
Intraosseous hibernomas may mimic a primary bone tumor and one should have a high index of suspicion. Hibernomas should be considered as a differential diagnosis of sclerotic bone lesion associated with soft tissue mass even in adults.
Dr. Abhishek Kumar Rai, Department of Orthopaedics, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India. E-mail: abhishek110891@gmail.com
IntroductionHibernoma is an uncommon benign tumor composed of multivacuolated brown adipocytes described in the literature a decade back. Intraosseous hibernomas are extremely rare with propensity to affect axial skeleton. Involvement of appendicular skeleton has been reported only twice in the literature till date.
Case ReportWe present a case of solitary, painless mass in the left proximal tibia mimicking neoplasm in a 35-year-old male. The plain radiographs revealed a lytic lesion with well-defined margin at the junction of metaphyseal-diaphyseal region of the left proximal tibia. The lesion was hyperintense on T2 and hypointense on T1 with heterogenous enhancement on contrast imaging. FDG-PET showed high uptake of fluorodeoxyglucose. Histopathological examination revealed the presence of multivacuolated cytoplasm with abundant mitochondria suggestive of hibernoma. On immunohistochemistry, the cells were positive for S-100.
ConclusionThe findings of imaging modalities are non-specific and histopathological examination is required to confirm the diagnosis of hibernoma. Intraosseous hibernoma needs to be considered as a differential diagnosis of sclerotic bone lesion. Further, evaluation with regular follow-up with imaging will be required if the mass undergoes any clinical changes. Both radiologists and pathologists, need to be aware of this rare entity to avoid misdiagnosis of the uncommon lesion.
KeywordsIntraosseous hibernoma , brown fat tumor, appendicular skeleton.
Hibernomas are rare, benign soft- tissue tumor containing multivacuolated cytoplasm resembling brown adipose cells [1]. It was first identified by Merkel in 1906 and described it as “pseudolipoma”. In 1914, Grey Gray found that the cell has resemblance with the brown fat of hibernating animals and thus coined the term “Hibernoma” [2]. Brown fat is a characteristic feature of new born mammals which is are responsible for non-shivering thermoregulatory functions. They are found in abundance in supraclavicular, tracheal, mediastinal, and paravertebral areas [3]. The presence of high number of microvesicles and mitochondria, confers the eponymous brown colour to the tissue. Hibernomas are usually found in the subcutaneous and muscle tissue around the axial skeleton. Intraosseous hibernoma is an entity, rare in Oorthopaedics with less than ten cases documented in the literature. Hibernoma usually affects axial skeleton [4]. Intraosseous hibernoma of an appendicular skeleton is extremely rare with only two cases reported in the literature. Hibernomas are known to have no malignant potential with no reports of malignancy of brown fat reported in the literature .[5]. We report a case of an intraosseous hibernoma which was an incidental finding in the left proximal tibia of a 35-year-old male.
