
Tension band wiring for osseous avulsion and triceps rupture is an easily reproducible technique with excellent outcomes.
Dr. Praveen Kumar Anbalagan, Department of Orthopaedics, MGM Medical College, Navi Mumbai, Maharashtra, India. E-mail: drpraveen93@yahoo.com
Introduction: Ideal treatment of chronic distal triceps rupture is controversial due to low occurrence of this injury. We report a unique case of chronic traumatic distal triceps rupture which was missed initially and then treated by tension band wiring.
Case Report: A 30-year-old manual labor presented with 2-month-old injury and difficulty in complete extension of the elbow which was initially managed conservatively. He was clinic-radiologically diagnosed as complete distal triceps bony avulsion tear. He was operated using tension band wiring technique. His DASH score at the end of 2-year follow-up was 5.4 indicating excellent outcome.
Conclusion: A strong clinical suspicion should be raised about triceps injury in patients with chronic elbow pain and weak extension. Tension band wiring technique gives good clinical and functional outcome in patients with bony avulsion along with distal triceps tear.
Keywords: Triceps rupture, chronic elbow pain, tension band wiring, modified Campbell Thompson test.
Rupture of the triceps tendon is an uncommon injury accounting for <1% of all the upper limb tendon injuries [1]. Due to the paucity in literature, there is a lack of proper guidelines for approaching these injuries [2, 3, 4, 5]. Although conservative treatment can be contemplated in patients with partial tear, surgical intervention gives good functional outcome in patients with complete tear. We report a case of chronic traumatic bony avulsion of distal triceps in a young adult which was missed initially by the primary physician. The avulsion was successfully treated with tension band wiring technique.
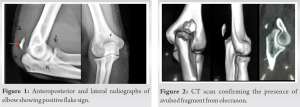
A 30-year-old right-hand dominant manual labor presented to our outpatient clinic with the complaints of difficulty in movements and intermittent pain around the right elbow joint for 2 months. There was an antecedent history of fall on an outstretched hand while playing cricket 2 months ago, which was treated conservatively by analgesics and rest. No investigation was performed at the time of initial injury since the patient responded partially to the conservative management. The patient had no comorbidities or history of similar complaints in the past. On examination, there was a small palpable gap at the posterior aspect of the right elbow just proximal to the olecranon tip. The sensory examination was within normal limits. Motor examination revealed a weakness in active extension at the right elbow. The modified Campbell Thompson test was positive which was suggestive of a complete triceps rupture. The extensors at the left elbow and bilateral flexors had power Grade 5. The palpable gap, weakness in active extension, and positive Thompson test lead to a suspicion of complete triceps rupture. Anteroposterior and lateral radiographs were then performed which revealed a positive flake sign (Fig. 1). A computed tomography scan was performed which confirmed the diagnosis and revealed a presence of 1.5 × 0.5 cm avulsed fragment from the olecranon tip (Fig. 2).
Thus based on the above findings, a decision for primary repair was taken. General anesthesia combined with brachial block was used. The patient was operated in lateral decubitus position with elbow in 90° flexion using a posterior approach. The triceps aponeurosis was incised and the osseous fragment of the olecranon tip was found to be attached to the distal aspect of triceps. There was a significant rent on the medial attachment of triceps tendon (Fig. 3). The edges at both the ends were freshened up and primary repair of triceps tendon was done using the transosseous technique (Fig. 4) A stainless steel wire was passed through the tunnels made in the proximal ulna and then taking it in a figure of 8 fashion through the distal triceps tendon (Fig. 5). The wire was twisted and the cut ends were buried deep. The triceps aponeurosis was repaired using non-absorbable Krakow type sutures with number 2 Ethibond (Ethibond Excel). The wound was closed over layers. Passive range of movements was assessed intraoperatively and 0–100° flexion was achieved.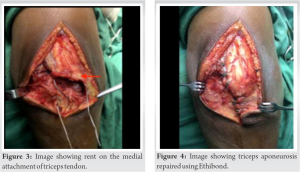
Post-operative protocol
An above-elbow posterior slab was then applied for 2 weeks following which gradual active and passive range of movements were begun. The patient had 0–120° flexion by the end of 6 weeks (Fig. 6). The final assessment was done using the Disability of Arm, Shoulder, and Hand scoring system [6] which was 5.4 at 2-year follow-up suggestive of an excellent outcome.
