
Recurrent giant cell tumors have to be re-evaluated for malignant changes and in Grade 3 GCTs resection and appropriate reconstruction is the best.
Dr. Raj Milind Sawant, Department of Orthopaedic Surgery, Dr. D. Y. Patil Medical College and Hospital, Navi Mumbai - 400 706, Maharashtra, India. E-mail: rajsawant135@gmail.com
Introduction: The aim of the study was a case report of a right-sided recurrent giant cell tumor of the distal end of the femur.
Methodology: A case of a 25-year-old male patient with a history of recurrent giant cell tumor of the right distal femur who presented with chief complaints of pain over right distal femur and stiffness in the right knee for 2 years with restricted knee movement and is unable to walk. He was diagnosed with recurrent giant cell tumor of the right of the distal femur and was treated with wide excision with mega prosthesis reconstruction.
Result: Wide excision with mega prosthesis reconstruction showed a good functional range of motion with early rehabilitation, stability, and mobility of joints.
Conclusion: We recommend wide excision and reconstruction with mega prosthesis is an effective method compared to sandwich technique and nailing and can be successfully done in the case of recurrent giant cell tumor of the distal femur with a good outcome, functional range of motion, stability, and mobility of the joint with early rehabilitation though it is a technically demanding surgery. The knee joint could have been salvaged and the need for more extensive surgery could have been prevented, had the diagnosis of recurrent giant cell tumor was made earlier.
Keywords: Recurrent giant cell tumor, mega prosthesis , reconstruction, wide excision.
Giant cell tumors are usually primary bone tumors that present usually in the long bones of the body with majority of such tumors usually occurring at locations such as distal femur, proximal tibia, and fibula [1]. In the more aggressive variants of giant cell tumors, patient usually presents with pathological fracture which occurs in around 12% of cases [1]. Giant cell tumor is characterized by the presence of large multinucleated osteoclast- like giant cells, mononuclear spindle-like stromal cells, and monocytes [2]. Knee joint is the most common site of giant cell tumor [3]. Bone resorption usually occurs due to giant cells present in giant cell tumors [3]. Among all primary neoplasms, giant cell tumor constitutes for 5% and among all benign bone tumors, giant cell tumor constitutes for 20% [4]. Pain is the most common presentation of giant cell tumor which occurs due to mechanical instability due to bone resorption [4]. Large bony swelling is usually observed at the local site due to destruction of bone and progression of tumor [4]. The usual location of giant cell tumor is close to the joint due to which there is limitation of range of motion, joint effusion, and synovitis [5]. Patients who present with pathological fracture which is around 12% most commonly indicate a more aggressive disease and a possibility of recurrence after treatment and metastasis in rare cases [6].
We present a case of a 25-year-old male who presented to us with chief complaints of pain over the right distal femur and stiffness in the right knee for 2 years. The patient gives a history of pain in the lateral aspect of the knee in 2017. The pain started increasing gradually over 1 year so he visited an orthopedic surgeon in 2018. The doctor advised him to get an Magnetic resonance imaging (MRI) done on his right knee. Later, patient gave a history of fall from heights of approximately 2–3 feet and his pain aggravated. He took x-rays and MRI after this incident. X-rays were taken by the patient after the fall which were suggestive of the lytic lesion and pathological fracture. MRI done by the patient after the fall was s/o large expansile altered signal intensity lesion in the distal epimetaphysis at the lateral aspect involving the lateral femoral condyle with a pathological fracture through the lesion. The lesion could represent a neoplastic etiology like a giant cell tumor. The patient decided to get operated and on May 27, 2018, he was operated for curettage with cementing and 2 CC screw fixation. The sample removed was sent for histopathological assessment by a reputed musculoskeletal pathologist. Histopathology report was s/o features consistent with giant cell tumor of the bone. Post-operative X-ray was done (Fig. 1a and b).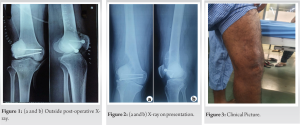 The patient was asked to take serial X-rays at regular intervals. X-rays taken on post-operative 6 months and 3 years showed lytic lesions. After that patient presented to a tertiary care teaching hospital in Navi Mumbai with a chief complaint of pain over the right distal femur and stiffness in the right knee for 2 years. X-rays done on admission show a lytic lesion around the lateral aspect of the distal femur with cementing and 2 cc screws from the previous procedure (Fig. 2a and b). Clinical pictures on admission show swelling and healed surgical scar (Fig. 3). The patient was advised for a CT scan from our side. Furthermore, a fresh MRI was done (Fig. 4a-c). The patient was advised to biopsy the lesion. Biopsy was done from the lesion and sent for histopathological examination-biopsy was s/o giant cell tumor with malignant potential. Since the tumor was suggestive of malignant potential, the patient was advised to undergo a PET scan to rule out metastasis. Pet scan was s/o increased metabolic activity is noted in lytic lesion involving the lateral aspect of the distal femoral metadiaphysis and lateral femoral condyle associated with cortical erosion on the lateral aspect and associated enhancing soft tissue likely neoplastic etiology. A plan of the right distal femur wide excision with mega prosthesis reconstruction was made.
