
Fascia lata is a readily available autograft which makes it a good choice for anterior capsule reconstruction and knotless fibretak anchors ease your surgery during graft pulling.
Dr. Hari Krishna Yadoji, Department of Arthroscopy and Shoulder Surgery, Sunshine Hospital, Secunderabad - 500 003, Telangana, India. E-mail: drharry2807@gmail.com
Abstract
Introduction: Shoulder has multidirectional mobility with capsule and rotator cuff as stabilizers. Irreparable subscapularis tears are relatively uncommon. Anterior capsule reconstruction (ACR) is one of the different modalities of treatment for irreparable subscapularis tears. Anterior capsular reconstruction can be performed using hamstring autograft, tibialis anterior allograft, and human dermal allograft. Procedures using hamstring autograft and tibialis anterior allograft reported severe capsular deficiency, recurrent dislocation, and subluxations. Dermal allograft is routinely used for ACR anterior capsule reconstruction. But However, there are no reports of Fascia lata autograft being used for ACR anterior capsule reconstruction. As fascia lata is an autograft, it may have a better chance of healing than dermal allograft.
Case Report: A 60-year year-old male patient came with history of slip and fall at home 3 months ago and injured his left shoulder. Magnetic resonance imaging MRI is showing subscapularis tear retracted medial to glenoid and anterior supraspinatus tear with minimal retraction. The aim of this case report is to describe in detail the arthroscopic technique of ACR anterior capsule reconstruction using fascia lata autograft using the new knotless all suture anchors (fibereTak) on glenoid.
Conclusion: Fascia lata being an autograft may have better healing potential, but its superiority over dermal allografts in the setting of ACR anterior capsule reconstruction needs further studies.
Keywords: Anterior capsule reconstruction, irreparable subscapularis, fascia lata, knotless fibereTak.
Shoulder has a multidirectional mobility with wide range of motion. The capsule and rotator cuff are the static and dynamic stabilizers of the shoulder joint, respectively. In the literature, incidence of isolated subscapularis tear accounts to only 5 % of rotator cuff tears [1]. Hence, encountering an irreparable subscapularis tear is uncommon. There are different modalities of treatment described for irreparable subscapularis tear such as tendon transfers and anterior capsule reconstruction (ACR). Tendon transfers are non-anatomic approaches altering the native biomechanics and reported significant retear rates, poor outcomes, and complications including musculocutaneous and axillary nerve injury [2-, 3, 4].
ACRAnterior capsule reconstruction has been described as a treatment for irreparable subscapularis tear using different grafts. Studies on anterior capsular reconstruction using hamstring autograft and tibialis anterior allograft reported severe capsular deficiency, recurrent dislocation, and subluxations [5]. In the literature, there are previous reports, where human allografts like such as acellular dermal and autografts like fascia lata have been used for superior capsular reconstruction or augmentation procedures in the context of massive rotator cuff tears and have produced promising early results [6]. Studies show that fascia lata is superior to dermal graft [7,8] and we have experience in using fascia lata for arthroscopic superior capsule reconstruction at our center and hence, we chose fascia lata as the graft of choice in our patient.
Adam et al. [9], in their surgical technique, described the arthroscopic ACRanterior capsule reconstruction using acellular dermal allograft and sutureTak anchors which work on the principle of double pulley. In our case, we have used fibereTak instead of sutureTak which is a new knotless all suture anchor. The aim of this case report is to describe in detail the arthroscopic technique of ACRanterior capsule reconstruction using fascia lata autograft using the new knotless all suture anchors (fibereTak) on glenoid and its functional outcome in a 1 year post- operative case of ACR anterior capsule reconstruction. A 60-year year-old male patient came with history of slip and fall at home 3 months ago and injured his left shoulder. Magnetic resonance imaging MRI is showing subscapularis tear retracted medial to glenoid as in (Fig. 1) and anterior supraspinatus tear with minimal retraction. The muscle atrophy is grade Grade 1 in supraspinatus and grade Grade 3 in subscapularis. We have planned for an arthroscopic ACR anterior capsule reconstruction with fascia lata autograft using new knotless suture anchors (fibereTak) for graft fixation.
