
The arm squeeze test is a simple but often overlooked test to differentiate between cervical and shoulder pathology, which could be implemented into routine practice to avoid needless surgical intervention.
Dr. George Ampat, School of Medicine, Institute of Life Course & Medical Sciences, Faculty of Health & Life Sciences, University of Liverpool, Liverpool, United Kingdom. Email: geampat@liverpool.ac.uk
Abstract
Background: Diagnostic dilemma exists in differentiating between neck and shoulder pathology, as both can give a rise to shoulder and arm symptoms. In addition, the hypersensitivity of magnetic resonance imaging (MRI) scans may wrongly highlight non-clinically significant changes as potential targets for surgical intervention. The arm- squeeze test is a recognised recognized method used to help differentiate pathology arising from the shoulder or the neck. Performing this test preoperatively may prevent needless surgical intervention when diagnostic difficulties exist, even when MRI scans are not helpful.
Case Presentation: We report the case of a 41-year-old male who initially presented with numbness and pins and needles in both arms. Following clinical review and an MRI scan of the cervical spine, the patient underwent an Anterior Cervical Discectomy and Fusion. Unfortunately, there was no relief of symptoms following surgery. A post- operative clinical review identified the shoulder as a potential cause of the symptoms.
Conclusion: The arm- squeeze test is not popular and is not routinely used in shoulder and cervical spine examinations. However, it is recommended by National Institute for health and care excellence to help differentiate between neck and shoulder pathology, and, hence, dissemination of this information is vital.
Keywords: Anterior cervical discectomy and fusion, unnecessary surgery, arm- squeeze test, differentiating neck and shoulder pathology.
Increasingly sedentary lifestyles have caused the incidence of neck pain to rise, although it remains at a lower incidence than that of back pain. At present, it is estimated that up between 10% and 20% of the population experience neck pain each year and 70% of the population will have at least one episode of neck pain during their lifetime [1,2]. One of the causes of neck pain is disk degeneration, known commonly as cervical spondylosis. Cervical spondylosis is observable in over half of the middle-aged population [3], but most cases are asymptomatic. Radicular symptoms, including arm pain, may only occur when changes to the disk materialize, which result in impingement of the cervical nerve roots. For example, disks herniation, osteophyte formation, or hypertrophied ligaments may cause cervical nerve root compression and consequent radiculopathy [3]. Initial treatment for neck pain and associated radiculopathy should be non-operative, even if there is neurological involvement. Surgery should only be considered when a patient is unresponsive to non-operative management, or if there is a sudden progressive neurological deficit requiring immediate intervention [4].
Anterior cervical discectomy with fusion is an accepted procedure for patients when there is neurological deficit. However, surgery is not indicated when there is no definite and objective clinical evidence of neurological deficit, and imaging studies do not show spinal cord compression or cervical nerve root impingement. However, even the results from imaging studies may result in incorrect indications. One issue regarding imaging studies used in the diagnosis of nerve root compression is the over sensitivity of a magnetic resonance imaging (MRI) scan. MRIs are not reliable to assess nerve root tension and often overestimate disk pathology [5]. This may result in non-clinically significant changes being highlighted as targets for surgical intervention. In addition, common radicular symptoms are often similar to symptoms that arise from shoulder pathology. A 2020 review of shoulder and cervical spine pathology reported that 15% of cervical spondylosis patients are ultimately diagnosed with a shoulder disorder [6]. Hence, shoulder and cervical spine pathologies can often overlap and be easily confused. It is therefore imperative that, when diagnosing a patient with radiculopathy, pathology of the shoulder is considered and ruled out [7].
History
We present the case of a 41-year-old male groundwork construction worker who, before February 2017, developed numbness and pins and needles in both arms, starting at the elbow and extending down the forearm and into all fingers. The general practitioner initially suggested non-operative management. The patient was reviewed again in April 2018. Due to non-relief of symptoms, an MRI scan was requested, and the patient was referred for a neurosurgical opinion.
