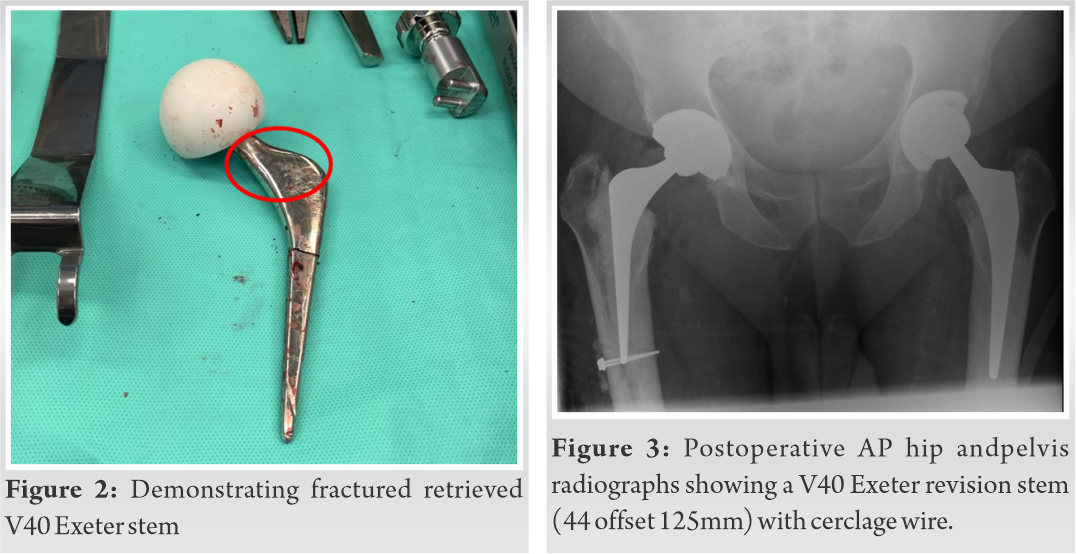
At present, the Exeter stem is used within 64% of all cemented hip replacements in the UK [1]. The Exeter stem has been found to produce survivorship of a minimum of 20 years among younger patients. In a study utilizing a mean follow-up of 22 years, only one broken Exeter stem was reported among 130 hip arthroplasties and [3], among older patients, stem fractures are incredibly rare. Within the latest V40 version of the Exeter stem fractures are rare – Facek et al. found a small number reported in the peer-reviewed literature, with most occurring in earlier versions of the stem that utilized inferior designs or materials [4]. Revision surgery for femoral stems, as a result of metalwork fracture, is also rare –Samra et al. found 80 reported cases out of 800,000 between 1991 and 2008, globally [6 ]. The most common reasons for revision surgery are aseptic loosening, osteolysis, infection, and dislocation. Within the body, the greatest amount of stress is placed on the middle third of the stem, and this is where fractures most commonly occur. In vivo, cantilever bending, stress placed on the stem, and stress concentration can lead to fracture [1]. The factors associated with increased risk of metalwork fracture relate to the patient (e.g., increased BMI and reduced bone stock)are biological (e.g., osteolysis and inadequate proximal osseous support),and relate to the implant (e.g., undersizing and material defects) [5].
Within the current report, we present a case of a failed Exeter stem in an elderly patient with previous revision hip arthroplasty. Although rare, given the aging population and associated increased need for hip replacements, it is likely that more fractures of this nature will be reported. Therefore, clinicians must have as much information as is available, in order to understand the factors associated with failures, its complications and to improve patient outcomes. In patients having undergone arthroplasty, and especially those reporting pain, we urge clinicians to consider the possibility of Exeter stem implant fracture.
The case is rare, at the time of writing there are only a handful of published papers detailing a fracture through an Exeter stem implant. Our hope is that this information can be used by surgeons to inform their decisions and improve patient outcomes.
References
- 1.1. Bolland BJ, Howell JR, Hubble MJ, Timperley AJ, Gie GA, Ling RS. Fractures of the exeter femoral prosthesis: Incidence, aetiology, and factors predisposing to failure. J Bone Joint Surg Br 2012;94:322-7. [Google Scholar]
- 2.2. Scheerlinck T, Casteleyn PP. The design features of cemented femoral hip implants. J Bone Joint Surg Br 2006;88:1409-18. [Google Scholar]
- 3.3. Keeling P, Howell JR, Kassam AA, Sathu A, Timperley AJ, Hubble MJ, et al. Long-term survival of the cemented exeter universal stem in patients 50 years and younger: An update on 130 hips. J Arthroplasty 2020;35:1042-7. [Google Scholar]
- 4.4. Facek M, Khatib Y, Swarts E. Prosthetic fracture of a cemented exeter femoral stem. Reconstruct Rev 2016;6:35. [Google Scholar]
- 5.5. Davies BM, Branford White HA, Temple A. A series of four fractured exetertm stems in hip arthroplasty. Ann R Coll Surg Engl 2013;95:e130-2. [Google Scholar]
- 6.6. Inderpaul Samra * and Christos Paliobeis. A Dual Biomechanical Failure: Exeter Stem and Pubic Rami Insufficiency Fracture, following Hybrid Total Hip Arthroplasty. Case Rep Orthop. 2015; [Google Scholar]