Anaesthesia and Patient patient positioning:
General anaesthesia and a regional interscalene block is are given for left shoulder. On physical examination under anaesthesia, the side-to-side difference in passive external rotation found to be around 20°0 and a load & and shift for instability showed anterior subluxation. The patient is placed in the beach-chair position with the left shoulder and ipsilateral thigh prepared in anticipation of harvesting fascia lata and draped by sterile techniques.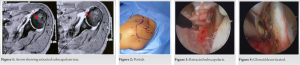
A diagnostic arthroscopy:
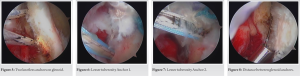
After establishing a standard posterior viewing portal which is 2 cm inferior and 1 cm medial from the posterolateral corner of acromion and a standard anteroinferior working portal through the rotator interval which is is inferolateral to the the tip of coracoid process as in (Fig. 2) using outside in technique with 18- guage Guage spinal needle. A diagnostic arthroscopy was performed. The capsulolabral complex, rotator cuff, anterior glenoid rim, articular cartilage, long head of the biceps tendon, and biceps-labral complex were thoroughly evaluated. Articular cartilage was normal. The long head of biceps found to be subluxed from bicipital groove with fraying, a biceps tenotomy is performed from its origin at the glenoid. The rotator cuff is carefully examined which showed a retracted subscapularis tear, as shown in (Fig. 3). Despite all the possible releases, only a small portion of upper subscapularis along with comma tissue is reaching the medial edge of subscapularis footprint on lesser tuberosity. The Patient patient has also got a full- thickness supraspinatus tear with minimal retraction. We decided to proceed for ACR anterior capsule reconstruction as subscapularis found to be irreparable. Additional portals like anterolateral which is 2 cm lateral and posterior to anterolateral corner of acromion, posterolateral which lies 2 cm lateral, and 2 cm anterior from the posterolateral corner of acromion are made using outside in technique. Portals for drilling of humerus anchor for supraspinatus are made separately by outside in technique.
Glenoid:
With anterolateral portal as viewing portal and anteroinferior portal as working portal, glenoid anterior surface is decorticated with a burr, as shown in (Fig. 4) and curetted for bleeding bony surface preserving the anterior labrum. Two knotless all suture anchors (arthrex – fibereTak 1.8mm) were drilled on anterior glenoid, one at 2.30’ o clock and other at 4.30 ’ o clock positions as in (Fig. 5).
Humerus:
We planned for a single row fixation on humerus. With anterolateral portal as viewing portal and anteroinferior portal as working portal, the subscapularis footprint on lesser tuberosity is decorticated and curetted. Two all suture anchors (conmed – Y Knot RC 2.8 mm) are deployed on the superior and inferior aspect, in the middle of subscapularis footprint as in (Fig. 6, 7).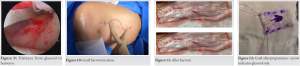
Graft measurements:
With anterolateral portal as viewing portal and anteroinferior portal as working portal, the distance between glenoid anchors is measured to be 10 mm, as shown in (Fig. 8) and between lesser tuberosity anchors is 15 mm. The distance between superior anchors of glenoid & and humerus is 30 mm, as shown in (Fig. 9). The distance between inferior anchors of glenoid and humerus is 27 mm. We added 5 mm to the above measurements on all sides to have better coverage of graft. From ipsilateral thigh an S- shaped incision is given, as shown in (Fig. 10) and fascia lata graft (3×18 cm) is harvested, as shown in (Fig. 11). Graft was prepared (20x40x25x37 mm). Traction sutures with 2-–0 vicryl are passed at lateral corners of the graft to keep graft in tension during graft passage, as shwon in (Fig. 12).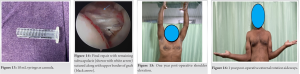
Graft passage:
A 10 ml syringe is cut at the tip and used as cannula in the anteroinferior portal (interval portal) for the graft to pass, as shown in (Fig. 13). With anterolateral portal as viewing portal and anteroinferior portal as working portal, one tying suture from each glenoid anchor are is brought out from interval portal and shuttled at about 5 mm from medial edge of the graft (one suture at each end) in inverted mattress configuration. This suture is now loaded into the pulling suture. As the pulling suture of each anchor are is pulled, the graft gets pulled into the joint towards glenoid. To avoid twisting of graft, we held the tailing end of graft with a grasper until the graft is intra-articular. The suture from each fibere Tak is pulled until graft is securely fixed on the glenoid which is confirmed arthroscopically.
