
Pseudoaneurysm of the lateral genicular artery, a well-documented complication of a TKR, can also be a possible cause for recurrent hemarthrosis post-UKR. Timely diagnosis and concurrent management can prevent it from progressing and becoming debilitating.
Dr. Amyn M Rajani, Department of Orthopaedics, OAKS Clinic, Mumbai - 400 007, Maharashtra, India. E-mail: dramrajani@gmail.com
Introduction: Unicondylar knee replacement is a minimally invasive technique of surface replacement of the knee joint. Very little literature is available regarding vascular complications in patients who undergo this procedure due to their extremely rare nature.
Case Report: This first-of-its-kind report describes a case of pseudoaneurysm of the lateral genicular artery of the right knee in a hypertensive, 65-year-old man, following a single sitting bilateral unicompartmental knee replacement (UKR). With no involvement of the lateral compartment in UKR, we suspect an underlying mechanical element as the cause of the pseudoaneurysm. Patient presented with swelling and pain in the right knee for the first time at 8-month postoperatively, and after aspiration of the hemarthrosis, had two events of recurrence with increasing frequency. Dynamic magnetic resonance angiography confirmed the diagnosis and the patient underwent angiography-guided embolization of the lateral genicular artery using polyvinyl alcohol particles, with no recurrence in over a year since then.
Conclusion: Pseudoaneurysm of the lateral genicular artery is a possible cause of recurrent hemarthrosis even after unicondylar knee replacement and requires a high degree of suspicion for its timely diagnosis and management.
Keywords: Unicompartmental knee replacement, arthroplasty, pseudoaneurysm, genicular artery, hemarthrosis, recurrent.
Despite the rise in the number of surgeons preferring unicompartmental knee replacement (UKR) to total knee replacement (TKR) for their patients who suit the profile, the literature is elusive with regards to the complications arising intraoperatively and postoperatively to a UKR. One such aspect is vascular complications, which are a rare entity in TKR itself, forming a mere 0.03–0.2% cases [1]. Pseudoaneurysms of the popliteal, anterior tibial and genicular arteries have been reported in small numbers following TKR [2]. However, on scouring through the literature for studies based on complications following UKR [3], we found that the formation of a pseudoaneurysm post-UKR is not mentioned anywhere. Despite the rarity, it can rapidly deteriorate the condition of the operated knee to levels of being limb threatening, warranting a high index of suspicion to facilitate timely management. We report one such case who underwent a single-sitting, bilateral UKR, and presented with belated and recurrent complaints of swelling in the right knee. He was diagnosed with superior lateral genicular artery pseudoaneurysm on radiology and underwent suitable management.
A 65-year-old male presented to the clinic with bilateral knee pain. On clinical examination, he had tenderness restricted to the medial joint line, and a correctible varus deformity. Plain radiographs of bilateral knee joint confirmed the pain to be due to bilateral, severe, and medial compartment osteoarthritis of the knee joint (Fig. 1). The patient was on the treatment for hypertension for the past decade. He underwent bilateral UKR in single sitting. The intraoperative, perioperative, and immediate post-operative period was uneventful. The post-operative radiographs were acceptable, and the patient was discharged in a stable condition (Fig. 2). By 21st post-operative day, he improved to a normal gait with near-complete pain relief. On 8-month post-operative follow-up, he presented with pain in the right knee which was exaggerated on weight bearing, difficulty in bending the knee, and an alteration in the gait was observed (Fig. 3). On clinical examination, suprapatellar effusion was found due to a tense suprapatellar pouch and a positive patellar tap test. Consequently, the collection in the suprapatellar pouch of the affected knee joint was aspirated under all aseptic precautions. (Fig. 4) 120 cc of bloody aspirate was obtained, suggestive of hemarthrosis. Post-aspiration, the pain subsided, and the patient regained normal gait with no further complaints. Six months after this (1.5 years postoperatively), the patient presented with the same complaints in the same knee. Repeat aspiration of the suprapatellar pouch was done, and around 110 cc with bloody aspirate was noted. This time, the condition recurred after a mere 3 days, raising the suspicion of a pseudoaneurysm formation in the mind of the chief surgeon, due to the nature and the frequency of complaints.
