
Talectomy and tibiocalcaneal arthrodesis can be an effective option for management for advanced cases of giant cell tumor of the talus.
Dr. Nilesh S Sakharkar, Department of Orthopaedics, Government Medical College and Hospital, Nagpur - 440 003, Maharashtra, India. E-mail: orthodrnilesh@gmail.com
Introduction: Giant cell tumor of bone most commonly involves ends of the long bones in a skeletally mature patient. Giant cell tumor of the bones of the hand and feet is very rare, so is the giant cell tumor of talus.
Case Report: We are reporting a case of giant cell tumor of talus in a 17-year-old female who presented with a history of pain and swelling around left ankle since 10 months. Radiographs of the ankle showed lytic expansile lesion involving whole of talus. Talectomy followed by calcaneo-tibial fusion was done as intralesional curettage was not feasible in this patient. Histopathology confirmed the diagnosis of giant cell tumor. There was no evidence of recurrence even at 9 years follow-up and the patient was able to carry out her daily activities without much discomfort.
Conclusion: Giant cell tumor is most commonly encountered around the knee or distal radius. Involvement of foot bones especially talus is extremely uncommon. In early presentation, extended intralesional curettage with bone grafting and, in late, talectomy with tibiocalcaneal fusion are the treatment options.
Keywords: Talectomy, giant cell tumor, osteoclastoma, tibiocalcaneal fusion.
Giant cell tumor of bone most commonly involves ends of the long bones [1, 2]. Giant cell tumor of the bones of the hand and feet is very rare, so is the giant cell tumor of talus [1, 2, 3]. We are reporting a case of giant cell tumor of talus in a 19-year-old female.
A 19-year-old female presented with history of pain in the left ankle since 10 months. Pain had gradually increased over the time so that, at the time of presentation, the patient had restricted daily activities. She also had swelling over left ankle region since last 3 months. On examination, swelling and tenderness of ankle were present. Subtalar and ankle joint movements were painful and restricted. Plain radiographs of the ankle revealed expansile osteolytic lesion of the talus which had expanded whole of the talus and the bony cortices were thinned out but were not broken (Fig. 1). CT scan of ankle showed thinning of all the cortices, but no evidence of cortical break or soft-tissue extension was found (Fig. 2). 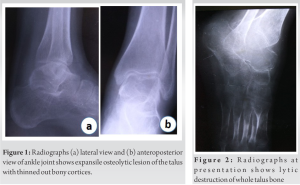 Patient’s hemoglobin, white blood cell count, and erythrocyte sedimentation rate were normal. Fine-needle aspiration cytology from the lesion showed giant cell rich lesion of the bone. The patient was posted for surgery. By anterior approach, talectomy was done. Then, tibiocalcaneal fusion was done using external fixator without using bone graft (Fig. 3). Post-operative period was uneventful. Histopathological examination proved the lesion to be giant cell tumor. External fixator was removed at 3 months and the patient was advised full weight-bearing along with the use of ankle-foot orthosis. There is no evidence of recurrence at 9 years of follow-up.
Patient’s hemoglobin, white blood cell count, and erythrocyte sedimentation rate were normal. Fine-needle aspiration cytology from the lesion showed giant cell rich lesion of the bone. The patient was posted for surgery. By anterior approach, talectomy was done. Then, tibiocalcaneal fusion was done using external fixator without using bone graft (Fig. 3). Post-operative period was uneventful. Histopathological examination proved the lesion to be giant cell tumor. External fixator was removed at 3 months and the patient was advised full weight-bearing along with the use of ankle-foot orthosis. There is no evidence of recurrence at 9 years of follow-up.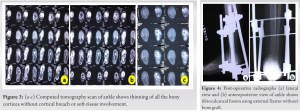
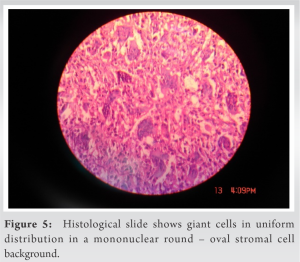
