
It highlights the importance of histopathological examination in diagnosis.
Dr. Samriti Goyal, Department of Pathology, Government Medical College and Hospital, Patiala, Punjab, India. E-mail: samritigoyal0505@gmail.com
Introduction: Cutaneous actinomycosis of popliteal fossa is quite unusual, chronic granulomatous disease caused by a group of anaerobic or microaerophilic Gram positive filamentous bacteria that colonize the mouth, colon, and urogenital tract. Actinomycosis of popliteal fossa is rare clinical condition; therefore, recognition of this entity needs high degree of suspicion as the organism is specific internal habitant; primary involvement of extremities is rare.
Case Report: This case report presents a rare case of actinomycosis of popliteal fossa (left side) in a 40-year-old male patient. The patient complained of presence of a mass with multiple pus oozing sinuses over popliteal fossa. The X-ray of leg revealed presence of foreign body. Histopathological examination of the biopsy from the lesions confirmed diagnosis of cutaneous actinomycosis.
Conclusion: Cutaneous actinomycosis is a disease with great diagnostic challenge and requires high degree of suspicion for the early diagnosis which avoids unnecessary surgery and decreased morbidity and mortality.
Keywords: Cutaneous Actinomycosis, Popliteal fossa, Sinuses, Histopathology.
Actinomycosis is a rare infection primarily caused by the Gram-positive, non-sporeforming, and anaerobic bacillus actinomyces. It is primarily a commensal microbe found in normal oral cavities, including tonsillar crypts, dental plaques, carious teeth, and female genital tract. Cutaneous actinomycosis of popliteal fossa is quite unusual. Most of the infection occurred after trauma that creates an anaerobic conditions predisposing to this microorganism and other bacterial infections. It is characterized by producing chronic granulomatous, suppurative lesions with abscesses, along with drainage sinuses and it easily spreads to adjacent structures and organs. Due to the exclusively endogenous habitat of the etiologic agent, head and neck, thorax, and abdomen are the sites that commonly involved and popliteal fossa involvement is rare [1]. Males have a threefold higher incidence than females, possibly due to poorer dental hygiene and/or more frequent trauma. In vivo growth of actinomycetes usually results in the formation of characteristic clumps called grains or sulfur granules [2]. Actinomycosis of popliteal fossa is rare clinical condition; therefore, recognition of this entity needs high degree of suspicion as the organism is specific internal habitant, primary involvement of extremities is rare.
A 40-year-old male was admitted with a history of large mass with multiple pus oozing sinuses over left popliteal fossa since 3–4 years. The patient had past history of trauma due to explosion 13 years back which was healed spontaneously. The patient came to Out Patient Department, Rajindra hospital for treatment purpose as he noticed swelling with formation of pus oozing sinus over the same region. Swelling was gradually increasing with formation of multiple pus oozing sinuses (Fig. 1).
On examination – Vital signs were normal with no palpable lymphadenopathy. Various investigations were carried out. All hematological and biochemical investigation were in normal range. There was no palpable lymphadenopathy. The X-ray of leg revealed presence of small foreign body in popliteal fossa (Fig. 2). Then patient was advised for fine needle aspiration cytology (FNAC). FNAC of the mass was done and it showed inflammatory smear (Fig. 3).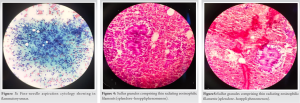
The patient underwent surgery of incision and debridement. The pus and gray-brown color material were drained out. Malignancy was considered as the provisional diagnosis by the surgeon. On histopathological examination, Hematoxylin and Eosin stained sections showed aggregates of sulfur granules comprising thin radiating eosinophilic filaments surrounded by a rim of strong eosinophilic amorphous material (splendore–hoeppli phenomenon) surrounded by inflammatory infiltration comprising lymphocytes, plasma cells, neutrophils, and hemosiderin-laden macrophages along with areas of necrosis (Figs. 4 and 5). Acid-fast stain was non-contributory, and thus, evidence of malignancy was ruled out. Final diagnosis was rendered. The patient responded well to surgery and further combined with course of antimicrobial treatment for actinomycosis. No further complications occurred.
