Surgeons may reasonably use common reconstructive methods in pediatric patients with acute flaccid myelitis presenting with painful hip displacement to increase comfort, reestablish anatomic alignment, and prevent long-term recurrence.
Ms. Amy L Xu, Department of Orthopaedic Surgery, The Johns Hopkins Hospital, 1800 Orleans St, Baltimore, Maryland 21287, USA. E-mail: amyxu@jhmi.edu
Introduction: Acute flaccid myelitis (AFM) is a recently described diagnosis that primarily impacts the pediatric population. It is characterized by profound proximal muscle weakness with resultant orthopedic manifestations similar to well-known neuromuscular conditions. While the incidence of AFM has been rising, management outcomes are understudied. Here, we describe the first known case of hip reconstruction in AFM.
Case Report: A 5-year-old female presented with painful bilateral hip subluxations 2 years after being diagnosed with AFM. Imaging confirmed substantial uncovering of the femoral heads, right greater than left, with reduction on abduction views. Given the extent of her hip pathology and symptoms, she underwent bilateral Dega and varus derotational osteotomies with adductor lengthening, achieving a 35° correction in femoral neck angle and 30° reduction in femoral anteversion bilaterally. At 2 years postoperatively, she was asymptomatic without recurrence of hip displacement.
Conclusion:Reconstructive femoral osteotomies can be effective for achieving painless, reduced hips in patients with AFM. Thus, surgeons may reasonably extrapolate current concepts utilized for other low-tone neuromuscular conditions to inform approach to AFM.
Keywords: Acute flaccid myelitis, hip displacement, hip reconstruction, varus derotational osteotomy, Dega osteotomy, neuromuscular.
Acute flaccid myelitis (AFM) has been diagnosed in over 650 individuals worldwide – largely in the pediatric population – since the Centers for Disease Control and Prevention began tracking its epidemiology in August 2014 [1] . It is a syndrome characterized by acute onset of flaccid paralysis – prominently of the proximal musculature – accompanied by longitudinal gray matter spinal cord lesions on magnetic resonance imaging; it results in a myriad of neurological manifestations and is suspected to be secondary to mainly enterovirus infection [2, 3]. The profound muscle weakness may lead to long-term orthopedic sequalae, including scoliosis and joint subluxation or dislocation [4, 5]. If not painful, neuromuscular hip displacement can be managed with observation. If patients are symptomatic, non-operative options include pain medication, physical therapy, and corticosteroid injections. In cases of severe pain that is not responsive to these conservative measures, soft-tissue releases and reconstructive surgeries can be pursued [6]. There is currently no evidence regarding the outcomes of reconstructive surgeries for hip displacement in patients with AFM. Here, we describe the first case of surgical reconstruction for bilateral painful hip subluxation in a 5-year-old female patient with AFM who underwent bilateral Dega and varus derotational osteotomies.
A 5-year-old female patient presented to the orthopedic surgery clinic in October 2020 for initial consultation of painful bilateral hip subluxation in the setting of AFM diagnosed in September 2018. She had a medical history of AFM sequalae including quadriplegia, scoliosis, bilateral shoulder subluxations, and recently diagnosed low bone mass treated with pamidronate. Surgical history included nerve transfers for her right upper limb (median to musculocutaneous, radial to axillary, and spinal accessory to suprascapular nerves) and bilateral lower limbs (sciatic to inferior gluteal nerves). Her parents began noticing popping sounds in her hips approximately 1 year before presentation to the clinic. On physical examination, passive hip range of motion was 0 to 110° with abduction to 50° and mild degree of discernable subluxation. Flexion contractures were observed and estimated at 30° on the right and 20° on the left. Muscle strengths were as follows: quadriceps 4/5, thigh adductors 4/5, thigh abductors 3/5, and hamstrings 4/5. Mild lumbar spinal asymmetry was noted without obvious pelvic obliquity. The patient used a manual wheelchair for community mobility but was able to ambulate short distances with the assistance of a crocodile posterior walker with forearm support and bilateral ankle foot orthoses (AFOs). Radiographs revealed evidence of bilateral hip dysplasia and coxa valga with superolateral subluxation –>75% uncovering of the right femoral head and >50% of the left (Fig. 1a). On abduction views, both hips reduced and appeared located (Fig. 1b). Due to the extent of hip pathology and pain with weight-bearing, surgical correction was recommended. The patient underwent bilateral Dega osteotomies with autogenous tricortical structural bone graft and varus derotational osteotomies, fixed with blade plates and cannulated screws, respectively. The procedure achieved a 35° correction in femoral neck angle and 30° reduction of anteversion from 50 to 20° bilaterally. During the same procedure, the patient also underwent bilateral adductor lengthening. Subsequently, she was admitted for inpatient rehabilitation as planned preoperatively. At 6 week s post-operative, the patient presented for a follow-up visit without reported complications and negligible pain. Surgical sites and osteotomies were well-healed. Radiographs demonstrated improved alignment of the bilateral hips, with located femoral heads, greater acetabular coverage, and decreased coxa valga (Fig. 2).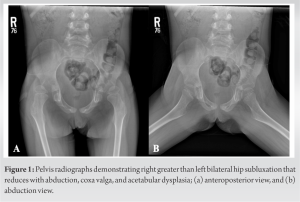 At 2 years post-operative, the patient presented without reported complications or complaints of pain. Residual flexion contractures were estimated at 5° on the right and 11° on the left, reduced since before surgery. Functionally, she was able to transition independently from sit to stand as well as into and out of her wheelchair with minimal assistance, and she could ascend a flight of stairs by sidestepping with use of a railing. She maintained her ability to ambulate short distances with her walker and AFOs. Her radiographs were unchanged from the early post-operative period (Fig. 3).