A 35-year-old male, presented to our outpatient department with complaints of painless solitary mass over the left proximal tibia. The swelling was insidious in onset, gradually progressed for over a period of two 2 years. The swelling was pea sized to begin with, which gradually progressed to a present size of 9 × ×8 cm (Fig. 1). On clinical examination of the swelling, there was no local warmth, tenderness, crepitus, or discoloration of the overlying skin. The swelling was firm in consistency which was adhered to the underlying structures. There were no palpable lymph nodes. The regional radiographs revealed a large lytic lesion with well-defined margins and narrow zone of transition without cortical breech or periosteal reaction in the metaphyseal -diaphyseal region of the left proximal tibia (Fig. 2). The radiographs of skeletal survey showed no lesions elsewhere. The regional magnetic resonance imaging (MRI) of tibia showed ill-defined serpiginous areas of heterogenous T2 hyperintensity and T1 hypointensity involving left proximal tibia (Fig. 3). On post post-contrast study, these areas show heterogenous enhancement. In the given clinical setting, the above findings were suggestive of bone infarcts. Heterogenous T2 hyperintense with T1 hypointense subcutaneous collection was seen along the anterior aspect of the left proximal tibia and seen communicating with marrow cavity through above- mentioned cortical defect. For further details and to locate the potential primary tumor, Positron Emission Tomography was performed which showed a circumscribed sclerotic lesion with high Fluorodeoxyglucose avidity in the left proximal tibia with no other abnormalities elsewhere (Fig. 4). Considering high metabolic activity in a solitary lesion, a biopsy was planned from the most representative part of the swelling. Four core samples were obtained using an 18-gauge biopsy device and histopathology suggested fat cells in organoid arrangement of uniform large cells resembling brown fat with coarsely granular to multivacuolated cytoplasm surrounded by fibrovascular tissue (Fig. 5).The cells were positive for S-100 protein. The cells had multiple adipocytes with numerous mitochondria. There is not even a single case reported in the literature which suggests malignant potential in hibernomas. Following biopsy, the decision was made to follow this lesion clinically and to keep a close follow- up every 6 monthly. The patient was followed up for two 2 years for clinico-radiological evaluation. The solitary mass did not further progress in size and was painless. Given the unique quality of this case, the anticipated natural course of this mass in the absence of additional treatment is not known. Further, evaluation with regular follow-up with imaging will be required if the mass undergoes any clinical changes.
The radiographs of skeletal survey showed no lesions elsewhere. The regional magnetic resonance imaging (MRI) of tibia showed ill-defined serpiginous areas of heterogenous T2 hyperintensity and T1 hypointensity involving left proximal tibia (Fig. 3). On post post-contrast study, these areas show heterogenous enhancement. In the given clinical setting, the above findings were suggestive of bone infarcts. Heterogenous T2 hyperintense with T1 hypointense subcutaneous collection was seen along the anterior aspect of the left proximal tibia and seen communicating with marrow cavity through above- mentioned cortical defect. For further details and to locate the potential primary tumor, Positron Emission Tomography was performed which showed a circumscribed sclerotic lesion with high Fluorodeoxyglucose avidity in the left proximal tibia with no other abnormalities elsewhere (Fig. 4). Considering high metabolic activity in a solitary lesion, a biopsy was planned from the most representative part of the swelling. Four core samples were obtained using an 18-gauge biopsy device and histopathology suggested fat cells in organoid arrangement of uniform large cells