
Primary hyperparathyroidism is an indolent disease that must be taken in consideration while dealing with bone lesion associated with hypercalcemia.
Dr. Abhishek Kumar Rai, Department of Orthopaedics, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India. E-mail: abhishek110891@gmail.com
Introduction: Primary hyperparathyroidism may mimic osteoporosis and lead to pathological fractures.
Case Report: We report a case of 35-year-old female who sustained left distal tibia-fibula fracture after a trivial fall, later diagnosed to have left inferior parathyroid adenoma. The fracture was managed conservatively and left inferior parathyroidectomy for the adenoma. At 4 years follow-up, there are no clinical or biochemical signs of recurrence
Conclusion: Pathological fracture in a case of parathyroid adenoma is extremely rare and requires a multidisciplinary approach for optimal outcome. A combination of clinical, biological, radiological, and biochemical markers with a high index of suspicion in an isolated bone fracture is required to diagnose parathyroid adenoma.
Keywords: Pathological fracture, parathyroid adenoma, parathyroidectomy, tibia-fibula fracture, single photon emission computed tomography.
Parathyroid adenoma is a continuum of parathyroid proliferative pathogenesis which starts with hyperplasia of parathyroid follicles and may result in parathyroid carcinoma [1]. Most of the patients present with non-specific symptoms of loss of appetite, polyuria, polydipsia, and fatigue. The intestinal symptoms are loss of appetite, nausea, and bloating [2]. Musculoskeletal symptoms include myalgia, bone pain, and osteoporosis [2]. Thus, the patients usually present with intestinal, renal, and musculoskeletal symptoms simultaneously. The diagnosis is usually confirmed by biochemical screening of elevated serum calcium levels, decreased phosphate levels, and elevated serum parathyroid levels [3]. With increased awareness on health, hypercalcemia is usually documented incidentally on routine biochemical work up [4]. Primary hyperparathyroidism is mainly caused by parathyroid adenoma followed by follicular hyperplasia and parathyroid carcinoma [5]. Follicular hyperplasia typically presents with hyperplasia of all four parathyroid glands. On the contrary, parathyroid adenoma usually involves only one gland. Normally, parathyroid glands are too small (5 mm × 3 mm × 1 mm) in size to be detected on routine imaging. The routine imaging modalities to visualize parathyroid adenoma include ultrasonography (USG) and 99mTc-sestamibi scintigraphy [6]. Single photon emission computed tomography (SPECT) has higher sensitivity over sestamibi scan for the visualization of parathyroid adenoma. To visualize ectopic glands, contrast enhanced computed tomography/MRI can be used [6]. Considering the vague symptoms, an isolated fracture makes the clinical presentation extremely rare to be diagnosed as a parathyroid adenoma, leading to mis-management. We report this case of an isolated fracture, later diagnosed as a parathyroid adenoma leading to exploration of the neck.
A 35-year-old previously healthy female with insignificant past medical or surgical history presented to our Outpatient Department (OPD) with significant pain over her left leg. She had a history of trivial fall, when she slipped while cleaning her room. On clinical examination, the patient had sustained a closed injury over her left distal leg. She was having pain and swelling over the injury, predominantly on the lateral aspect. Tenderness could be elicited over the left lateral malleolus. The distal pulses and neurological examination were normal. Standard radiographs revealed left distal tibia-fibula fracture (Fig. 1). We planned to manage her conservatively on above-knee slab, limb elevation, ice fomentation, and analgesics. Considering the fall to be trivial, we did biochemical investigations to rule out any metabolic disorder. The biochemical reports showed severe hypercalcemia: 12.4 mg/dL (Norma l: 8.6–10.3 mg/dL), hypophosphatemia: 1.9 mg/dL (Normal: 2.8–4.5 mg/dL), high levels of serum Parathyroid Hormone (PTH): 1 2 2 6 p g / m l (No rma l : 1 1 – 5 1 p g / m l ), hypercalciuria 276 nmol/L (Normal: 3–8nmol/L), and raised Alkalin Phosphatase level: 642 IU/L (Normal: 30–300 IU/L). Biochemical reports suggested hyperparathyroidism. Bone densitometry values were <−2.5 SD, suggestive of severe osteoporosis. To rule out, parathyroid disorder, USG, was done which revealed left inferior parathyroid hyperplasia. We, further, investigated with parathyroid scan coupled with SPECT using 99mTc-sestamibi tracer (Fig. 2). SPECT showed a 28 mm mass in the left inferior parathyroid gland. After consultation with the endocrinologist and surgeons, the patient underwent exploration of neck for parathyroid adenoma. Intraoperative findings confirmed a 2.4 cm mass in the left inferior parathyroid (Fig. 3). The mass was not adhered to any vital adjacent structure and was removed en bloc. There was a drastic fall in the levels of PTH immediately after the removal of mass. The PTH levels returned to normal (18 pg/ml) at 1st post-operative day. The patient was supplemented with oral calcium and vitamin D postoperatively to prevent hypocalcaemia. The resected mass was sent for histopathological examination (HPE). HPE showed a mixture of chief cells and predominant oxyphill cells with delicate fibrovascular bands suggestive of parathyroid adenoma (Fig. 4). After the parathyroid excision, the patient was followed up regularly in OPD at 1 month interval for clinicoradiological examination. The fracture united at 3 months follow-up. We repeated the biochemical investigations after 3 months which turned out to be normal. The patient was last followed up at 4 years, with no clinical or biochemical markers of recurrence (Fig. 5).
