Robotic-assisted total knee arthroplasty for osteoarthritis with windswept deformity.
Dr. Takao Kaneko, Department of Orthopedic, Ichinomiya Onsen Hospital, Adult Reconstruction Center, Japan. E-mail: takao-knee@oha.toho-u.ac.jp
Introduction: Windswept deformity (WD) refers to valgus deformity in one knee and varus deformity in the other. We performed robotic-assisted (RA) total knee arthroplasty (TKA) for osteoarthritis of the knee with WD, made patient reported outcome measurements (PROMs), and performed gait analysis based on triaxial accelerometery.
Case Report: A 76-year-old woman presented to our hospital with bilateral knee pain. Image-free handheld RA TKA was performed on the left knee with severe varus deformity and severe pain during walking. RA TKA was performed on the right knee with severe valgus deformity 1 month later. The RA technique was used to determine implant positioning and the plan for osteotomy intraoperatively, taking into account soft-tissue balance. This made it possible to use a posterior stabilized implant instead of a semi-constrained implant for severe valgus knee deformity with flexion contracture (Krachow classification Type 2). At 1 year after TKA, PROMs were inferior in the knee with pre-operative valgus deformity. Gait ability improved after surgery. Even with the RA technique, it took 8 months to achieve left-right balance while walking and for the variability of the gait cycle to become equivalent to that of a normal knee.
Conclusion: Primary RA TKA is a viable option for osteoarthritis of the knee with WD. It took time for the gait ability of both knees to become equal and PROMs were better with the varus deformity compared to before surgery.
Keywords: Windswept deformity, robotic assisted total knee arthroplasty, patient reported outcome measurements, triaxial accelerometer, gait ability.
Windswept’ deformity (WD) refers to valgus deformity in one knee and a varus deformity in the other [1]. Current developments in robotic-assisted (RA) surgical techniques give surgeons intraoperative options for total knee arthroplasty (TKA) that improve accuracy [2, 3]. There have been no reports of primary RA TKA for WD. We performed RA TKA for osteoarthritis of the knee with WD and assessed patient reported outcome measurements (PROMs) and the changes in gait ability over time.
A 76-year-old woman with a body mass index of 20.9 kg/m2 with bilateral knee pain visited our hospital. Pre-operative characteristics of the patient are shown in Table 1. Preoperatively, the right knee had valgus deformity Krakow classification Type 2 [4] and the left knee had varus deformity (Kellgren-Lawrence classification Grade 4) (Fig. 1). 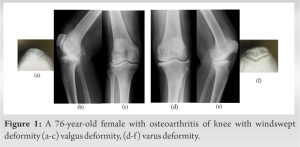 For pre-operative planning, component alignment and osteotomy volume were planned using three-dimensional computed tomography (3DCT) data of the entire limb. The goal was to achieve post-operative mechanical alignment using ZedView (ZedKnee; LEXI Co., Ltd., Tokyo, Japan). RA TKA was performed on the left knee, which was painful upon walking and on the right. RA TKA was performed on the right knee 1 month later.
For pre-operative planning, component alignment and osteotomy volume were planned using three-dimensional computed tomography (3DCT) data of the entire limb. The goal was to achieve post-operative mechanical alignment using ZedView (ZedKnee; LEXI Co., Ltd., Tokyo, Japan). RA TKA was performed on the left knee, which was painful upon walking and on the right. RA TKA was performed on the right knee 1 month later. 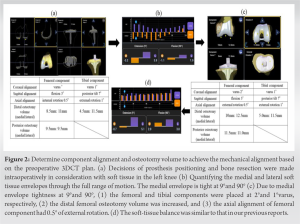 Both procedures were performed with the medial subvastus approach. The Blue Belt Navio surgical system (Navio; Smith and Nephew, Plymouth, MN, USA) was used for image-free handheld RA surgery. We followed the methods of Kaneko et al. 2021 [5]. Planning of prosthesis position and bone resection was done intraoperatively with consideration of soft tissue balance. The osteophytes on the femur, tibia, and intercondylar were resected. Tracker fixation of the femur was proximal and anterior to the medial epicondyle and mid-shaft femur. Tracker fixation of the tibia was from the anteromedial tibia to 6 cm from the incision using bury pin threads (4.0 mm). Landmark registration, ROM testing, varus-valgus stress test, and mapping of the anatomy of the femoral condyle and tibial plateau were performed by “painting” the surfaces with an optical probe. A virtual model of the knee was thus created. Planning for prosthesis size, alignment, and position, as well as the volume of bone removal, were determined intraoperatively by the surgeon. Arthritic cartilage and bone were then methodically removed using a handheld sculptor. The RA surgical technique continuously tracked the position of the patient’s lower limb and the progress of bone resection with a navigation system camera. Decisions about prosthesis and bone resection volume was made intraoperatively in consideration of the soft tissue in the left and right knee (Fig. 2 and 3).