The patient was asked to take serial X-rays at regular intervals. X-rays taken on post-operative 6 months and 3 years showed lytic lesions. After that patient presented to a tertiary care teaching hospital in Navi Mumbai with a chief complaint of pain over the right distal femur and stiffness in the right knee for 2 years. X-rays done on admission show a lytic lesion around the lateral aspect of the distal femur with cementing and 2 cc screws from the previous procedure (Fig. 2a and b). Clinical pictures on admission show swelling and healed surgical scar (Fig. 3). The patient was advised for a CT scan from our side. Furthermore, a fresh MRI was done (Fig. 4a-c). The patient was advised to biopsy the lesion. Biopsy was done from the lesion and sent for histopathological examination-biopsy was s/o giant cell tumor with malignant potential. Since the tumor was suggestive of malignant potential, the patient was advised to undergo a PET scan to rule out metastasis. Pet scan was s/o increased metabolic activity is noted in lytic lesion involving the lateral aspect of the distal femoral metadiaphysis and lateral femoral condyle associated with cortical erosion on the lateral aspect and associated enhancing soft tissue likely neoplastic etiology. A plan of the right distal femur wide excision with mega prosthesis reconstruction was made.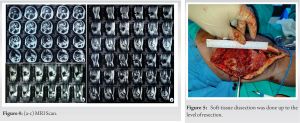 The patient was taken in a supine position under general and epidural anesthesia, parts were prepared and the tourniquet was raised. The lateral approach was taken over the scar of the previous surgery, thick flaps were raised and rectus was identified and isolated, the patella was everted and soft-tissue dissection was done up to the level of resection (Fig. 5). The joint was opened and ligaments were cut along with the posterior capsule, femoral neurovascular bundle was identified and dissected free. Osteotomy was done using a saw and the lesion was excised after clipping feeders. All soft-tissue attachments were cut. A thorough wash was given, hemostasis achieved, and the specimen (Fig. 6a and b) was examined for margins. femur end was prepared after which the tibial end was prepared.
The patient was taken in a supine position under general and epidural anesthesia, parts were prepared and the tourniquet was raised. The lateral approach was taken over the scar of the previous surgery, thick flaps were raised and rectus was identified and isolated, the patella was everted and soft-tissue dissection was done up to the level of resection (Fig. 5). The joint was opened and ligaments were cut along with the posterior capsule, femoral neurovascular bundle was identified and dissected free. Osteotomy was done using a saw and the lesion was excised after clipping feeders. All soft-tissue attachments were cut. A thorough wash was given, hemostasis achieved, and the specimen (Fig. 6a and b) was examined for margins. femur end was prepared after which the tibial end was prepared. 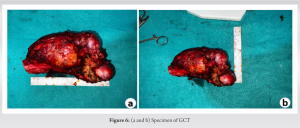 Trial implants were placed and rom was assessed along with stability and limb length. Final implantation was done and again from was assessed along with stability and limb length and was found to be satisfactory (Fig. 7). Cement was set for correct rotation and wash given. The closure is done in layers. Post-operative X-rays were done (Fig. 8a and b). Post-operative day 2 patient was mobilized with a walker. X-rays were repeated post-operative 2 months which showed no evidence of lytic lesions (Fig. 9a and b). Patient has a good range of motion at the knee joint postoperatively which was reassessed on pod 2 months .patient can be seen walking comfortably postoperatively at 2 months. At post-operative 2 months, the patient has a healthy suture line.