At 2 years post-operative, the patient presented without reported complications or complaints of pain. Residual flexion contractures were estimated at 5° on the right and 11° on the left, reduced since before surgery. Functionally, she was able to transition independently from sit to stand as well as into and out of her wheelchair with minimal assistance, and she could ascend a flight of stairs by sidestepping with use of a railing. She maintained her ability to ambulate short distances with her walker and AFOs. Her radiographs were unchanged from the early post-operative period (Fig. 3).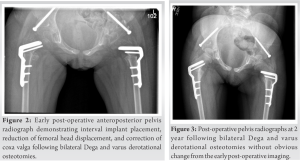
The flaccid weakness typical of AFM tends to develop over the course of several hours to days after the viral prodrome, often with marked asymmetry involving the proximal muscles. It has a predilection for the upper limbs, but the lower limbs are also affected in up to 66% of cases [2, 4]. Hip migration may occur secondary to this weakness of the proximal musculature, which resulted in coxa valga, progressive hip lateralization, and acetabular dysplasia in other neuromuscular conditions with similar clinical presentation [7]. The present case is the first to describe reconstructive surgery for symptomatic hip displacement in the setting of AFM. While the orthopedic manifestations of AFM have yet to be studied extensively, the characteristic flaccid weakness likens that of other neuromuscular disorders – including spinal muscular atrophy (SMA) – and allows for comparison of concepts. A combination of diminished weight-bearing and profound gluteal muscle weakness is thought to attenuate the stimulus for trochanteric apophyseal growth. The resultant coxa valga subsequently places patients at greater risk for femoral head migration [8]. Of note, this mechanism differs than that proposed for other conditions, like myelodysplasia, which have spastic features and more predominant sensory abnormalities in addition to motor impairment. In other conditions involving proximal weakness, hip subluxations or dislocations have traditionally been reported as painless due to less resistance from surrounding musculature [7, 8]. Anecdotally, we understand a subset of these populations to still experience painful hip displacement that interferes with daily activities. A recent study demonstrated that hip dislocation, as determined clinically or radiographically, is an independent predictor of moderate-to-severe hip pain in patients with SMA [9]. In the present case, we illustrate that patients with AFM can similarly experience symptomatic hip dislocation related to their low muscle tone and weakness. However, we are currently unable to speak to the prevalence of hip displacement or associated pain in AFM and its emerging burden for the medical community. In regard to management of the dislocated hip, there is substantial controversy regarding the value of reconstructive surgeries for conditions with muscle weakness. Shapiro et al. [10, 11, 12] advocated for aggressive soft-tissue procedures and varus osteotomy of the proximal femur to maintain reduction in SMA. O’Brien et al. [13] recommended a similar approach for hip dislocation secondary to poliomyelitis. Surgical reduction can improve refractory symptoms via correcting sitting balance, maintaining pelvic alignment, and lowering the incidence of ischial decubitus ulceration [8]. Despite positive outcomes in a subset of patients, lesser resistance surrounding the joint structure also means greater susceptibility to recurrent subluxation, even after joint reconstruction [7, 8, 14, 15]. Due to this, some physicians question the value of operative treatment for painless hip displacement in these populations, as patients are privy to perioperative complications while potentially achieving only transient benefits. Yet, it must be noted that pain relief following reconstruction can be substantial and improve quality of life, highlighting the value of such procedures in symptomatic cases refractory to more conservative measures [9].