Both procedures were performed with the medial subvastus approach. The Blue Belt Navio surgical system (Navio; Smith and Nephew, Plymouth, MN, USA) was used for image-free handheld RA surgery. We followed the methods of Kaneko et al. 2021 [5]. Planning of prosthesis position and bone resection was done intraoperatively with consideration of soft tissue balance. The osteophytes on the femur, tibia, and intercondylar were resected. Tracker fixation of the femur was proximal and anterior to the medial epicondyle and mid-shaft femur. Tracker fixation of the tibia was from the anteromedial tibia to 6 cm from the incision using bury pin threads (4.0 mm). Landmark registration, ROM testing, varus-valgus stress test, and mapping of the anatomy of the femoral condyle and tibial plateau were performed by “painting” the surfaces with an optical probe. A virtual model of the knee was thus created. Planning for prosthesis size, alignment, and position, as well as the volume of bone removal, were determined intraoperatively by the surgeon. Arthritic cartilage and bone were then methodically removed using a handheld sculptor. The RA surgical technique continuously tracked the position of the patient’s lower limb and the progress of bone resection with a navigation system camera. Decisions about prosthesis and bone resection volume was made intraoperatively in consideration of the soft tissue in the left and right knee (Fig. 2 and 3). 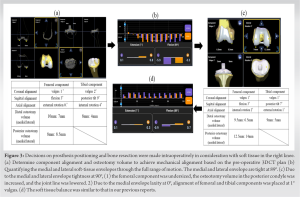 Bicruciate stabilized TKA was performed on the left knee (Journey II BCS; Smith and Nephew. Inc., Memphis, TN, USA) to induce medial pivot movement. For the right knee, LESION posterior stabilized (PS) TKA (Smith and Nephew. Inc., Memphis, TN, USA) was performed (Fig. 4).
Bicruciate stabilized TKA was performed on the left knee (Journey II BCS; Smith and Nephew. Inc., Memphis, TN, USA) to induce medial pivot movement. For the right knee, LESION posterior stabilized (PS) TKA (Smith and Nephew. Inc., Memphis, TN, USA) was performed (Fig. 4).  TKA treatment of valgus deformity is associated with more frequent use of ligament releases and semi-constrained implants and with lower outcome scores than TKA treatment for varus deformity [6, 7, 8]. However, in this case, the patient had Krachow classification Type 2 disease, that is, failure of the medial support mechanism and lateral bone loss as well as failure of support mechanism. Osteotomy and component placement with RA TKA achieved tightness of the medial soft-tissue envelope and laxity of the lateral soft-tissue envelope, which allowed us to avoid using a semi-constrained prosthesis. In other words, planning and bone resection occurred intraoperatively with consideration of soft-tissue balance. On the 1st day after surgery, the drainage tube was removed and physical therapy was initiated. A physical therapist started isometric strength exercises for the quadriceps and ROM exercises for the knee joint. Full weight-bearing was not restricted and patients were allowed to walk with or without assistive devices. The patient followed the same post-operative rehabilitation protocol. Post-operative CT scans were obtained at 4 weeks for both knees. Using reference points, pre-operative CT images were fused to post-operative images automatically by matching bone surfaces. After matching, the femoral-tibial component template from a computer- aided design model was superimposed on the implant image manually to match their contours. Based on the positioning of the templates, the coronal, sagittal, and axial alignments of both components were measured using ZedView with reference to the coordinate system. The post-operative femorotibial angle (FTA) was also measured as the leg axis between the anatomical axis of the femur and tibia in the coronal plane defined by the coordinate systems. The post-operative 3DCT images of the femur and tibia were superimposed onto those of the pre-operative 3DCT plan using ZedView software (Fig. 5) [9, 10, 11, 12].