Actinomycotic infection is an active chronic suppurative inflammatory process. It is caused by a group of anaerobic or microaerophilic bacteria that are commensal of vagina, large bowel, and oral cavity. The most frequent sites of involvement of actinomycosis are cervicofacial, thoracic, and abdominal among which cervicofacial is the most common type. The disease occurs worldwide and has no predilection for age race, season, or occupation but mainly occurs in the middle decades of life [2]. Cutaneous actinomycosis is an uncommon infection. The recognition of this entity needs high degree of suspicion, because the organism resides in internal habitant, the primary involvement of extremities is rare. Most of the cases reported give a clear history of trauma [1, 3]. Histopathological examination of the lesions helped to reach a final diagnosis. The filamentous organism usually needs a traumatized skin from injury or bites to inoculate and established anaerobic conditions to cause actinomycotic infection. Clinical features of the cutaneous lesion in primary infection resemble many other skin infections and it leads to a nonspecific clinical diagnosis. Its clinical presentation is usually indolent and has various manifestations, including nodular lesions, subcutaneous abscess, or even mass lesion mimicking tumor [4]. It produces manifestations that can be easily mistaken for metastatic disease, with multiple nodules in virtually any organ or tissue [5]. The other differential diagnoses are cutaneous tuberculosis, sporotrichosis, and nocardiosis, because all of them tend to form nodular lesions with fistulae. The symptoms include pain is rare and only mild fever occurs in over half of the patients. The imaging techniques include magnetic resonance imaging and computed tomography (CT) which usually yields nonspecific findings. In view of these non-specific manifestations and imaging findings, the clinical diagnosis of actinomycosis still remains difficult. There are no specific radiological features on ultrasound to aid the diagnosis. CT can be helpful in the presence of a contrast-enhancing multicystic lesion to approach biopsy [6]. Actinomycosis is identified by draining sinuses containing sulfur granules in the pus, histopathologically, the “sulfur granules” contains filamentous structures or club-shaped structures. These structures are Gram-positive but are negative with acid-fast staining [7]. The gold standard for diagnosis of actinomycotic infection is culture and isolation from clinical specimens. Surgical biopsy is necessary to obtain a tissue sample for a final diagnosis, especially when the cutaneous lesions have the features of abscess [8]. Histopathological examination of specimen is necessary for diagnosis of actinomycosis. Diagnosis is based on histopathological findings, because the cultures are positive in only 24% of cases [9]. After surgical treatment, oral penicillin therapy was started as the treatment of choice for actinomycosis, the patient responded well and was completely healed [10]. No further complications occurred, in spite of the local spread of disease in popliteal fossa region and the patient was cured with conservative therapy. In this case, the diagnosis of cutaneous actinomycotic infection was based on the microscopic examination of skin tissue with characteristic sulfur granules. The prognosis for treated infections is excellent if it is recognized early.
Cutaneous actinomycosis is a rare condition that presents with considerable diagnostic challenge requiring higher degree of suspiciousness for the early diagnosis, thereby avoiding unnecessary surgery and reduced morbidity and mortality. This case report highlights the importance of histopathological examination and clinical awareness to consider full spectrum of the disease.
This is quite a rare case of Cutaneous Actinomycosis of Popliteal Fossa. The aim of this report is to give the idea that the diagnosis of cutaneous actinomycotic infection is based on the histopathological examination of skin tissue with characteristic sulfur granules. The prognosis for treated infections is excellent if it is recognized early.
References
- 1.Gupta V, Jain P, Gupta G, Gupta S, Gill M, Singh S. Primary cutaneous actinomycosis of upper extremity masquerading as soft tissue neoplasm: A case report. Trop Doc 2012;42:58-9. [Google Scholar]
- 2.Russo TA.Actinomycosis. In: Longo DL, Kasper DL, Jameson JL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. Vol. 1. 8th ed. New York: McGraw Hill; 2012. [Google Scholar]
- 3.Yang CH. Primary cutaneous actinomycosis of an extremity, a case report. J Int Med Taiwan 2010;21:290-93. [Google Scholar]
- 4.Kumar A, Detrisac DA, Krecke CF, Jimenez MC. Actinomycosis of the thigh presenting as a soft-tissue neoplasm. J Infect 1991;23:187-90. [Google Scholar]
- 5.Malik A, Papagrigoriadis S, Leather A, Rennie J, Salisbury J, Beese R. Abdominopelvic mass secondary to Actinomyces israelii mimicking cancer: Report of two cases. Tech Coloproctol 2005;9:170-71. [Google Scholar]
- 6.Acevedo F, Baudrand R, Letelier LM, Gaete P. Actinomycosis: A great pretender. Case reports of unusual presentations and a review of the literature. Int J Infect Dis 2008;12:358-62. [Google Scholar]
- 7.Wee SH, Chang SN, Shim JY, Chun SL, Park WH. A case of primary cutaneous actinomycosis. J Dermatol 2000;27:651-4. [Google Scholar]
- 8.Prasad P, Bhardwaj M. Primary tuberculosis of tonsils: A case report. Case Rep Med 2012;2012:120382. [Google Scholar]
- 9.Golden N, Cohen H, Weissbrot J, Silverman S. Thoracic actinomycosis in childhood. Clin Pediatr 1985;24:646-50. [Google Scholar]
- 10.Reiner SL, Harrelson JM, Miller SE, Hill GB, Gallis HA. Primary actinomycosis of an extremity: A case report and review. Rev Infect Dis 1987;9:581-9. [Google Scholar]





