
• Creating awareness about the simplicity of the treatment modality depending on the grade of the Amniotic Band • Reporting the most common presentation type and its association with CTEV. • Nature of its complex presentation and the serial correction of the constriction bands before correction of the talipes equino varus deformity.
Dr. Sajid Salman, Department of Orthopaedics, Princess Esra Hospital, 1-2-36/2, Street No. 4, Habsiguda, Hyderabad - 500007, Telangana, India. E-mail: sajid.salman4@live.com
Abstract
Introduction: The term Streeter’s syndrome is a term used to describe rare ongenital malformations that includes a variety of clinical presentations usually consisting of a constriction band around a part of the body which can be as superficial as involving just the skin which can be only cosmetic and asymptomatic or can be as deep as causing restricted circulation distally which may be in incompatible with life. Such conditions are remarkably rare accounting for an incidence range from 1:1.2 k to 1: 15 k live births and 178:10 k spontaneous abortions [1]. Males and females are uniformly affected. Almost all cases are sporadic; extremely rare evidence of familial transmission. The entity has been described in the literature in 34 different terms, (such as amniotic rupture sequence, ADAM complex, constriction band syndrome, Streeter’s dysplasia, etc.) due to its extremely variable clinical features and lack of understanding of the etiology. This results in a lack of understanding and creates unnecessary stress for the surgeon/physician as well as the parents.
Case Report: We discuss case reports of two such cases with their simple nature of treatment with their outcomes.
Conclusion: There is a significant deficit in the education of cases with low incidence, such is the case with pediatric patients presenting with amniotic bands, which usually present and are associated with Congenital Talipes Equino Varus deformity. In such cases, improper or incorrect treatment and/or neglect of the constriction may lead to the vascular deficit and eventually auto-amputation of the segment distal to the amniotic band.
Keywords: Amniotic band syndrome, amniotic rupture sequence, ADAM complex, constriction band syndrome, Streeter’s dysplasia, constriction band.
Amniotic constriction band represents a collection of congenital malformations characterized by extreme variability in the clinical presentation that ranges from simple ring constriction to the anomalies that render life incompatible [2]. It is a term used to describe rare congenital malformations that includes a variety of clinical presentations usually consisting of a constriction band around a part of the body which can be as superficial as involving just the skin which can be only cosmetic and asymptomatic or can be as deep as causing restricted circulation distally which may be in incompatible with life. The incidence ranges from 1:1,200 to 1: 15,000 live births and 178:10,000 spontaneous abortions. Males and females are uniformly affected [2]. Almost all cases are sporadic; extremely rare evidence of them being hereditary. Most cases are non-genetic, and there is no recurrence in siblings or children of affected adults[3]. The entity has been chronicled in literature in 34 different terms, (such as amniotic rupture sequence, ADAM complex, constriction band syndrome, Streeter’s dysplasia, etc.) due to its extremely variable clinical features and lack of understanding of the etiology [4]. Such anomalies are usually associated with gross developmental delay of the child. The etiology of Streeter’s syndrome has been a debate for as long as this entity has been initially described 9 decades ago. The most accepted theory proposed by Torpin [5] is that of amniotic disruption. The theory suggests that following an event of amniotic rupture in-utero, there occurs eviction of all or parts of the fetus into the chorionic cavity. As the fetus grows, this eventually causes compression and the extruded fetal limbs or body parts are entwined with the puckered remnants of the broken amnion. The presentation usually depends on the timing of such an event, and the amount of compression of the fetal structures. Where in early fetal age, that is, before 45 days of fetal age or gestation, extreme defects of the brain and cranium and varying degrees of neurological insults and associated with facial clefts have been described and in damage occurring in later fetal ages, that is, beyond 45 days limb involvement is seen usually without any central neurological involvement as described by Higginbottom et al. [6].
Classification and grading of Streeter’s syndrome Patterson classification system [7]
• Category 1: Uncomplicated constriction rings
• Category 2: Rings with associated deformity of the distal part that with or without lymphedema
• Category 3: Constriction rings with Acrosyndactyly and is further split into three types based on the involvement of web formation between fingers
• Category 4: Children with intrauterine amputation due to the extent of the constriction.