resembling brown fat with coarsely granular to multivacuolated cytoplasm surrounded by fibrovascular tissue (Fig. 5).The cells were positive for S-100 protein. The cells had multiple adipocytes with numerous mitochondria. There is not even a single case reported in the literature which suggests malignant potential in hibernomas. Following biopsy, the decision was made to follow this lesion clinically and to keep a close follow- up every 6 monthly. The patient was followed up for two 2 years for clinico-radiological evaluation. The solitary mass did not further progress in size and was painless. Given the unique quality of this case, the anticipated natural course of this mass in the absence of additional treatment is not known. Further, evaluation with regular follow-up with imaging will be required if the mass undergoes any clinical changes. 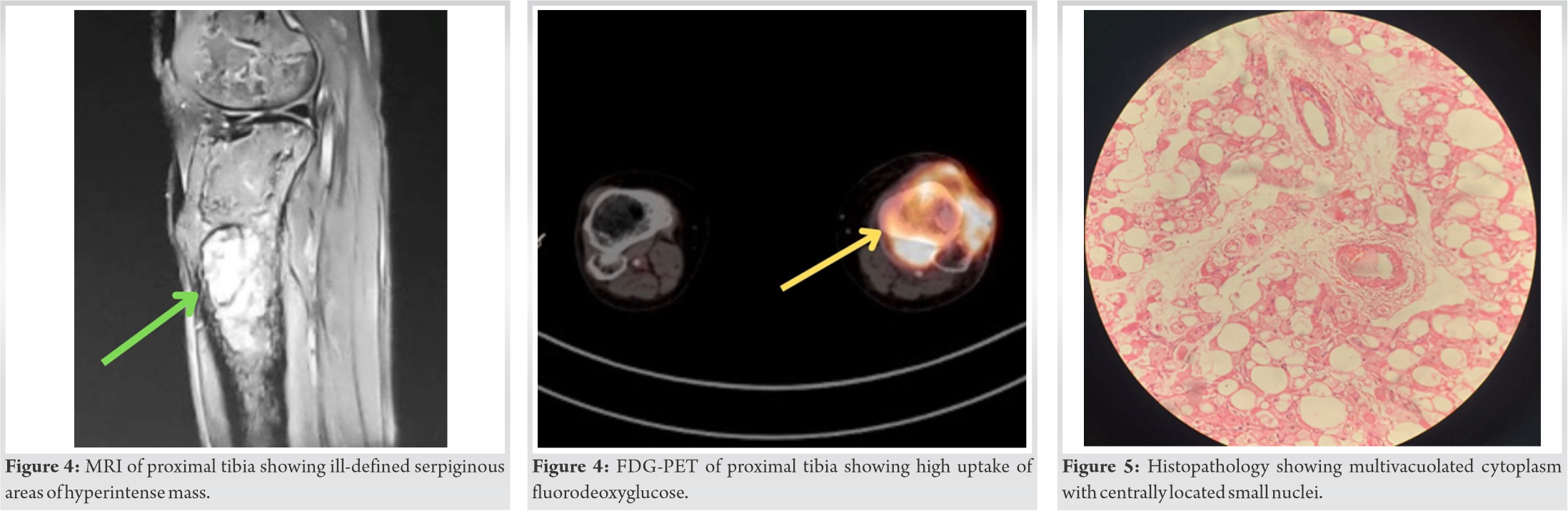
Hibernoma is an extremely rare benign tumor formed in soft tissue, mainly composed of brown fat. Hibernomas represent less than <2% of all benign adipocytic tumors. Brown fat, a characteristic feature of mammalian species, is mainly found in the axial skeleton of newborn and hibernating animals. It most commonly involves male with maximum preponderance in the fourth decade. The brown fat has role in the non-shivering thermogenesis. The brown fat tends to disappear gradually over time by adulthood, but may remain in patches in the axial skeleton. Hibernomas are rare in the bone, with less than ten cases of intraosseous hibernoma reported in the Caucasians. Most of the time, intraosseous hibernomas are reported incidentally during detailed clinico-radiological examination. The hibernomas are mostly reported in axial skeleton [6]. They are usually asymptomatic with only one reported case having symptoms. The patient was a known case of ovarian carcinoma presented with chest pain and shortness of breath. Computed Tomography Angiography (CTA) was done to rule out pulmonary embolism. CTA showed sclerotic lesion in T3 vertebral body. A biopsy was planned which confirmed the diagnosis of intraosseous hibernoma. The symptomatic case was managed by radiofrequency ablation with complete resolution of symptoms within a year [7]. The intraosseous hibernomas are sclerotic on plain radiographs and computed tomography. The presence of sclerosis is a non-specific finding which can be seen in any reactive cases. On MRI, the lesion is hyperintense on T2 and hypointense on T1 with heterogenous hyperintensity on contrast images. The brown fat contains numerous mitochondria which are responsible for hypermetabolism [8]. The FDG-PET shows mild to high avidity of fluorodeoxyglucose. The radiological imaging of hibernoma is not characteristic and suggests the possibility of various differential diagnosis. The common ones include hemangioma, liposarcoma, lymphoma, metastatic carcinoma, and osteomyelitis. Hemangiomas are hyperintense, both on T1 and T2 and cold on bone scan. To rule out malignancy and to establish the diagnosis of hibernoma, histopathological examination is a must. Hibernoma cells resemble adipocytes containing multivacuolated cytoplasm with abundant mitochondria. On immunohistochemistry, hibernomas are positive for S-100 protein and negative for cytokeratins, desmin, and CD68 [9]. The histological examination resembles foamy histiocytosis which can be differentiated on immunohistochemistry as they are CD68 positive. The first case of intraosseous hibernoma was reported by Thorns et al. in 2008 [10]. Bonar et al. reported a case series of intraosseous hibernoma consisting of five patients. The findings of imaging modalities are non-specific and histopathological examination is required to confirm the diagnosis of hibernoma [11, 12]. The pathologists need to consider hibernoma as a differential diagnosis of adipocytic tumors associated with sclerosis of bone. The advancement in the radiological imaging especially FDG-PET has resulted in reporting of more cases of hibernoma.
