
Greater angulated radial neck fracture (180°) can successfully be treated with good radiological and functional outcome with open reduction and K wire fixation and patient should be explained about risk of avascular necrosis of head of radius and growth arrest.
Dr. Sheel Sunil Chhajed, Vinayaka Misssion Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India. E-mail: sheelchhajed@gmail.com
Introduction: 180 °rotated and displaced fracture neck of radius with displacement is rare case in pediatric age as the cartilaginous head absorbs the force and transmits it to the weaker physis or metaphysis of the neck. These fractures characteristically produce an angular deformity of the head with the neck.
Case Report: This case report describes a rare case of 180° rotated and displaced fracture neck of radius with displacement. A 12-year-old female presented to OPD with history of self-fall over right elbow while playing and started complaining of pain over right elbow for about 2 h. She underwent open reduction internal fixation with k wire fixation procedures. She made an uneventful recovery and reported full range of motion after a follow-up of 3 months.
Conclusion: The best treatment options in pediatric age suffering from a displaced (Judet classification type 4b) radial neck fracture with displacement in childhood is open reduction and fixation of fracture to avoid further joint stiffness and growth related deformity.
Keywords: 180° Rotation, fracture neck of radius, displacement.
Most fractures of the proximal radius occur at the neck and after a fall on an outstretched arm with elbow extended. The immature radial head is primarily cartilaginous and ossifies around 10 years of age. Intra-articular radial head fractures in children and adolescents are rare and constitute around 1% of all fractures [1, 2, 3, 4]. The cartilaginous head absorbs the force and transmits it to the weaker physis or metaphysis of the neck. These fractures characteristically produce an angular deformity of the head with the neck [1, 2, 3, 4, 5, 6, 7]. The direction of angulation depends on whether the forearm is in a supinated, neutral, or pronated position at the time of the fall. In neutral position, the pressure is concentrated on the lateral portion of the head-and-neck. In supination, the pressure is concentrated anteriorly, and in pronation it is concentrated posteriorly. Proximal radial fractures also may occur in association with elbow dislocation. The fracture will occur either during the dislocation event, typically when displaced anterior. Alternatively, the fracture may occur during spontaneous reduction of the distal humerus, driving the displacement of the proximal radius posterior. Hence, in this present study, we are presenting a case review of rare (180°) angulated radial neck fracture with the review of literature.
A 12-year-oldgirl presented to OPD after a fall over right elbow while playing at home with pain and limitation of movements. On examination, we observed that pain aggravates on movement and there was tenderness over head of radius and it was aggravating on supination and pronation of forearm. We have also noted mild swelling over tender extremity. Range of motion was limited and painful in supination and pronation, flexion and extension with active finger movement, and distal pulse present. There was no distal neurovascular deficit. following which X-ray was taken and she was diagnosed with displaced fracture neck of Right (JUDET TYPE IV b CLASSIFICATION as shown in Fig. 1).
As closed reduction for Judet Type IV b always fails to reduce and it is important to achieve complete reduction as with mild angulation of radial head may lead to restriction of movement of the elbow joint, patient was planned for open reduction internal fixation with k wire/tens nailing right radius. Patient was placed in supine position. Under general anesthesia closed manipulation technique was tried as described by Patterson as given in (Fig. 2). An assistant was holding the arm proximally, with one hand placed medially against the distal humerus, and straight longitudinal distal traction was applied. Then, varus force was applied to the forearm and digital pressure directly over the tilted radial head to complete the reduction. Forearm is held in 90° of flexion and in pronation.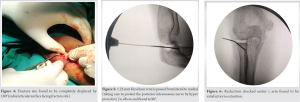
Reduction was found to be unsuccessful and elbow was found to be subluxating after closed reduction. Then open reduction was attempted. About 5 cm Incision(lateral kochers approach) made over lateral aspect of elbow joint. Skin, fascia, and subcutaneous tissue incised and retracted. Intramuscular plane identified between anconeus and extensor digitorium communis. After separating these two muscles radius, head was exposed as given in (Fig. 3). Fracture site found to be completely displaced by 180° (radial articular surface facing fracture site) as given in (Fig. 4). After removing interpositioned tissue, fracture site was freshened. After correcting anatomical reduction, the 1.25 mm Kirschner wire is passed from lateral to medial (taking care to protect the posterior interosseous nerve by hyper pronation) in elbow and flexed to 90° as shown in (Fig. 5). Reduction checked under c arm found to be satisfactory in flexion and extension (Fig. 6) of elbow and supination and pronation of forearm. Radiocapitellar line found to be intact throughout the range of motion. Thorough wound wash given. Wound closed in layers and sterile dressing done and above elbow slab applied. Immediate post-operative X-ray was taken and found to be satisfactory sequential monthly follow-up X-ray was taken and k wire was removed as shown in (Fig. 7). After 3-month postoperatively, she has good functional outcome of the right elbow joint as shown in (Fig. 8).