Treatment options available
Depending on the time of prenatal presentation and analysis, fetal surgery is a viable option for constriction bands which have been observed prenatally to obstruct the blood flow to the distal unit which may eventually cause in-utero amputation. In the Postnatal period, the baby may need reconstructive surgery depending on the extent of the residual deformity which ranges from minor to complicated.[8]
Non-operative
Type 1: Uncomplicated constriction ring with no Compromise to the circulation.
Operative
1. Excision/Release of constriction band: Type-1 with compromised distal circulation
2. Circumferential Z Plasties: Type-2; distal deformities present
3. Surgical release of syndactyly: Type-3 with distal fusions
4. Reconstruction of involved digits or limb: Type-4 to improve function.
Presented are the two cases with the variable extent of involvement. Both were delivered by vaginal delivery and no antenatal diagnosis.
1. Case 1: Male baby with bilateral lower limb involvement. The left side was Type II (associated CTEV) and the right side was Type I. Two parallel constricting bands, occurring over the ankle of the right lower limb with one at the base of great toe which was associated with edema and no vascular insufficiency. Brachydactylic digits and amputation of the fifth digit were also observed.(Fig. 1)
2. Case 2: Male baby with bilateral lower limb involvement. The left side was type II (associated with CTEV) and the right side was Type IV (near total amputation- gangrenous). There was associated bowing of the tibia and fibula on the left side. Both patients were evaluated for other joints and system involvement, and there were no other anomalies found.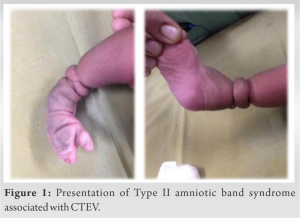
Doppler examination of CTEV-affected limbs revealed
Anterior tibial artery narrowing in caliber distal to constriction band. The absence of color flow along posterior tibial artery (PTA) and distal PTA color filling is seen through large musculo collateral. Dorsalis pedis artery is normal in caliber.
Treatment
Case 1
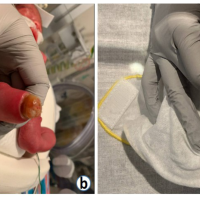
Two staged (180°) releases of the constriction band performed by initially identifying the depth of the band, and releasing any entwined soft tissue structures followed by excising it and approximation of the edges.(Fig. 2) on the right side with 3 weeks intervals performed. This was followed by CTEV correction by the Ponseti technique of manipulation. The correction was obtained after five casts and maintained on the Abduction splint. No intervention was done on the left lower limb.(Fig. 3).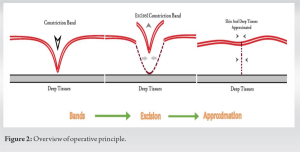
Case 2
The operative procedure performed was below-knee amputation on the right side and two staged (180°) release of constriction band on the left side. This was followed by serial manipulation by the Ponseti technique for CTEV and final percutaneous Tendo Achilles tenotomy. The correction was maintained on Ankle Foot Orthosis.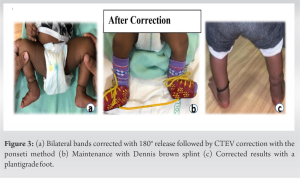
Streeter’s syndrome is a rare condition, as among all the body malformations, it accounts for –1–2%, less common in the lower limb (15% of ABS). The typical feature of ACB is the involvement of multiple extremities at different levels and degrees, mostly presenting as to cause limb or digit amputations, arachnodactyly, or simple constriction rings and other deformities [9]. The management is staged wise, partial release, and repeat of surgery to avoid vascular complications [10]. Antenatal diagnosis can be missed if of low grade, with the advance of fetal surgery in the future, if diagnosed in the antenatal period, debilitating complications like auto amputation can be avoided after a timely intervention. Especially if associated with CTEV or other deformities, it needs to be treated early, so that plaster cast application can be done.[11]. Special care needs to take as there is a high risk of compression and distal edema due to poor lymphatic and venous drainage.
ACB encompasses a variety of rare congenital abnormalities with diverse clinical presentations that are unique to each patient. Surgeons and clinicians should be acquainted with the range of clinical presentations that are possible for ABS and should consider this entity in the differential diagnosis for asymmetrical malformations of the extremities, face, or body wall. The patient needs customized stage-wise intervention with unpredictable outcomes[9]. The parents must be made advised of all the possibilities to avoid undue complications, and notified about the nature of the disease, to unburden them with superstitious beliefs existing in minds of grandparents, and to explain clearly the potential difficulties with rehabilitation.
