
Prompt diagnosis and management of a rare condition to prevent damage to articular cartilage.
Dr. Nirvin Paul, Department of Trauma Surgery, AIIMS, Rishikesh - 249 203, Uttarakhand, India. E-mail: drnirvinpaul@gmail.com
Abstract
Introduction: Synovial hemangioma is a rare benign condition that is seen predominantly in the adolescent age group. Patients commonly present with pain and swelling of the involved joint. Here, we report a case of recurrent synovial hemangioma in a 10-year-old girl.
Case Report: A 10-year old presented with complaints of recurrent swelling in her right knee of 3 years duration. She had complaints of pain, swelling, and deformity of her right knee. She had undergone a surgery to excise the swelling earlier for similar complaints elsewhere. She remained asymptomatic for a year, after which swelling reappeared.
Conclusion: Synovial hemangioma is a rare benign condition that is often missed and needs to be promptly addressed to prevent damage to the articular cartilage. The chance of recurrence is high.
Keywords: Synovial hemangioma, recurrence, sclerotherapy
Synovial hemangiomas are rare benign lesions that arise in the knee (most common), elbow, wrist, ankle, or synovium of tendon sheaths [1]. The usual age of appearance is adolescence [2]. Patients present with joint pain, fullness, and difficulty in ambulation. Delay in diagnosis is seen if a visible swelling is not present. A missed diagnosis could lead to arthritic joint changes in the future [3]. Here, we describe the evaluation and management of a recurrent synovial hemangioma of the knee in a 10-year-old girl.
A 10-year old presented with complaints of recurrent swelling in her right knee of 3 years duration. She had complaints of pain, swelling, and deformity of her right knee. She had undergone surgery to excise the swelling earlier for similar complaints elsewhere. She remained asymptomatic for a year, after which swelling reappeared. Physical examination revealed a soft lump measuring 3 × 4 cm in the suprapatellar region of her right knee. There was a fixed flexion deformity of 10°. The plain X-ray revealed a poorly defined soft-tissue density over the infrapatellar fat pad. No joint-related changes were seen (Fig. 1). An magnetic resonance imaging (MRI) scan was done which revealed a lobulated hyperintense lesion involving Hoffa’s fat pad, extending from the anterior margin of the patella to the anterior cruciate ligament (ACL) and the menisci. There was a mild cortical irregularity and subchondral marrow edema in the patellofemoral joint (Figs. 2 and 3).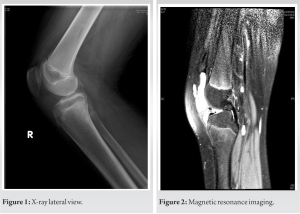 Features of the lesion were suggestive of a hemangioma or a venous malformation. A focussed USG screening was done, in which the anechoic spaces in Hoffa’s fat pad showed vascularity on augmentation, which inclined more toward a venous malformation (Figs. 4 and 5) Other differentials considered were pigmented villonodular synovitis [4]. An excision biopsy was planned. Arthroscopic excision was not considered due to the previous surgical scarring at the same site. A radiology opinion was sought regarding the role of sclerotherapy in managing the lesion; however, since no feeder’s vessels were found, it was not feasible. Hence, an arthrotomy and excision of the lesion were planned. The knee was approached through an anterior midline incision over the previous surgical scar and a medial parapatellar arthrotomy was carriedout.
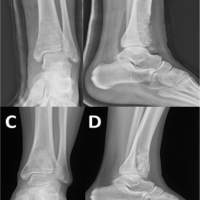
Features of the lesion were suggestive of a hemangioma or a venous malformation. A focussed USG screening was done, in which the anechoic spaces in Hoffa’s fat pad showed vascularity on augmentation, which inclined more toward a venous malformation (Figs. 4 and 5) Other differentials considered were pigmented villonodular synovitis [4]. An excision biopsy was planned. Arthroscopic excision was not considered due to the previous surgical scarring at the same site. A radiology opinion was sought regarding the role of sclerotherapy in managing the lesion; however, since no feeder’s vessels were found, it was not feasible. Hence, an arthrotomy and excision of the lesion were planned. The knee was approached through an anterior midline incision over the previous surgical scar and a medial parapatellar arthrotomy was carriedout.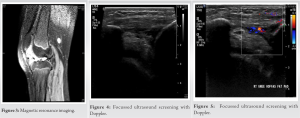 The hemangioma was identified as a brownish tissue filling the anteromedial compartment anterior to the ACL, Hoffa’s fat pad, lateral gutter, and intermeniscal region. The pathological tissue was excised and bleeding points were cauterized after releasing the tourniquet. The knee was splinted with a posterior above knee slab (Fig. 6). Postoperatively, continuous passive mobilization was initiated, starting at 30°, and gradually increasing over the following 3 weeks. Three months postoperatively, the child had a range of motion of 10°–135° and grade 4 quadriceps power. The wounds healed well without complications.
