
Anticipation of need for quadriceps V-Y lengthening in a patella gap non-union is necessary to avoid on table struggles.
Dr. Pranay Kondewar, Department of Orthopaedics, Grant Govt. Medical College and JJ Hospital, Mumbai, Maharashtra, India. E-mail: pranaypk1@gmail.com
Introduction: The management of gap non-union patella fractures continues to be a challenge in orthopedics. The incidence of these cases ranges between 2.7% and 12.5%. The quadriceps muscle attached to the proximal fractured fragment pulls it proximally leading to the gap at fracture site. If the gap is too large, there won’t be any fibrous union resulting in failure of quadriceps mechanism and extension lag. The primary aim is to bring the fracture fragments together and restore the extensor mechanism. Most of the surgeons prefer single-stage procedure, in which mobilization of the proximal fragment, followed by fixing with the lower fragment is done using V-Y plasty or x lengthening with or without pie Crusting. Others use of pre-operative traction to the proximal fragment using pins or ilizarov method. In our case, we used single-stage procedure whose results were encouraging.
Case Report: A 60-year-old male patient presented with pain in the left knee with difficulty in walking since 3 months. The patient had road traffic accident 3 months back and sustained trauma to left knee. On clinical examination, there was palpable gap of more than 5 cm between the fracture fragments, anterior surface of femur and condyles was palpated through fracture site and knee range of motion was between 30° and 90° of flexion, and X-ray suggests of patella fracture. Midline 15 cm longitudinal incision was taken. The insertion of the quadriceps tendon over proximal pole of patella was exposed and pie crusting was done on medial and lateral side and V-Y plasty was done. SS wire was used to hold the reduction of the fragments by encirclage wiring and anterior tension band wiring done. Retinaculum was repaired and wound closed in layers. Postoperatively, long rigid knee brace was given for 2 weeks and walking with partial weight-bearing started. After suture removal at 2 weeks, full weight-bearing initiated. At 3 weeks, knee range of motion started and continued till 8 weeks. At 3 months post-operative, the patient is able to do flexion up to 90° and no extension lag is present.
Conclusion: Adequate quadriceps mobilization during the surgery along with pie crusting and V-Y plasty with TBW and encirclage combined gives good functional outcome in patella gap non-unions.
Keywords: V-Y quadriceps plasty, patella non-union, gap non-union, TBW, patella fractures.
The management of gap non-union patella fractures continues to be a challenge in orthopedic practice. There exists limited evidence in the literature to guide the clinician in the management of these complications. The incidence of these cases ranges between 2.7% and 12.5% [1]. Delayed presentation of displaced fracture of the patella is a common presentation in practice, but in most of the cases, fragments can be approximated easily when gap is <3 cm. In cases with very old injury, fragments are very much separated and another intervention in form of pre-operative traction using ilizarov frame or soft-tissue procedure may become necessary. Along with fracture, there are soft-tissue contractures involving quadriceps muscle, retinaculum, and internal ligaments of the knee joint, leading to joint stiffness. The quadriceps muscle attached to the proximal fractured fragment pulls it proximally leading to the gap at fracture site [2]. If the gap is too large, there won’t be any fibrous union resulting in failure of quadriceps mechanism and extension lag. The proximal fractured fragment can be retracted proximally in the distal thigh to various length. Non-union patella may be well tolerated by low functional demand patients but requires surgical intervention in active patients [3]. The Primary aim is to bring the fracture fragments together and restore the extensor mechanism. There are various options in terms of the management for such complex presentation. Earlier it was managed conservatively with knee ROM exercises and an extension lag was accepted. most of the surgeons prefer single-stage procedure, in which mobilization of the proximal fragment, followed by fixing with the lower fragment is done using V-Y plasty or x lengthening with or without pie Crusting [4], Others use of pre-operative traction to the proximal fragment using pins or ilizarov method to approximate the fragments and then fixing the fragments [5]. In our case, we used single-stage procedure whose results were encouraging.