Investigations
An MRI scan performed in June 2018 showed a disk osteophyte complex at both C3/4 and C5/6 (Fig. 1). The development of osteophytes at both locations caused mild narrowing of the lateral recess and mild spinal canal encroachment. However, there was no compression of the nerve roots or spinal cord identified at either location, and the report concluded that the cervical spinal cord appeared normal. Unfortunately, the newly recommended arm squeeze test, used to distinguish cervical nerve root compression from shoulder pathology, was not conducted. Considering the length of symptoms, the neurosurgeon recommended that the patient undergo an anterior cervical discectomy and fusion.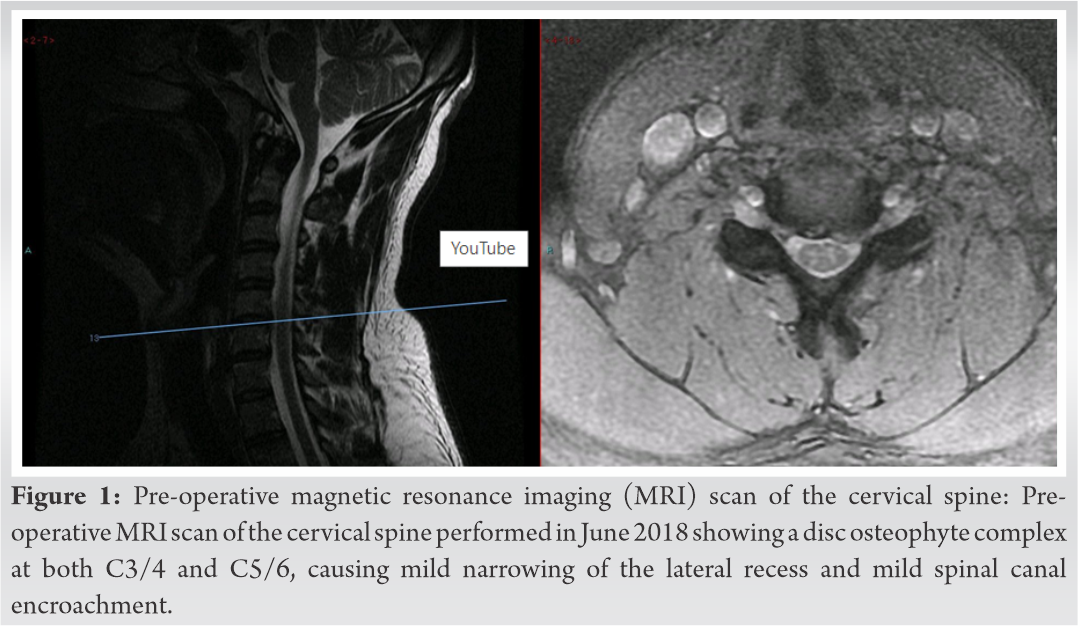
Intervention
The patient underwent a C5/6 anterior cervical discectomy and fusion in September 2018, as visible on a post-operative X-ray performed in June 2019 (Fig. 2).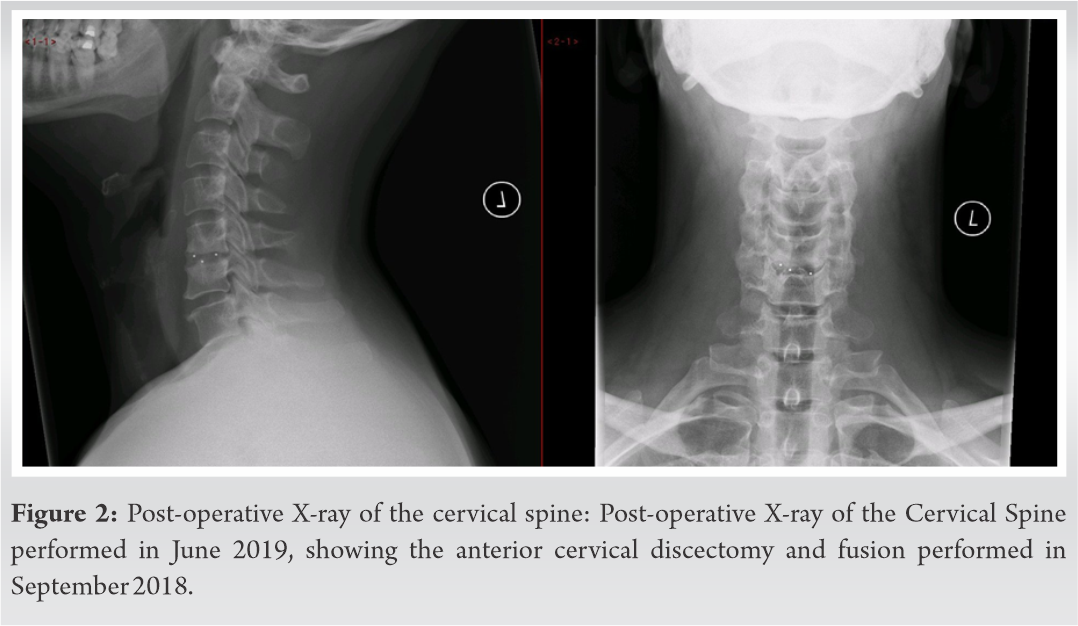
Outcome and follow-up
Unfortunately, following surgery, the patient continues to experience severe neck and shoulder pain. The range of motion in his neck and both shoulders is limited to around 50%. According to the patient’s statement, his symptoms have only worsened since the surgery, and he has been unable to work since February 2019 due to his ongoing issues. Post-operative clinical review found that the symptoms may be arising from shoulder pathology and not from the neck as first assumed. The patient is currently undergoing non-surgical shoulder rehabilitation.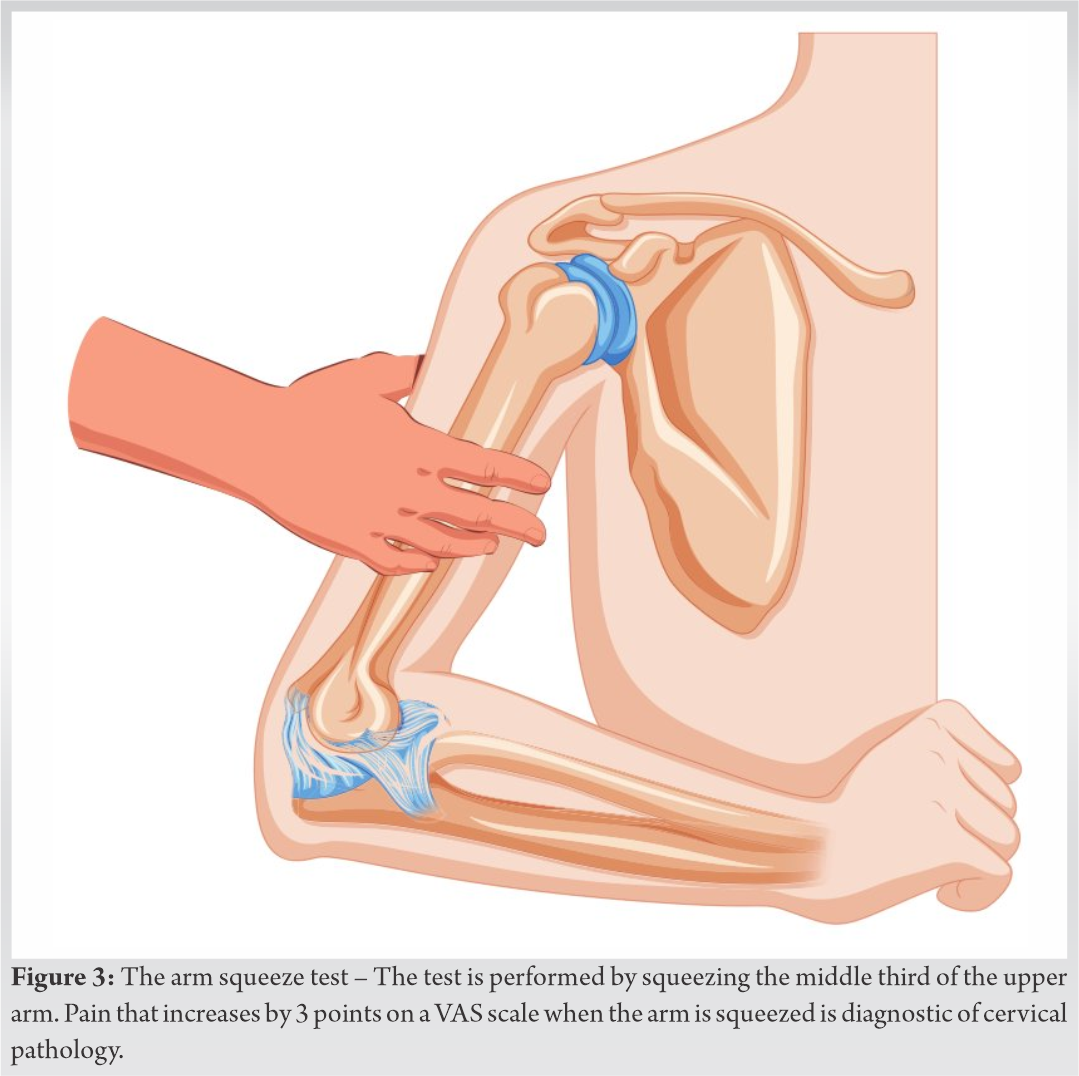
In clinical practice, outcomes from operations are not always consistent, and all procedures come with some degree of risk. The most effective solution in reducing poor outcomes and surgical risks is to avoid unnecessary surgical treatment [8]. Unnecessary surgery has been defined as a surgical intervention which is not required, indicated, or in the patient’s best interest when weighed against the potential outcomes of other, conservative measures [8]. Unfortunately, a significant number of surgeries that are performed worldwide may be unnecessary. This is especially so with regard to cervical surgeries, given that the benefits of surgery over conservative care for neck pain have not been clearly demonstrated within the literature [9]. Despite this, it