Fixing to Lesser lesser tuberosity:
With posterior portal as viewing portal and anterolateral portal as working portal, sutures from Lesser lesser tuberosity anchors are shuttled through lateral edge of the graft using an accupass in mattress configuration, ; in addition, a suture from the superior anchor was shuttled through remnant superior subscapularis and knots are tied with graft in adequate tension and shoulder in 30°0 abduction, slight external rotation, and forward elevation. Supraspinatus was repaired arthroscopically to the greater tuberosity with two double -loaded all suture anchors. Final repair was checked as in Fig. 14. Acromioplasty is performed. Portals are closed with 2-0 ethilon.
Post-operative rehabilitation: the patient was put in a 30°0 abduction + 15°0 external rotation brace and was allowed to do active elbow, wrist, and hand movements. No movements were allowed in shoulder for 4 weeks. From 5th -to 6th week, passive shoulder ROM slowly progressing to full range. From 7th week, active assisted ROM slowly progressing to full range, scapular stabilising stabilizing exercise, and isometric cuff strengthening was started. From 13 week along with above exercises, theraband strengthening was advised. Lifting weights up to 5 kgs was were allowed after 6 months post-operative. At 1 year follow -up, the patient is having full range of forward and lateral elevation and active external rotation sideways (ERS) is 0-70, as shown in (Fig.15, 16). The Patient patient is able to perform all his routine activities by himself.
A functional subscapularis is vital for shoulder biomechanics and joint stability. The Literature literature shows different modalities of treatment, both non-anatomic and anatomic to reconstruct the anterior glenohumeral capsule and the subscapularis muscle for irreparable subscapularis tear. The results have varying rates of success and associated with high retear rates, and complications such as nerve injury. The Use use of dermal and fascia lata grafts in superior capsule reconstruction have has increased in recent times. They are of superior mechanical strength than tendon grafts, which are smaller, thinner, and more prone to tearing [7,8]. Open and arthroscopic ACRanterior capsule reconstruction with dermal allograft has been described earlier [9,10]. In a systematic review by Clara et al. [8] comparing fascia lata autograft versus human dermal allograft in arthroscopic superior capsular reconstruction for irreparable rotator cuff Tearstears, the graft tear rate reported in studies using fascia lata autograft ranged from 5% to 32%, whereas the values reported in studies using human dermal allograft ranged from 20% to 75%. Arthroscopic superior capsule reconstruction using fascia lata autograft is routinely done in our hospital, we applied the same technique for arthroscopic ACRanterior capsule reconstruction with fascia lata autograft which is the first ever in literature. The purpose of this case report is to emphasizse.
• the The use of knotless fibereTak on glenoid – the advantages are (a) small size of anchor, i.ethat is, 1.8 mm makes it easy to deploy on difficult sites with smaller surface areas like glenoid, (b) easy to pass the graft into joint, (c) secure fixation on glenoid, and (d) time saving, as there is no need of tying knots.
• if If sutures from both glenoid & and humerus anchors are passed through graft at once outside the shoulder before pulling the graft inside, there is a risk of suture entanglement. We can avoid this by passing only glenoid anchor sutures first and pull the graft into joint.
• Dermal allografts are not easily available in all countries, especially in developing countries like India. Fascia lata autograft is easily available and as it is an autograft the outcome can be better than allograft.
• when compared to open ACRanterior capsule reconstruction, arthroscopic ACRanterior capsule reconstruction has the advantage of dealing with any other concomitant pathologies apart from subscapularis tear like a supraspinatus tear in our case.
• Our patient achieved good functional outcome with ACRanterior capsule reconstruction using fascia lata, but we need further large scale studies to emphasise emphasize ACR with fascia lata as treatment of choice for irreparable subscapularis tear.