A 60-year-old male patient presented with pain in the left knee with difficulty in walking since 3 months. The patient had road traffic accident 3 months back and sustained trauma to the left knee. The patient did not took any treatment for the same and came to hospital after 3 months of the injury. On clinical examination, there was palpable gap of more than 5 cm between the fracture fragments, anterior surface of femur and condyles were palpated through fracture site and knee range of motion was between 30° and 90° of flexion, and terminal 30° extension lag was present. On radiological examination in form of X-ray radiograph and CT scan with 3D reconstruction fracture, morphology delineated and gap of 5 cm was noted (Fig. 1, 2). 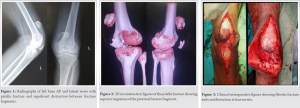
The patient was operated in supine position and tourniquet was not used (to avoid interference with quadriceps release). Midline 15 cm longitudinal incision was taken and medial and lateral flaps were raised. Fracture fragments were identified. Fracture ends were completed covered by the fibrotic tissue (Fig. 3). Fracture ends were freshened, there was a gap of 5 cm between the fragments in full extension of knee. The insertion of the quadriceps tendon over proximal pole of patella was exposed and pie crusting was done on medial and lateral side, but still fragments were not approximated, so quadriceps release was done from the anterior surface of femur and V-Y plasty was done. Three longitudinal tunnels were made in proximal and distal fracture fragments
and ethibond 5 was passed through it (Fig. 4).
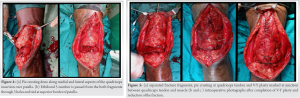
This helped to reduce the fracture gap and was later tied along superior border. For the V-Y plasty, the length of the limbs of the V of size double the length of the defect was taken, approximately 10 cm. The V shaped cut is marked at junction of tendon and muscle and partial thickness cut were made. The ends of V are then pulled down along with patella and fracture ends were approximated. SS wire was used to hold the reduction of the fragments by encirclage wiring and anterior tension band wiring done. The Y limb so formed after pulling of the tendon was sutured, and then, part of V was sutured back with the medial and lateral native quadriceps muscle tendon. Retinaculum was repaired and wound closed in layers (Fig. 5). Post-operative radiograph showed approximation of the fragment and reduction of articular surface (Fig. 6).
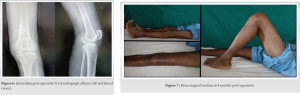
Postoperatively, long rigid knee brace was given for 2 weeks and walking with partial weight-bearing started. After suture removal at 2 weeks, full weight-bearing initiated. At 3 weeks, knee range of motion started and continued till 8 weeks. At 3 months post-operative, the patient is able to do flexion up to 90° and no extension lag is present (Fig. 7). There is bony union seen at 3 months follow-up.
All of cases of displaced fracture of the patella required operative intervention. If not operated, then the patients generally land up with a gap non-union due to ignorance as they walk full weight-bearing. The normal tensile force across a patella is around 3000 N, which increases up to 6000 N in athletes. The generated patellofemoral compressive forces are 3 times greater than that of the body weight during routine daily activities and may exceed 7 times the body weight while climbing stairs and squatting. These forces act on the proximal pole in fractures associated with tears in the medial and lateral retinaculum. The integrity of the medial and lateral expansions along with the anterior fascia lata and Sharpey’s fibers decides the degree of active extension of the knee after patellar fracture. Unopposed transfer of these forces leads to continuous increase in the gap between the fragments and contracture of the quadriceps [6]. In our case, we have measured the functional outcome in terms of knee range of motion gained after surgery and union of the patella fracture. The patient had gained full extension at 3 months post-operative and there is union at fracture site. A systematic review by Nathan et al. concluded that tension band wiring is the treatment of choice for patients with non-union of patella fracture. Partial or total patellectomy is also an option for small distal fragments