ACB is a condition that needs more widespread recognition for its various and complex presentations. Depending on the type of the constriction band, the release can either be done in a stage-wise manner or it can be done as a complete release. The stage-wise release offers the surgeon for better healing of the surgical site with fibrosis and does not in turn create a new constriction while healing, defeating the purpose of the intervention. Complications of such an entity can be devastating and may lead to auto-amputation of the distal segment by hampering the blood supply which should always be investigated with an arterial and venous Doppler at first contact. With the simple release of the band superficially, we aim to restore the hindered blood supply and reduce the risk of auto-amputation. This should be explained to the parents as there is widespread superstition over such an entity. Other joints and extremities should be examined for identifying the presence of such an entity which requires prompt diagnosis before the development of a complication.
References
- 1.Richardson S, Khandeparker RV, Pellerin P. Amniotic constriction band: A report of two cases with unique clinical presentations. J Korean Assoc Oral Maxillofac Surg 2017;43:171-7. [Google Scholar | PubMed]
- 2.Cilogu NS, Gumus N. A rare form of congenital amniotic band syndrome: Total circular abdominal constriction band. Arch Plast Surg 2014;41:290-1. [Google Scholar | PubMed]
- 3.Matic A, Komzec J. Amniotic band syndrome. Acta Med Medianae 2009;48:44-8. [Google Scholar | PubMed]
- 4.Barros M, Gorgal G, Machado AP, Ramalho C, Matias A, Montenegro N. Revisiting amniotic band sequence: A wide spectrum of manifestations. Fetal Diagn Ther 2014;35:51-6. [Google Scholar | PubMed]
- 5.Torpin R. Amniochorionic mesoblastic fibrous strings and amnionic bands: associated constricting fetal malformations or fetal death. Am J Obstet Gynecol 1965;91:65-75. [Google Scholar | PubMed]
- 6.Higginbottom MC, Jones KL, Hall BD, Smith DW. The amniotic band disruption complex: Timing of amniotic rupture and variable spectra of consequent defects. J Pediatr 1979;95:544-9. [Google Scholar | PubMed]
- 7.Hung NN. Congenital constriction ring in children: sine plasty combined with removal of fibrous groove and fasciotomy. J Child Orthop. 2012 Jul;6(3):189-97. [Google Scholar | PubMed]
- 8.Goldfarbb CA, Sathienkijkanchai A, Robin NH. Amniotic constriction band: A multidisciplinary assessment of etiology and clinical presentation. J Bone Joint Surg Am 2009;91 Suppl 4:68-75. [Google Scholar | PubMed]
- 9.Koskimies E, Syvänen J, Nietosvaara Y, Mäkitie O, Pakkasjärvi N. Congenital constriction band syndrome with limb defects. J Pediatr Orthop 2015;35:100-3. [Google Scholar | PubMed]
- 10.Cignini P, Giorlandino C, Padula F, Dugo N, Cafa EV, Spata A. Epidemiology and risk factors of amniotic band syndrome, or ADAM sequence. J Prenatal Med 2012;6:59-63. [Google Scholar | PubMed]
- 11.Daya M, Makakole M. Congenital vascular anomalies in amniotic band syndrome of the limbs. J Pediatr Surg 2011;46:507-13. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2024 Club Foot with Contralateral Congenital Amniotic Band Syndrome Amputation Successfully Treated with Ponseti Method: Case Report
September 1, 2024 Club Foot with Contralateral Congenital Amniotic Band Syndrome Amputation Successfully Treated with Ponseti Method: Case Report April 10, 2024 Reviewers Acknowledgement & Photo Gallery April 2024
April 10, 2024 Reviewers Acknowledgement & Photo Gallery April 2024 May 10, 2021 Outcome of Neglected Versus Treated Tuberculous Dactylitis in the Same Patient – A case report
May 10, 2021 Outcome of Neglected Versus Treated Tuberculous Dactylitis in the Same Patient – A case report June 9, 2021 Unusual Combination of Hip Dislocation with Ipsilateral Femoral Neck and Acetabulum Fracture: A Rare Case Report
June 9, 2021 Unusual Combination of Hip Dislocation with Ipsilateral Femoral Neck and Acetabulum Fracture: A Rare Case Report