By 21st post-operative day, he improved to a normal gait with near-complete pain relief. On 8-month post-operative follow-up, he presented with pain in the right knee which was exaggerated on weight bearing, difficulty in bending the knee, and an alteration in the gait was observed (Fig. 3). On clinical examination, suprapatellar effusion was found due to a tense suprapatellar pouch and a positive patellar tap test. Consequently, the collection in the suprapatellar pouch of the affected knee joint was aspirated under all aseptic precautions. (Fig. 4) 120 cc of bloody aspirate was obtained, suggestive of hemarthrosis. Post-aspiration, the pain subsided, and the patient regained normal gait with no further complaints. Six months after this (1.5 years postoperatively), the patient presented with the same complaints in the same knee. Repeat aspiration of the suprapatellar pouch was done, and around 110 cc with bloody aspirate was noted. This time, the condition recurred after a mere 3 days, raising the suspicion of a pseudoaneurysm formation in the mind of the chief surgeon, due to the nature and the frequency of complaints. 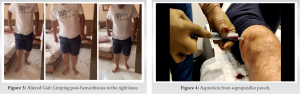 The patient was advised dynamic magnetic resonance angiography (Fig. 5) of his right lower limb. The diagnosis was confirmed to be a pseudoaneurysm of the right lateral genicular artery of the knee joint. The patient was referred to an interventional radiologist and he was advised angiography-guided embolization of the lateral genicular artery using polyvinyl alcohol particles (Fig. 6). Post-embolization, the recurrence of hemarthrosis stopped, and the patient was mobilized immediately. Over a year since then, the patient has had no recurrence and has achieved complete clinical and functional normalcy in terms of gait, range of motion, and return to activities of daily life.
The patient was advised dynamic magnetic resonance angiography (Fig. 5) of his right lower limb. The diagnosis was confirmed to be a pseudoaneurysm of the right lateral genicular artery of the knee joint. The patient was referred to an interventional radiologist and he was advised angiography-guided embolization of the lateral genicular artery using polyvinyl alcohol particles (Fig. 6). Post-embolization, the recurrence of hemarthrosis stopped, and the patient was mobilized immediately. Over a year since then, the patient has had no recurrence and has achieved complete clinical and functional normalcy in terms of gait, range of motion, and return to activities of daily life.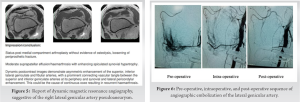
Spontaneous hemarthrosis after TKR is rare, occurring in 0.3–1% cases [1]. Pseudoaneurysm involves a fibrous wall, which increases in size due to systemic pressure. It can lead to debilitating sequalae by its ability to cause pressure effects on the surrounding neurovascular structures, and by its rupture into the surrounding soft tissue [1]. Pseudoaneurysm of the vascular structures in the knee joint has been well documented after a TKR, but there has been no report of the same following a UKR [4]. Pseudoaneurysm can occur following an extensive lateral release in a TKR, posterior capsular release, or due to a shear injury to an atherosclerotic vessel [1, 5]. Its formation after a UKR becomes intriguing as the lateral femoral condyle remains unexposed. Considering our patient was a long-standing hypertensive, and the belated presentation of complaints, we hypothesize the formation of pseudoaneurysm of the lateral genicular artery in our case, either following intraoperative manipulations or plaque disruption in a non-compliant, atherosclerotic vessel, due to pneumatic tourniquet or thermal injury by exothermic nature of cement. The belated presentation could imply the formation of a small pseudoaneurysm at onset, which progressively increased in size. Multiple treatment modalities exist, including direct compression, excision, ligation, ultrasound guided thrombin injection, intravascular coils, or beads [1, 6, 7, 8]. However, Angiographic coil embolization is considered as the best treatment for post-arthroplasty pseudoaneurysms thanks to its minimally invasive nature that ensures lesser chances of infection, uninhibited rehabilitation, and diagnosis as well as definitive treatment in the same procedure [1, 9]. A solitary case of popliteal artery pseudoaneurysm, 7-day post-UKR, has been reported recently by Sadat U et al. The case was managed successfully by angiography-assisted stenting [10]. Keeping this in mind, once the diagnosis was made in our case, immediate angiographic embolization was undertaken, leading to complete subsidence of the condition, and excellent short-term as well as long-term results.