Trial implants were placed and rom was assessed along with stability and limb length. Final implantation was done and again from was assessed along with stability and limb length and was found to be satisfactory (Fig. 7). Cement was set for correct rotation and wash given. The closure is done in layers. Post-operative X-rays were done (Fig. 8a and b). Post-operative day 2 patient was mobilized with a walker. X-rays were repeated post-operative 2 months which showed no evidence of lytic lesions (Fig. 9a and b). Patient has a good range of motion at the knee joint postoperatively which was reassessed on pod 2 months .patient can be seen walking comfortably postoperatively at 2 months. At post-operative 2 months, the patient has a healthy suture line.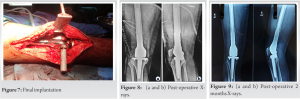
Giant cell tumors are usually found around the knee joint and treatment of giant cell tumors pose a challenge to orthopedic surgeons because the knee joint is one of the most crucial joint in the body as it is a weight bearing joint. Certain characteristics which are commonly seen in giant cell tumors are expansible growth and cortex thinning and this usually presents as a pathological fracture [7, 8]. Giant cell tumor found in distal femur, rarely spread into the knee joint and the negative effect of a giant cell tumor in knee range of motion is most commonly seen. This is the very reason accurate pre-operative planning is essential to reduce the probability of recurrence and improving knee function postoperatively. Various treatment modalities available for giant cell tumor include curettage, cryotherapy, phenol combined with bone grafting, or bone cement. We opted for wide excision with megaprosthesis in our patient. Standard treatment for giant cell tumor includes intralesional curettage of long bones along with use of polymethylmethacrylate. Associated complications of this include high risk of recurrence compared to wide local resection as can be seen in our patient which was missed earlier. The advantage of our method of using a mega prosthesis reconstruction is a lesser chance of recurrence and the patient can start weight bearing and physiotherapy on the next day of surgery. Pitfalls which could have been avoided earlier in this patient would be, biopsy should have been done before curettage by the local doctor. Recurrence should have been picked up early as X-rays showed it clearly by a local doctor. Recurrence could have been prevented had the principles of extended curettage with speed bur followed in the previous surgery. Rebiopsy is necessary for recurrences to rule out sarcomatous changes. Excision should be done with clear margins to prevent sarcomatous changes and metastasis. The drain has to be in the line of incision as scars have to be excised in recurrences.
Wide excision and reconstruction with mega prosthesis is an effective method and can be successfully done in a case of recurrent giant cell tumor of the distal femur with a good outcome, range of motion, stability, and mobility of joint with early rehabilitation though it is a technically demanding surgery.
Always do a biopsy before surgery. Excision with clear margins is of utmost importance as trying to minimize the recurrence is the key to a successful management. Definitive management by Megaprostshesis replacement in these tumors around the knee has given excellent results but are very demanding surgeries requiring skilled surgeons and precision tools.
References
- 1.MacEwan AA, Nanda SN, Mishra D, Tuteja S, Sandeep B. A giant cell tumor of the distal femur managed by excision and knee arthrodesis using a custom made long intramedullary interlocking nail: A case report and review of the literature. Cureus 202;13:e14810. [Google Scholar]
- 2.Chakarun CJ, Forrester DM, Gottsegen CJ, Patel DB, White EA, Matcuk GR Jr. Giant cell tumour of bone: Review, mimics, and new developments in treatment. Radiographics 2013;33:197-211. [Google Scholar]
- 3.Cowan RW, Singh G. Giant cell tumour of bone: A basic science perspective. Bone 2013;52:238-46. [Google Scholar]
- 4.Kalil RK, Amary F. Tumours and Tumour-Like Lesions of Bone. Cham: Springer; 2020. [Google Scholar]
- 5.Turcotte RE. Giant cell tumour of bone. Orthop Clin North Am 2006;37:35-51. [Google Scholar]
- 6.Lewis VO, Wei A, Mendoza T, Primus F, Peabody T, Simon MA. Argon beam coagulation as an adjuvant for local control of giant cell tumour. Clin Orthop Relat Res 2007;454:192-7. [Google Scholar]
- 7.Niu X, Zhang Q, Hao L, Ding Y, Li Y, Xu H, et al. Giant cell tumour of the extremity: Retrospective analysis of 621 Chinese patients from one institution. J Bone Joint Surg Am 2012;94:461-7. [Google Scholar]
- 8.Ayerza MA, Aponte-Tinao LA, Farfalli GL, Restrepo CA, Muscolo DL. Joint preservation after extensive curettage of knee giant cell tumours. Clin Orthop Relat Res 2009;467:2845-51. [Google Scholar]
- 9.Salunke AA, Chen Y, Chen X, Tan JH, Singh G, Tai BC, et al. Does pathological fracture affect the rate of local recurrence in patients with a giant cell tumour of bone?: A meta-analysis. Bone Joint J 2015;97-B:1566-71. [Google Scholar]