has been reported that, between 1997 and 2012, the rate of cervical spinal fusions increased by 114% [10]. As a result of this unexplained increase in procedures, patients, hospitals, insurance companies, and surgeons are now all questioning whether some spinal operations are “unnecessary” [11]. A 2013 study by Epstein investigated the frequency at which people are recommended for an unnecessary spinal surgical procedure. They found that 60.7% of patients were told that they required an unnecessary surgical procedure, and 33.3% of patients were advised to undergo the wrong surgery. Only 11% were told that they needed the proper indicated procedure [11]. An issue with the diagnosis of cervical spine conditions, which may contribute to unnecessary surgery, is that an MRI scan can be too sensitive and may highlight non-clinically significant findings as reasons for surgery. Previously, issues with MRI scans regarding nerve root tension and the measurement of disk conditions have been reported [5]. This was evident in asymptomatic patients who were diagnosed with a disk herniation, showing the over sensitivity of the imaging technique [12]. Such findings indicate the importance of other tests, not just imaging techniques, in the diagnosis of shoulder and cervical spine pathologies. The importance of distinguishing shoulder and cervical spine pathologies is amplified when considering that they can result in similar symptoms. Such similarities often cause the pathologies to be confused with one another [6]. For instance, one study previously reported that 15% of cervical spondylosis patients were misdiagnosed and later received treatment for a shoulder condition [6]. It is, therefore, important that all relevant testing is conducted before a decision is made concerning the need for surgery. Pre-operative tests, such as Spurling’s test and the arm squeeze test, can be carried out to ensure that a correct diagnosis is made. Spurling’s test is a well-known and widely-used provocative test for the assessment of cervical radiculopathy. The test was originally described as passive lateral flexion and compression of the head, but the technique has since been updated. Typically, Spurling’s test is now defined as the passive cervical extension with rotation to the affected side and axial compression [13]. The test aims to distinguish cervical radiculopathy by reproducing symptoms through compression of the affected nerve root. Cervical extension reproduces posterior bulging of the intervertebral disk, while rotation of the head causes narrowing of the cervical neuroforamina. Application of axial compression augments these effects to amplify any pre-existing nerve root compression. If radicular pain that radiates to the shoulder or upper extremity is reproduced, the test is considered positive, and cervical radiculopathy can be established [13]. However, the previous research has demonstrated that the Spurling’s test has high specificity but low-to-moderate sensitivity [14], indicating the need for a more sensitive alternative. The arm squeeze test is a simple, quick, and useful method of assessment, helping to differentiate between shoulder and neck pathologies. The test is performed by squeezing the middle third of the upper arm on the side, where the shoulder pain is reported. It is theorized that, in cervical nerve root compression from C5 to T1, the pain will radiate along the nerves in the arm. In the middle third of the upper arm, the musculocutaneous nerve (cervical root from C5 to C7), the radial nerve (C5 to T1), the ulnar nerve (C7 to T1), and the median nerve (C5 to T1) are located fairly superficially. Hence, moderate squeezing of the cutis, subcutis, and bicep/tricep muscles will cause a slight tension on these nerves and will elicit a localized painful response in patients with cervical nerve root compression from C5 to T1, but not when the pain comes from shoulder pathology. Pain that increases by 3 points on a VAS scale when the arm is squeezed is diagnostic of cervical pathology (Fig. 3) [15]. A study involving 1567 patients found that the arm squeeze test positively identified nerve root compression 96.7% of the time, demonstrating high sensitivity [15]. These findings show that the test has good sensitivity and is a reliable diagnostic tool to distinguish between cervical and shoulder pathology. Hence, the technique is recommended by the National Institute for Health and Care Excellence [4]. However, the arm squeeze test is not well-known or popular, as it has only been identified recently. Therefore, attempts should be made to raise awareness of its existence.