The purpose behind reporting this case is to make fellow orthopedicians aware about the plausibility of pseudoaneurysm of even the lateral genicular artery following a UKR, despite the lateral compartment of the knee not being involved in UKR. Retaining a high index of suspicion in cases with recurrent or persistent hemarthrosis post-surgery is strongly recommended. If diagnosed early, it can be successfully treated using radiological endovascular techniques, without compromising on the rehabilitation of the patient, and ensuring complete recovery.
Pseudoaneurysm of the lateral genicular artery, a well- documented complication of a TKR, can also be a possible cause for recurrent hemarthrosis post-UKR. Timely diagnosis and concurrent management can prevent it from progressing and becoming debilitating.
References
- 1.Saini P, Meena S, Malhotra R, Gamanagatti S, Kumar V, Jain V. Pseudoaneurysm of the superior lateral genicular artery: Case report of a rare complication after total knee arthroplasty. Patient Saf Surg 2013;7:15. [Google Scholar]
- 2.Ji JH, Park SE, Song IS, Kang H, Ha JY, Jeong JJ. Complications of medial unicompartmental knee arthroplasty. Clin Orthop Surg 2014;6:365-72. [Google Scholar]
- 3.Agarwala SR, Mohrir GS, Dotivala SJ. Posttraumatic pseudoaneurysm of popliteal artery following total knee arthroplasty. Indian J Orthop 2013;47:101-3. [Google Scholar]
- 4.Law KY, Cheung KW, Chiu KH, Antonio GE. Pseudoaneurysm of the genicular artery following total knee arthroplasty: A report of two cases: J Orthop Surg 2007;15:386-9. [Google Scholar]
- 5.Calligaro KD, Dougherty MJ, Ryan S, Booth RE. Acute arterial complications associated with total hip and knee arthroplasty. J Vasc Surg 2003;38:1170-7. [Google Scholar]
- 6.Paschalidis M, Theiss W, Kolling K, Busch R, Schomig A. Randomised comparison of manual compression repair versus ultrasound guided compression repair of postcatheterisation femoral pseudoaneurysms. Heart 2006;92:251-2. [Google Scholar]
- 7.Olsen DM, Rodriguez JA, Vranic M, Ramaiah V, Ravi R, Diethrich EB. A prospective study of ultrasound scan-guided thrombin injection of femoral pseudoaneurysm: A trend toward minimal medication. J Vasc Surg 2002;36:779-82. [Google Scholar]
- 8.Klonaris C, Katsargyris A, Matthaiou A, Giannopoulos A, Tsigris C, Papadopouli K, et al. Emergency stenting of a ruptured infected anastomotic femoral pseudoaneurysm. Cardiovasc Intervent Radiol 2007;30:1238-41. [Google Scholar]
- 9.Chen L, Liang W, Zhang X, Cheng B. Indications, outcomes, and complications of unicompartmental knee arthroplasty. Front Biosci (Landmark Ed) 2015;20;689-704. [Google Scholar]
- 10.Sadat U, Naik J, Verma P, See TC, Cousins C, Chitnavis JP, et al. Endovascular management of pseudoaneurysms following lower limb orthopedic surgery. Am J Orthop (Belle Mead NJ) 2008;37:E99-102. [Google Scholar]