Primary hyperparathyroidism is a common endocrine disorder, mainly affecting the postmenopausal women. It is usually diagnosed by the elevated levels of serum calcium and PTH [7]. The preliminary diagnosis of adenoma is usually done by USG and sestamibi scan. Diagnosis is confirmed by HPE. The usual asymptomatic or oligosymptomatic presentation of parathyroid adenoma makes the diagnosis difficult. An isolated bone fracture in a case of parathyroid adenoma is extremely rare and, thus, makes the diagnosis difficult. A thorough search of PubMed showed <10 cases of pathological fracture, secondary to parathyroid adenoma. Bennett et al. reported a case of an adolescent female, who sustained right femoral neck fracture [8]. The case was managed by closed reduction, internal fixation with pinning, and a hip spica cast. Two weeks later, the parathyroid adenoma was excised. Buisset et al. reported a case of a 40-year-old female with pathological left forearm fracture, managed conservatively on cast [9]. The patient was diagnosed to have a right inferior parathyroid mass which was excised en bloc. Terro et al. managed a case of the left clavicle fracture in a 41-year-old male conservatively [10]. He was having a giant parathyroid adenoma which was operated for the right lower parathyroidectomy. We present a similar, extremely rare case of the left distal tibia-fibula fracture in a previously asymptomatic female. As the fall was trivial, a planned and staged protocol for a pathological fracture was followed to diagnose parathyroid adenoma. After the excision of parathyroid adenoma, the fracture united by 3 months follow-up with normal biochemical markers. The limitation of the study is a short duration of follow-up of 4 years. Although the recurrence is most commonly reported within 2–3 years of excision, a longer follow-up may be needed for long-term outcome.
Terro et al. managed a case of the left clavicle fracture in a 41-year-old male conservatively [10]. He was having a giant parathyroid adenoma which was operated for the right lower parathyroidectomy. We present a similar, extremely rare case of the left distal tibia-fibula fracture in a previously asymptomatic female. As the fall was trivial, a planned and staged protocol for a pathological fracture was followed to diagnose parathyroid adenoma. After the excision of parathyroid adenoma, the fracture united by 3 months follow-up with normal biochemical markers. The limitation of the study is a short duration of follow-up of 4 years. Although the recurrence is most commonly reported within 2–3 years of excision, a longer follow-up may be needed for long-term outcome.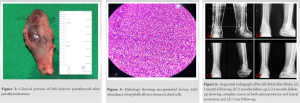
Considering parathyroid adenoma to be rare in premenopausal females, a high index of suspicion is required to diagnose an extremely rare presentation of isolated bone fracture. Primary hyperparathyroidism is an indolent disease that must be taken in consideration while dealing with bone lesion associated with hypercalcemia. A combination of clinicoradiological and biochemical studies with an expertise in dealing pathological fractures helps in the optimum treatment. Such rare presentations can be best managed by a multidisciplinary approach to achieve the best possible outcome.
Combination of clinicoradiological and biochemical studies with a high index of suspicion helps to diagnose the underlying pathology.
References
- 1.Wieneke JA, Smith A. Parathyroid adenoma. Head Neck Pathol 2008;2:305-8. [Google Scholar]
- 2.Yigit B, Tanal M, Citgez B. Giant parathyroid adenoma diagnosed by brown tumour, a clinical manifestation of primary hyperparathyroidism: A case report. J Pak Med Assoc 2021;71:1266-9 [Google Scholar]
- 3.Adegoke OO, Ajani MA, Awosusi BL, Onakpoma FA, Saiki O, Daniel A. Parathyroid adenoma with unusual presentations of rib bone and thoracic vertebrae fractures in a premenopausal female in Ibadan, Nigeria. Niger Med J 2020;61:273-5. [Google Scholar]
- 4.Łach J, Dyaczyński M, Buczkowski K. Primary hyperparathyroidism on the example of a 33-year-old female patient with parathyroid adenoma. Pol Przegl Chir 2019;92:55-61. [Google Scholar]
- 5.Hussain A, Mahmood H, Geddoa E, Hamish M, Reda AH. Parathyroid adenoma and hypercalcemia in a patient presenting with multiple pathological fractures of the long bones. Int J Surg 2008;6:465-8. [Google Scholar]
- 6.Johnson NA, Carty SE, Tublin ME. Parathyroid imaging. Radiol Clin North Am 2011;49:489-509, vi. [Google Scholar]
- 7.Pappu R, Jabbour SA, Reginato AM, Reginato AJ. Musculoskeletal manifestations of primary hyperparathyroidism. Clin Rheumatol 2016;35:3081-7. [Google Scholar]
- 8.Bennett JT, Alex ander HH, Morrissy RT. Parathyroid adenoma presenting as a pathologic fracture of the femoral neck in an adolescent. J Pediatr Orthop 1986;6:473-6. [Google Scholar]
- 9.Buisset C, Demarquet L, Raynal M, Busby H, Nominé-Criqui C, Brunaud L. When a pathological forearm fracture led to explore the neck: About a case. Head Neck Pathol 2020;14:828-32. [Google Scholar]
- 10.Terro JJ, El-Helou E, El-Khoury E, Lakkis RS, Shibli A, Al Raishouni MA, et al. Giant parathyroid adenoma presenting with a pathological left clavicular fracture: An extremely rare case report. Int J Surg Case Rep 2020;75:311-6. [Google Scholar]