or where satisfactory internal fixation cannot be achieved [7]. The problem faced by surgeons while treating neglected and displaced patellar fracture is the difficulty of bringing the fragments close to each other due to contracture of surrounding soft tissues. Various methods have been described to treat difficult patellar fractures such as (A) observation and conservative treatment in selected cases, (B) single-stage operative procedure to bring the fragments together by soft-tissue dissection, sometimes requiring V-Y plasty, and (C) some authors have suggested two stage treatment which consisted of preoperative traction to the proximal fragment by any means like Ilizarov ring fixator to approximate the fragments followed by internal fixation at a later date [8]. In a case Series published by Garg et al., 35 patients of non-union/delayed union of patella with significant gap and failure of quadriceps mechanism, which underwent three different methods surgically: (1) V-Y plasty and tension band wiring (n = 10); (2) patellar traction followed by tension band wiring without V-Y plasty (n = 15); and (3) patellar traction followed by partial or total patellectomy (n = 10). They compared the results in term of Knee Society Score, Melbourne patella score, showed that the 15 cases of patellar traction followed by tension band wiring showed the best results, cases with patellectomy showed the next best results, but they had a longer period of rehabilitation. V-Y plasty gave the least favorable outcome [9]. Another study by Uvaraj et al. compared tension band wiring to patellectomies in neglected fractures of the patella. Twenty-two patients were treated for neglected fractures of the patella, comprised 18 transverse, two comminuted, and two lower pole fractures, most of which had been treated by traditional methods initially. Treatment methods included tension band wiring in 16 cases, tension band wiring with cerclage in three cases and patellectomy in three cases. They noted that the function of the quadriceps after a patellectomy was significantly compromised. They reported a reduction of the efficiency of the extensor mechanism by about 30% [10].
Adequate quadriceps mobilization during the surgery along with pie crusting and V-Y plasty helps to approximate the fracture ends in gap non-union patella. TBW and encirclage gives stability to the construct till the healing of fractures, both of which combined gives good functional outcome in patella gap non unions.
Gap non-union patella fracture are managed well using encirclage wire and tension band wiring with quadriceps V-Y plasty.
References
- 1.Al-Obaedi O, Thakrar RR, Kundra R, Iqbal MJ. Gap non-union patella fractures: Case report and review of the literature. J Orthop Case Rep 2019;9:69-71. [Google Scholar]
- 2.Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma 1997;11:351-6. [Google Scholar]
- 3.Harna B, Gupta P, Singh J, Rousa S, Gupta A. Surgical management of non-union patella fracture: A case series and review of the literature. Arch Bone Jt Surg 2021;9:554-8. [Google Scholar]
- 4.Bhimani R, Singh P, Bhimani F. Double-tension wire management of nonunion patella with severe quadriceps contracture. Case Rep Orthop 2018;2018:1364129. [Google Scholar]
- 5.Baruah RK. Modified ilizarov in difficult fracture of the patella. A case report. J Orthop Case Rep 2016;6:26-8. [Google Scholar]
- 6.Mahajan NP, Kumar GS, Kondewar P, Jadhav K Multi-fragment patellar non-union in a young patient due to failed fixation and its management- a rare case report. Trauma Int 2021;7:12-4. [Google Scholar]
- 7.Nathan ST, Fisher BE, Roberts CS, Giannoudis PV. The management of nonunion and delayed union of patella fractures: A systematic review of the literature. Int Orthop 2011;35:791-5. [Google Scholar]
- 8.Dhar SA, Mir MR. Use of the illizarov method to reduce quadriceps lag in the management of neglected non-union of a patellar fracture. J Orthop 2007;4:12. [Google Scholar]
- 9.Garg P, Sahoo S, Satyakam K, Biswas D, Garg A, Mitra S. Patellar nonunions: Comparison of various surgical methods of treatment. Indian J Orthop 2012;46:304-11. [Google Scholar]
- 10.Uvaraj NR, Vahanan NM, Sivaseelam A, Sameer MM, Basha IM. Surgical management of neglected fractures of the patella. Injury 2007;38:979-83. [Google Scholar]