The most common mechanism of injury, leading to triceps rupture, is fall on an outstretched hand which can cause a forceful contraction of the distal triceps or a direct trauma [2, 3,4, 5]. It is more commonly seen in athletes and weight lifters with a male preponderance of 2:1 [4, 5]. Apart from the aforementioned causes, a variety of systemic and local factors have been attributed to triceps rupture. The systemic causes include chronic renal failure, renal osteodystrophy, rheumatoid arthritis, olecranon bursitis, diabetes, hypocalcemic tetany, metabolic disorders such as hyperparathyroidism, Marfan syndrome, or osteogenesis imperfect [5, 7, 8]. Local factors that can lead to tendon attrition include the use of anabolic steroid therapy [9, 10], local steroids, or treatment with quinolones [11]. The diagnosis of triceps rupture can be missed initially in up to 50% of the cases due to the low threshold of its suspicion [12,13]. Antecedent history of pre-existing illness or trauma associated with a definitive palpable gap just above the olecranon tip and lack of active extension should arouse a strong suspicion of distal triceps rupture. However, in an acute stage, the defect may not be that easily palpable due to the presence of swelling and ecchymosis [4, 13]. Similarly, some amount of extension at the elbow joint can be present due to the compensatory anconeus muscle or an intact lateral expansion. The modified Campbell Thompson test is based on the same principle as the Thompson test which is used to assess the integrity of tendoachilles in the lower limb. Nevertheless, the long lever arm in the forearm and less bulk of triceps as compared to tendoachilles makes this test less reproducible. Furthermore, the compensatory muscles can give a false-negative result which further questions the reproducibility of this test [4]. The patient in the present report had a positive modified Thompson test which was suggestive of a complete triceps rupture. While the intrasubstance triceps tears are difficult to diagnose and often require ultrasound or an MRI scan, the avulsion ruptures usually present with flake sign on plain radiographs like in the present report. Partial (>75%) and few cases with high-grade tear in non-demanding patients can be successfully treated non-surgically whereas surgical intervention is usually contemplated in young and active patients [4, 5, 13]. A myriad of surgical interventions has been proposed in the literature which depends on various factors such as a complete or partial tear, occupation of the patient, time of presentation, condition of the tendon, and retraction of the tendon. Direct repair is preferred in patients with recent tear (usually <3 weeks old) [2, 14] while procedures such as V-Y advancement [14], triceps turndown [3], and anconeus slide procedures [3, 5] are reserved with a significantly retracted tendon. Moreover, chronic tears have been reconstructed with auto as well as allografts in the recent past [13]. Due to the presence of a reasonable amount of bone stock and a significantly recent history of injury, a direct repair was planned. In the present case, the bony flake was attached to the ruptured tendon which was then incorporated in olecranon with the help of stainless steel wire. The further need to use K wires to hold the bony fragment was not required. To the best of our knowledge, the technique using the stainless steel wire alone has not been previously described in the literature which makes this case unique.
Tension band wiring technique gives good clinical and functional outcome in patients with chronic distal triceps rupture with bony involvement. There should be a high degree of clinical suspicion in diagnosing such injuries to avoid further complications.
The diagnosis of bony avulsion of distal triceps can easily be missed if not investigated thoroughly. Advanced imaging modalities such as a computed tomography scan or magnetic resonance imaging scan can help in diagnosing these injuries involving small bony fragments that can be easily missed on plain radiographs. Weakness in extension is a commonly complain which should not be ignored.
References
- 1.Anzel SH, Covey KW, Weiner AD, Lipscomb PR. Disruption of muscles and tendons; an analysis of 1, 014 cases. Surgery 1959;45:406-14. [Google Scholar]
- 2.Van Riet RP, Morrey BF, Ho E, O’Driscoll SW. Surgical treatment of distal triceps ruptures. J Bone Joint Surg Am 2003;85:1961-7. [Google Scholar]
- 3.Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ. Triceps tendon ruptures in professional football players. Am J Sports Med. 2004;32:431-4. [Google Scholar]
- 4.Yeh PC, Dodds SD, Smart LR, Mazzocca AD, Sethi PM. Distal triceps rupture. J Am Acad Orthop Surg 2010;18:31-40. [Google Scholar]
- 5.Sierra RJ, Weiss NG, Shrader MW, Steinmann SP. Acute triceps ruptures: Case report and retrospective chart review. J Shoulder Elbow Surg 2006;15:130-4. [Google Scholar]
- 6.Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The upper extremity collaborative group (UECG). Am J Ind Med 1996;29:602-8. [Google Scholar]
- 7.Bach BR Jr., Warren RF, Wickiewicz TL. Triceps rupture. A case report and literature review. Am J Sports Med 1987;15:285-9. [Google Scholar]
- 8.Clayton ML, Thirupathi RG. Rupture of the triceps tendon with olecranon bursitis. A case report with a new method of repair. Clin Orthop Relat Res 1984;184:183-5. [Google Scholar]
- 9.Lambert MI, Gibson AS, Noakes TD. Rupture of the triceps tendon associated with steroid injections. Am J Sports Med 1995;23:778. [Google Scholar]
- 10.Miles JW, Grana WA, Egle D, Min KW, Chitwood J. The effect of anabolic steroids on the biomechanical and histological properties of rat tendon. J Bone Joint Surg Am 1992;74:411-22. [Google Scholar]
- 11.Casparian JM, Luchi M, Moffat RE, Hinthorn D. Quinolones and tendon ruptures. South Med J 2000;93:488-91. [Google Scholar]
- 12.Sharma SC, Singh R, Goel T, Singh H. Missed diagnosis of triceps tendon rupture: A case report and review of literature. J Orthop Surg (Hong Kong) 2005;13:307-9. [Google Scholar]
- 13.Marinello PG, Peers S, Sraj S, Evans PJ. A treatment algorithm for the management of distal triceps ruptures. Tech Hand Up Extrem Surg 2015;19:73-80. [Google Scholar]
- 14.Weng PW, Wang SJ, Wu SS. Misdiagnosed avulsion fracture of the triceps tendon from the olecranon insertion: Case report. Clin J Sport Med 2006;16:364-5. [Google Scholar]