ACRAnterior capsule reconstruction is a treatment option for irreparable subscapularis tear. We have used the new knotless anchors (fibereTak) on the glenoid with the merits of easy passage of graft, knotless fixation, and firm fixation. Fascia lata being an autograft may have better healing potential, but its superiority over dermal allografts in the setting of ACRanterior capsule reconstruction needs further studies. Unlike open ACRanterior capsule reconstruction, arthroscopic ACRanterior capsule reconstruction gives the advantage of dealing with any other co-existing pathologies at the same time.
ACRAnterior capsule reconstruction is a challenging procedure and use of knotless fibereTak reduces the difficulty in passage of graft. Fascia lata autograft is easily available and may have better potential of healing than allografts.
References
- 1.Jermolajevas V, Kemzuraitė N. Subscapularis tendon tears: Solutions for reparable and irreparable tears. Issue Rehabil Orthop Neurophysiol Sport Promot 2016;15:31-8. [Google Scholar | PubMed]
- 2.Gavriilidis I, Kircher J, Magosch P, Lichtenberg S, Habermeyer P. Pectoralis major transfer for the treatment of irreparable anterosuperior rotator cuff tears. Int Orthop 2010;34:689-94. [Google Scholar | PubMed]
- 3.Elhassan B, Christensen TJ, Wagner ER. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: An anatomic study. J Shoulder Elbow Surg 2014;23:492-9. [Google Scholar | PubMed]
- 4.Shin JJ, Saccomanno MF, Cole BJ, Romeo AA, Nicholson GP, Verma NN. Pectoralis major transfer for treatment of irreparable subscapularis tear: A systematic review. Knee Surg Sports Traumatol Arthrosc 2016;24:1951-60. [Google Scholar | PubMed]
- 5.Alcid JG, Powell SE, Tibone JE. Revision anterior capsular shoulder stabilization using hamstring tendon autograft and tibialis tendon allograft reinforcement: Minimum two year follow-up. J Shoulder Elbow Surg 2007;16:268-72. [Google Scholar | PubMed]
- 6.Mihata T, Lee TQ, Watanabe C, Fukunishi K, Ohue M, Tsujimura T, et al. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy 2013;29:459-70. [Google Scholar | PubMed]
- 7.Mihata T, Bui CN, Akeda M, Cavagnaro MA, Kuenzler M, Peterson AB, et al. A biomechanical cadaveric study comparing superior capsule reconstruction using fascia lata allograft with human dermal allograft for irreparable rotator cuff tear. J Shoulder Elbow Surg 2017;26:2158-66. [Google Scholar | PubMed]
- 8.Azevedo CI, Andrade R, Ângelo AC, Espregueira-Mendes J, Ferreira N, Sevivas N. Fascia lata autograft versus human dermal allograft in arthroscopic superior capsular reconstruction for irreparable rotator cuff tears: A systematic review of clinical outcomes. Arthroscopy 2020;36:579-91.e2. [Google Scholar | PubMed]
- 9.Kwapisz A, Tokish JM. Anterior capsule reconstruction technique with an acellular dermal allograft. Arthrosc Tech 2017;6:e1945-52. [Google Scholar | PubMed]
- 10.Pogorzelski J, Hussain ZB, Lebus GF, Fritz EM, Millett PJ. Anterior capsular reconstruction for irreparable subscapularis tears. Arthrosc Tech 2017;6:e951-8. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 7, 2014 Scalloping Sacral Arachnoid Cyst as a Cause of Perianal Pain- A Case Report
April 7, 2014 Scalloping Sacral Arachnoid Cyst as a Cause of Perianal Pain- A Case Report June 1, 2025 Giant Cell Tumor of the Proximal Femur with Pathological Fracture of Femoral neck
June 1, 2025 Giant Cell Tumor of the Proximal Femur with Pathological Fracture of Femoral neck March 10, 2023 Bilateral Knee Septic Arthritis after Prostatic Urethral Lift: A Case Report
March 10, 2023 Bilateral Knee Septic Arthritis after Prostatic Urethral Lift: A Case Report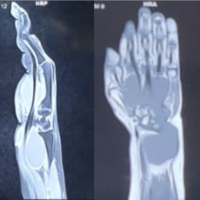 April 10, 2022 Tubercular Tenosynovitis Mimicking a Large Ganglion Cyst
April 10, 2022 Tubercular Tenosynovitis Mimicking a Large Ganglion Cyst