Anterior Cervical Discectomy and Fusion is a usually successful procedure for people who require it. However, shoulder and cervical spine pathologies have similar symptoms and can be mistakenly diagnosed, potentially leading to unnecessary surgical intervention. The arm squeeze test is a simple examination procedure that helps to differentiate between neck and shoulder pathology. The test has a sensitivity of 0.96 and a specificity ranging between 0.91 and 1. Implementing this test during both shoulder and cervical spine examinations should become routine.
Coming to the correct diagnosis preoperatively is crucial to provide the best outcomes and prevent needless surgical interventions. Accordingly, recommended pre-operative tests, namely, the arm squeeze test due to its high sensitivity, should be used routinely during cervical and shoulder examinations.
References
- 1.Turk O, Yaldiz C. Spontaneous regression of cervical discs: Retrospective analysis of 14 cases. Medicine (Baltimore) 2019;98:e14521. [Google Scholar | PubMed]
- 2.Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population. Eur Spine J 2006;15:834-48. [Google Scholar | PubMed]
- 3.Kuo DT, Tadi P. Cervical spondylosis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551557 [Last accessed on 2021 Sep 29]. [Google Scholar | PubMed]
- 4.Neck Pain-cervical Radiculopathy: Scenario: Management. National Institute for Health and Care Excellence; 2018. Available from: https://www.cks.nice.org.uk/topics/neck-pain-cervical-radiculopathy/management/management [Last accessed on 2021 Sep 16]. [Google Scholar | PubMed]
- 5.Shah S, Ripple Shah DD, Magdum PB, Gajjar S. Observational study of various spinal disorders regarding correlation of radiological and clinical parameters. Int J Orthop 2017;3:600-10. [Google Scholar | PubMed]
- 6.Katsuura Y, Bruce J, Taylor S, Gullota L, Kim HJ. Overlapping, masquerading, and causative cervical spine and shoulder pathology: A systematic review. Global Spine J 2020;10:195-208. [Google Scholar | PubMed]
- 7.Iyer S, Kim HJ. Cervical radiculopathy. Curr Rev Musculoskelet Med 2016;9:272-80. [Google Scholar | PubMed]
- 8.Stahel PF, VanderHeiden TF, Kim FJ. Why do surgeons continue to perform unnecessary surgery? Patient Saf Surg 2017;11:1. [Google Scholar | PubMed]
- 9.Tayade MC, Dalvi SD. Fundamental ethical issues in unnecessary surgical procedures. J Clin Diagn Res 2016;10:JE01-4. [Google Scholar | PubMed]
- 10.Salzmann SN, Derman PB, Lampe LP, Kueper J, Pan TJ, Yang J, et al. Cervical spinal fusion: 16-year trends in epidemiology, indications, and in-hospital outcomes by surgical approach. World Neurosurg 2018;113:e280-95. [Google Scholar | PubMed]
- 11.Epstein NE. Are recommended spine operations either unnecessary or too complex? Evidence from second opinions. Surg Neurol Int 2013;4:S353-8. [Google Scholar | PubMed]
- 12.Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 1990;72:403-8. [Google Scholar | PubMed]
- 13.Jones SJ, Miller JM. Spurling test. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493152/# [Last accessed on 2021 Aug 11]. [Google Scholar | PubMed]
- 14.Rubinstein SM, Pool JJ, van Tulder MW, Riphagen II, de Vet HC. A systematic review of the diagnostic accuracy of provocative tests of the neck for diagnosing cervical radiculopathy. Eur Spine J 2007;16:307-19. [Google Scholar | PubMed]
- 15.Gumina S, Carbone S, Albino P, Gurzi M, Postacchini F. Arm squeeze test: A new clinical test to distinguish neck from shoulder pain. Eur Spine J 2013;22:1558-63. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report January 28, 2015 Technical note on Modified Posterior Approach to the Hip Joint
January 28, 2015 Technical note on Modified Posterior Approach to the Hip Joint May 10, 2022 Fibrous Dysplasia of Radius Bone-excision and Fibula Graft: A Case Report
May 10, 2022 Fibrous Dysplasia of Radius Bone-excision and Fibula Graft: A Case Report October 10, 2015 A Rare Case of Progressive Gorham’s Disease of Right Shoulder Girdle and Cervical Spine in A Child: 10 Year Follow-up and A Review of Literature
October 10, 2015 A Rare Case of Progressive Gorham’s Disease of Right Shoulder Girdle and Cervical Spine in A Child: 10 Year Follow-up and A Review of Literature