The hemangioma was identified as a brownish tissue filling the anteromedial compartment anterior to the ACL, Hoffa’s fat pad, lateral gutter, and intermeniscal region. The pathological tissue was excised and bleeding points were cauterized after releasing the tourniquet. The knee was splinted with a posterior above knee slab (Fig. 6). Postoperatively, continuous passive mobilization was initiated, starting at 30°, and gradually increasing over the following 3 weeks. Three months postoperatively, the child had a range of motion of 10°–135° and grade 4 quadriceps power. The wounds healed well without complications.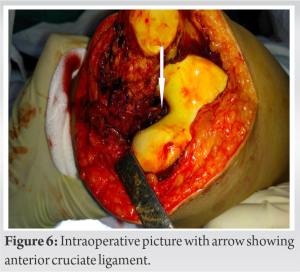
Synovial hemangioma was first described by Bouchut [5] in 1856 and it commonly affects the knee joint and involves the wrist, elbow, temporomandibular joint, and synovium of tendon sheaths less often [1]. They often present before the age of 16 due to hemorrhage into the joint from trivial traumaor spontaneously [3,6]. Clinical presentation is mainly pain, swelling, and recurrent hemarthrosis. They can also present with mechanical symptoms of the knee mimicking internal derangement of the knee joint [7]. It is classified based on the size and type of vessel that is seen mainly in the lesion. They are classified as cavernous which has predominantly large vessels (50%), capillary (25%), venous (5%), and arteriovenous (20%) [6,7]. They are also classified as intraarticular, juxta-articular, and intermediate based on their anatomical location [3,7]. Differential diagnosis includes pigmented villonodular synovitis, synovial chondromatosis, and osteochondromatosis [6]. It is an easily missed condition [8] that can lead to permanent joint damage if left undiagnosed for a prolonged period. Every child presenting with knee pain or fullness will benefit from further evaluation with an MRI which is the investigation of choice [6]. An ultrasonogram would provide additional information in case of a venous malformation [6]. Recurrences can occur even with an apparent complete resection [9]. Even though arthroscopic resection has been described, it is reserved for patients with bleeding disorders. Sclerosing agents are damaging to articular cartilage [10].
Open resection is the management of choice in intraarticular hemangiomas, as it allows adequate visualization to enable thorough excision. Sclerotherapy is not an advisable treatment option.
Synovial hemangioma is a rare benign condition of adolescent age that needs to be promptly diagnosed and treated with open resection.
References
- 1.Larsen IJ, Landry RM. Hemangioma of the synovial membrane. J Bone Joint Surg Am 1969;51:1210-5. [Google Scholar | PubMed]
- 2.Wen DW, Tan TJ, Rasheed S. Synovial haemangioma of the knee joint: An unusual cause of knee pain in a 14-month old girl. Skeletal Radiol 2016;45:827-31. [Google Scholar | PubMed]
- 3.Ramseier LE, Exner GU. Arthropathy of the knee joint caused by synovial hemangioma. J Pediatr Orthop 2004;24:83-6. [Google Scholar | PubMed]
- 4.Huang GS, Lee CH, Chan WP, Chen CY, Yu JS, Resnick D. Localized nodular synovitis of the knee: MR imaging appearance and clinical correlates in 21 patients. AJR Am J Roentgenol 2003;181:539-43. [Google Scholar | PubMed]
- 5.Bouchut E. Tumeur erectile de l’articulation dugenou. Gaz Hop Paris 1856;29:379. [Google Scholar | PubMed]
- 6.Greenspan A, McGahan JP, Vogelsang P, Szabo RM. Imaging strategies in the evaluation of soft-tissue hemangiomas of the extremities: Correlation of the findings of plain radiography, angiography, CT, MRI, and ultrasonography in 12 histologically proven cases. Skeletal Radiol 1992;21:11-8. [Google Scholar | PubMed]
- 7.Akgün I, Kesmezacar H, Oğüt T, Dervişoğlu S. Intra-articular emangioma of the knee. Arthroscopy 2003;19:E17. [Google Scholar | PubMed]
- 8.Cotten A, Flipo RM, Herbaux B, Gougeon F, Lecomte-Houcke M, Chastanet P. Synovial haemangioma of the knee: A frequently misdiagnosed lesion. Skeletal Radiol 1995;24:257-61. [Google Scholar | PubMed]
- 9.Pireau N, Boon LM, Poilvache P, Docquier PL. Surgical treatment of intra-articular knee venous malformations: When and how? J Pediatr Orthop 2016;36:316-22 [Google Scholar | PubMed]
- 10.Dompmartin A, Vikkula M, Boon LM. Venous malformation: Update on aetiopathogenesis, diagnosis and management. Phlebology 010;25:224-35 [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2024 Response of Recurrent Aggressive Aneurysmal Bone Cyst of Distal Tibia to Denosumab Treatment
June 10, 2024 Response of Recurrent Aggressive Aneurysmal Bone Cyst of Distal Tibia to Denosumab Treatment January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation
January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation October 1, 2025 Giant Cell Tumor of the Tendon Sheath: Case Series and Review of Literature
October 1, 2025 Giant Cell Tumor of the Tendon Sheath: Case Series and Review of Literature September 1, 2025 A Rare Case of Intraosseous Venous Malformation of Tibia in a Young Female – A Diagnostic Dilemma
September 1, 2025 A Rare Case of Intraosseous Venous Malformation of Tibia in a Young Female – A Diagnostic Dilemma