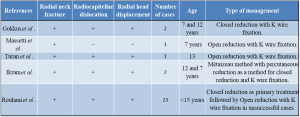
In this present review, 12-year-old girl with 180° angulated radial neck fracture case operated by open reduction and K wire internal fixation. The classification and treatment of these fractures depends on the angulation. Original and most widely used classification was given by the Judet as shown in (Fig. 9). According to this classification, Type 1 is non-displaced, Type 2 has <30° angulation, Type 3 has between 30°and 60°, and Type 4 has two sub-types. Type 4a has between 60°and 80° and Type 4b has >80° of angulation. Majed and Baco[8] reported a case report of closed reduction with intramedullary elastic nailing. They concluded that fixation with intramedullary wires is safe and effective even when the presentation is delayed. Bastard et al.[9] also observed similar finding, that is, greater displaced radial neck fractures best managed by open reduction but also reported that it could be associated with the loss of supination-pronation and other complication of open surgeries. In our case report, we did not observe any such complications. This may be due to intra-medullary nailing with K wire that is a minimally invasive, simple, and reproducible technique with a low rate of complication. Consistently, Pogorelić et al.[10] reported that use of flexible intra-medullary nailing for treating fractures of the radial neck in children shows very good functional and cosmetic results with early mobilization and rapid pain reduction. Rouhani et al.[11] in their study also reported that most patients accept the closed reduction as a primary method of treatment, but an open-reduction approach has been associated with optimal therapeutic outcomes for patients in whom closed reduction was not satisfactory or indicated.
Radial neck fracture of 180°,that is, Judet Type 4b (angulated>80°) fails to heal satisfactorily but can be treated with satisfactory results with open reduction and K wire fixation.
Greater angulated radial neck fracture (180°) can successfully be treated with good radiological and functional outcome with open reduction and K wire fixation and patient should be explained about risk of avascular necrosis of head of radius and growth arrest.
References
- 1.Watkins RG 4th, Chang D, Watkins RG 3rd. Return to play after anterior cervical discectomy and fusion in professional athletes. Orthop J Sports Med 2018;6:2325967118779672. [Google Scholar]
- 2.McAnany SJ, Overley S, Andelman S, Patterson DC, Cho SK, Qureshi S, et al. Return to play in elite contact athletes after anterior cervical discectomy and fusion: A meta-analysis. Global Spine J 2017;7:552-9. [Google Scholar]
- 3.Lindi-Sugino R, Hartl R, Klezl Z. Cervical arthroplasty in a professional kick-boxing fighter, 7 years follow-up. Acta Ortop Mex 2021;35:282-85. [Google Scholar]
- 4.Leider J, Piche JD, Khan M, Aleem I. Return-to-play outcomes in elite athletes after cervical spine surgery: A systematic review. Sports Health 2021;13:437-45. [Google Scholar]
- 5.Molinari RW, Pagarigan K, Dettori JR, Molinari R Jr, Dehaven KE. Return to play in athletes receiving cervical surgery: A systematic review. Global Spine J 2016;6:89-96. [Google Scholar]
- 6.Steinberger J, Qureshi S. Cervical disc replacement. Neurosurg Clin N Am 2020;31:73-9. [Google Scholar]
- 7.Xu S, Liang Y, Zhu Z, Qian Y, Liu H. Adjacent segment degeneration or disease after cervical total disc replacement: A meta-analysis of randomized controlled trials. J Orthop Surg Res 2018;13:244. [Google Scholar]
- 8.Badve SA, Nunley PD, Kurra S, Lavelle WF. Review of long-term outcomes of disc arthroplasty for symptomatic single level cervical degenerative disc disease. Expert Rev Med Devices 2018;15:205-17. [Google Scholar]
- 9.Mai HT, Chun DS, Schneider AD, Hecht AC, Maroon JC, Hsu WK. The difference in clinical outcomes after anterior cervical fusion, disk replacement, and foraminotomy in professional athletes. Clin Spine Surg 2018;31:E80-4. [Google Scholar]
- 10.Reinke A, Behr M, Preuss A, Villard J, Meyer B, Ringel F. Return to sports after cervical total disc replacement. World Neurosurg 2017;97:241-6. [Google Scholar]
- 11.Maroon JC, Bost JW, Petraglia AL, Lepere DB, Norwig J, Amann C, et al. Outcomes after anterior cervical discectomy and fusion in professional athletes. Neurosurgery 2013;73:103-12; discussion 112. [Google Scholar]