Intraosseous hibernomas are extremely rare benign tumor of brown fat resembling adipocytic tumors. The radiological imaging is highly non-specific and histopathological examination is a must for confirming the diagnosis. The increasing awareness among pathologists and radiologists will avoid missing the diagnosis of this rare entity.
Intraosseous hibernomas are extremely rare and are discovered as an incidental finding. The radiological imaging of hibernoma resembles sclerotic lesion of bone. Hibernomas should be considered as a differential diagnosis of sclerotic bone lesion associated with soft- tissue mass.
References
- 1.Song B, Ryu HJ, Lee C, Moon KC. Intraosseous hibernoma: A rare and unique intraosseous lesion. J Pathol Transl Med 2017;51:499-504. [Google Scholar]
- 2.Bonar SF, Watson G, Gragnaniello C, Seex K, Magnussen J, Earwaker J. Intraosseous hibernoma: Characterization of five cases and literature review. Skeletal Radiol 2014;43:939-46. [Google Scholar]
- 3.Jerman A, Snoj Ž, Kuzmanov BG, Novak AK. Intraosseous hibernoma: Case report and tumor characterization. BJR Case Rep 2015;1:20150204. [Google Scholar]
- 4.Westacott L, Collins A, Dickenson I. Intraosseous hibernoma in the sacrum of an adult. Int J Surg Pathol 2016;24:749-52. [Google Scholar]
- 5.Bai S, Mies C, Stephenson J, Zhang PJ. Intraosseous hibernoma: A potential mimic of metastatic carcinoma. Ann Diagn Pathol 2013;17:204-6. [Google Scholar]
- 6.Sohn MH, Lim ST, Jeong HJ, Kim DW, Jang KY, Yim CY, et al. Intraosseous lipoma in the femoral shaft mimicking a bone metastasis on bone scintigraphy. Clin Nucl Med 2009;34:693-5. [Google Scholar]
- 7.Ko A, Rowell CC, Vogler JB 4th, Samoilov DE. Intraosseous hibernoma: A metastatic mimicker to consider on the differential. Radiol Case Rep 2020;15:2677-80. [Google Scholar]
- 8.Kang HS, Kim T, Oh S, Park S, Chung SH. Intraosseous lipoma: 18 Years of experience at a single institution. Clin Orthop Surg 2018;10:234-9. [Google Scholar]
- 9.Vlychou M, Teh J, Whitwell D, Athanasou NA. Intraosseous hibernoma: A rare adipocytic bone tumour. Skeletal Radiol 2016;45:1565-9. [Google Scholar]
- 10.Thorns C, Schardt C, Katenkamp D, Kähler C, Merz H, Feller AC. Hibernoma-like brown fat in the bone marrow: Report of a unique case. Virchows Arch 2008;452:343-5. [Google Scholar]
- 11.Kumar R, Deaver MT, Czerniak BA, Madewell JE. Intraosseous hibernoma. Skeletal Radiol 2011;40:641-5. [Google Scholar]
- 12.Gitto S, Doeleman T, de Sande MA, Langevelde K. Intraosseous hibernoma of the appendicular skeleton. Skeletal Radiol 2022;51:1325-30. [Google Scholar]