Giant cell tumor of bone is a disease of mature skeleton, most commonly seen in the age group of 20–45 years. Distal femur, proximal tibia, and distal radius are the most common sites of giant cell tumor. However, involvement of proximal humerus, distal tibia, sacrum, proximal femur, pelvis, and spine by giant cell tumor is not rare [1, 2, 3]. Involvement of the small bones of foot by giant cell tumor is rare. Mirra et al. [4] reported an incidence of <2% and Unni [5] reported an incidence of 1.2% of giant cell tumor in the foot. Sung et al. found only one case in the talus in their series of 208 cases of giant cell tumor. Biscaglia et al. [6] reported an incidence of nine cases of giant cell tumor of talus out of about 900 cases of giant cell tumor presenting at their institute for 50 years. Thus, giant cell tumor of talus is a fairly rare occurrence. Histologically, aneurysmal bone cyst and giant cell reparative granuloma may mimic giant cell tumor. However, in case of giant cell tumor, giant cells have a uniform distribution in a mononuclear round – oval stromal cell background (Fig. 4). Changes of secondary ABC may be present in true giant cell tumor. Radiologically, most of the giant cell tumor in the foot present as lytic expansile lesions with no periosteal reaction. Cortex of the involved bone shows thinning or destruction in almost all the case [6, 7]. The treatment options for giant cell tumor of foot include simple curettage, curettage plus bone grafting, aggressive curettage plus bone grafting/bone cementing, and resection. Simple curettage and curettage plus bone grafting have produced recurrence rates of about 50–80% in foot lesions. On the other hand, aggressive curettage plus bone grafting/bone cementing and resection of foot lesions have given recurrence rates in the range of 15–30%. These are comparable to recurrence rates after similar procedures for giant cell tumor of the long bones. Hence, aggressive curettage plus bone grafting and resections appear to be the treatment of choice for foot lesions [6, 7]. About 30% cases of giant cell tumor of bones of foot are seen in patients younger than 20 years. Bapat et al. [8] and Ramdas et al. [9] have reported giant cell tumor of talus in skeletally immature patients. Giant cell tumor of the bones of foot shows a tendency to be multicentric. Hence, a skeletal survey is indicated for giant cell tumor of the foot [10]. Our case did not show any evidence of multicentricity on skeletal survey. In our case, the tumor had expanded whole of talus so talectomy was preferred over curettage and bone grafting. Tibiocalcaneal fusion was done with the help of an external fixator. Even at 9 years of follow-up, there was no evidence of recurrence and the patient was able to carry out her daily activities without much discomfort.
Giant cell tumor is most commonly encountered around the knee or distal radius. Involvement of foot bones especially talus is extremely uncommon. If the patient presents early, extended intralesional curettage with bone grafting is recommended. However, in late presentation, talectomy with tibiocalcaneal fusion can ensure reasonably good functional outcome without risk of recurrence.
Although extended intralesional curettage with bone grafting is the recommended modality of treatment of giant cell tumor; in cases who present late with destruction of the bone and hardly any bone stock remaining, excision with fusion can be a good alternative for reconstruction.
References
- 1.Sung HW, Kuo DP, Shu WP, Chai YB, Liu CC, Li SM. Giant-cell tumor of bone: Analysis of two hundred and eight cases in Chinese patients. J Bone Joint Surg Am 1982;64:755-61. [Google Scholar]
- 2.Campanacci M, Baldini N, Boriani S, Sudanese A. Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-14. [Google Scholar]
- 3.Wold LE, Swee RG. Giant cell tumor of the small bones of the hand and feet. Semn Diag Pathol 1984;1:173-84. [Google Scholar]
- 4.Mirra JM, Picci P, Gold RH, editors. Bone Tumors: Clionical, Radiologic and Pathological Correlations. Philadelphia: Lea and Febiger; 1989. p. 941-1020. [Google Scholar]
- 5.Unni KK, editor. Dahlin’s Bone Tumors: General Aspects and Data on 11087 Cases. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996. p. 263-83. [Google Scholar]
- 6.Biscaglia R, Bacchini P, Bertoni F. Giant cell tumor of the bones of the hand and foot. Cancer 2000;88:2022-32. [Google Scholar]
- 7.O’Keefe RJ, O’Donnell RJ, Temple HT, Scully SP, Mankin HJ. Giant cell tumor of bone in the foot and ankle. Foot Ankle Int 1995;16:617-23. [Google Scholar]
- 8.Bapat MR, Narlawar RS, Pimple MK, Bhosale PB. Giant cell tumour of talar body. J Postgrad Med 2000;46:110-1. [Google Scholar]
- 9.Ramdas A, Rao KR, Thomas A, Varghese RG, Gnanadoss JJ. Giant cell tumour of talus--a case report. J Indian Med Assoc 2007;105:96-8. [Google Scholar]
- 10.Cummins CA, Scarborough MT, Enneking WF. Multicentric giant cell tumor of bone. Clin Orthop Relat Res 1996;322:245-52. [Google Scholar]