In the present case, a pediatric patient presented with painful bilateral hip displacement and associated valgus deformity and acetabular dysplasia in the setting of AFM. Her symptoms improved following bilateral Dega and varus derotational osteotomies, and she remained asymptomatic at 2 years following surgery without evidence of recurrent subluxation. This case demonstrates that considerations for orthopedic manifestations of other low-tone neuromuscular conditions extend to AFM, and reconstruction with femoral osteotomies can help achieve a painless hip when appropriate. With the potentially increasing prevalence of AFM, future research must continue to assess orthopedic developments in this population and the effectiveness of surgical correction.
The orthopedic manifestations of AFM are similar to those of other low-tone neuromuscular conditions, and therefore, surgeons may reasonably use common reconstructive methods in pediatric patients with AFM presenting with painful hip displacement to increase comfort, reestablish anatomic alignment, and prevent long-term recurrence.
References
- 1.Centers for Disease Control and Prevention. AFM Cases and Outbreaks. CDC. Available from: https://www.cdc.gov/acute-flaccid-myelitis/cases-in-us.html [Last accessed on 2022 Jan 12]. [Google Scholar]
- 2.Messacar K, Schreiner TL, Van Haren K, Yang M, Glaser CA, Tyler KL, et al. Acute flaccid myelitis: A clinical review of US cases 2012-2015. Ann Neurol 2016;80:326-38. [Google Scholar]
- 3.Helfferich J, Knoester M, Van Leer-Buter CC, Neuteboom RF, Meiners LC, Niesters HG, et al. Acute flaccid myelitis and enterovirus D68: Lessons from the past and present. Eur J Pediatr 2019;178:1305-15. [Google Scholar]
- 4.Murphy OC, Messacar K, Benson L, Bove R, Carpenter JL, Crawford T, et al. Acute flaccid myelitis: Cause, diagnosis, and management. Lancet 2021;397:334-46. [Google Scholar]
- 5.Melicosta ME, Dean J, Hagen K, Oppenheimer K, Porter C, Rybczynski S, et al. Acute flaccid myelitis: Rehabilitation challenges and outcomes in a pediatric cohort. J Pediatr Rehabil Med 2019;12:245-53. [Google Scholar]
- 6.Shrader MW, Wimberly L, Thompson R. Hip surveillance in children with cerebral palsy. J Am Acad Orthop Surg 2019;27:760-8. [Google Scholar]
- 7.Canavese F, Sussman MD. Strategies of hip management in neuromuscular disorders: Duchenne muscular dystrophy, spinal muscular atrophy, charcot-marie-tooth disease and arthrogryposis multiplex congenita. Hip Int 2009;19:S46-52. [Google Scholar]
- 8.Sporer SM, Smith BG. Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-4. [Google Scholar]
- 9.Xu A, Crawford T, Sponseller P. Hip pain in patients with spinal muscular atrophy: Prevalence, intensity, interference, and factors associated with moderate to severe pain. J Pediatr Orthop 2022;42:273-9. [Google Scholar]
- 10.Shapiro F, Bresnan MJ. Orthopaedic management of childhood neuromuscular disease. Part I: Spinal muscular atrophy. J Bone Joint Surg Am 1982;64:785-9. [Google Scholar]
- 11.Shapiro F, Bresnan MJ. Orthopaedic management of childhood neuromuscular disease. Part II: Peripheral neuropathies, Friedreich’s ataxia, and arthrogryposis multiplex congenita. J Bone Joint Surg Am 1982;64:949-53. [Google Scholar]
- 12.Shapiro F, Bresnan MJ. Orthopaedic management of childhood neuromuscular disease. Part III: Diseases of muscle. J Bone Joint Surg Am 1982;64:1102-7. [Google Scholar]
- 13.O’Brien JP, Dwyer AP, Hodgson AR. Paralytic pelvic obliquity. Its prognosis and management and the development of a technique for full correction of the deformity. J Bone Joint Surg Am 1975;57:626-31. [Google Scholar]
- 14.Zenios M, Sampath J, Cole C, Khan T, Galasko CS. Operative treatment for hip subluxation in spinal muscular atrophy. J Bone Joint Surg Br 2005;87:1541-4. [Google Scholar]
- 15.Thompson CE, Larsen LJ. Recurrent hip dislocation in intermediate spinal atrophy. J Pediatr Orthop 1990;10:638-41. [Google Scholar]