TKA treatment of valgus deformity is associated with more frequent use of ligament releases and semi-constrained implants and with lower outcome scores than TKA treatment for varus deformity [6, 7, 8]. However, in this case, the patient had Krachow classification Type 2 disease, that is, failure of the medial support mechanism and lateral bone loss as well as failure of support mechanism. Osteotomy and component placement with RA TKA achieved tightness of the medial soft-tissue envelope and laxity of the lateral soft-tissue envelope, which allowed us to avoid using a semi-constrained prosthesis. In other words, planning and bone resection occurred intraoperatively with consideration of soft-tissue balance. On the 1st day after surgery, the drainage tube was removed and physical therapy was initiated. A physical therapist started isometric strength exercises for the quadriceps and ROM exercises for the knee joint. Full weight-bearing was not restricted and patients were allowed to walk with or without assistive devices. The patient followed the same post-operative rehabilitation protocol. Post-operative CT scans were obtained at 4 weeks for both knees. Using reference points, pre-operative CT images were fused to post-operative images automatically by matching bone surfaces. After matching, the femoral-tibial component template from a computer- aided design model was superimposed on the implant image manually to match their contours. Based on the positioning of the templates, the coronal, sagittal, and axial alignments of both components were measured using ZedView with reference to the coordinate system. The post-operative femorotibial angle (FTA) was also measured as the leg axis between the anatomical axis of the femur and tibia in the coronal plane defined by the coordinate systems. The post-operative 3DCT images of the femur and tibia were superimposed onto those of the pre-operative 3DCT plan using ZedView software (Fig. 5) [9, 10, 11, 12]. 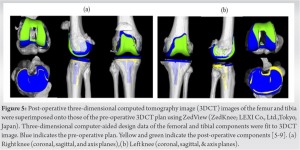 The patient was evaluated at 1 year after TKA using 2011 Knee Society Score (symptom, patient satisfaction, patient expectation, and activity) [13] and the range of motion of the knee. Westren ontario and macmaster universities osteoarthritis index (WOMAC) Score was used to assess pain, stiffness, and daily activity) [14]. Forgotten Joint Score-12 was used [15]. The coordinate system can be set according to the mechanical axes. Using the coordinate system, alignment measurements in accurate coronal, sagittal, and axial planes for the femoral and tibial mechanical axes can be accomplished. 3DCT measurements of the position of components can be used to evaluate the alignment of components and the leg-axis angle. Gait analysis was performed before and after surgery using a triaxial accelerometer (AYUMI EYE; Waseda Elderly Health, Inc., Association). The AYUMI EYE device can score the gait function instantly, based on acceleration data during walking, using a triaxial accelerometer and a gait cycle extraction program embedded in an iOS application (Fig. 6) [16].
The patient was evaluated at 1 year after TKA using 2011 Knee Society Score (symptom, patient satisfaction, patient expectation, and activity) [13] and the range of motion of the knee. Westren ontario and macmaster universities osteoarthritis index (WOMAC) Score was used to assess pain, stiffness, and daily activity) [14]. Forgotten Joint Score-12 was used [15]. The coordinate system can be set according to the mechanical axes. Using the coordinate system, alignment measurements in accurate coronal, sagittal, and axial planes for the femoral and tibial mechanical axes can be accomplished. 3DCT measurements of the position of components can be used to evaluate the alignment of components and the leg-axis angle. Gait analysis was performed before and after surgery using a triaxial accelerometer (AYUMI EYE; Waseda Elderly Health, Inc., Association). The AYUMI EYE device can score the gait function instantly, based on acceleration data during walking, using a triaxial accelerometer and a gait cycle extraction program embedded in an iOS application (Fig. 6) [16]. 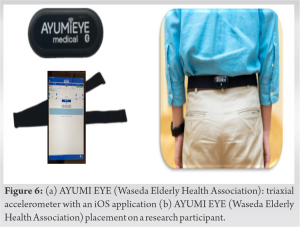 The program predicts the durations of the subsequent stride cycles based on foot contacts detected through a segmentation algorithm. In gait analysis using an accelerometer, the gait motion is considered a periodic movement of the body’s center of gravity (COG), and the rhythmic change in COG is measured using an accelerometer, which allows for objective measurements of gait abnormalities [17, 18, 19].
The program predicts the durations of the subsequent stride cycles based on foot contacts detected through a segmentation algorithm. In gait analysis using an accelerometer, the gait motion is considered a periodic movement of the body’s center of gravity (COG), and the rhythmic change in COG is measured using an accelerometer, which allows for objective measurements of gait abnormalities [17, 18, 19].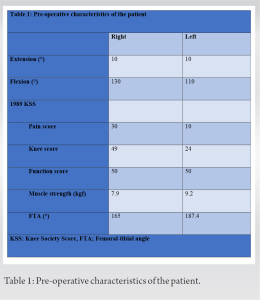 Flexion contracture decreased in both knees after surgery. The flexion angle of the left knee improved after surgery, but the flexion angle of the right knee worsened after surgery (Table 2).
Flexion contracture decreased in both knees after surgery. The flexion angle of the left knee improved after surgery, but the flexion angle of the right knee worsened after surgery (Table 2). 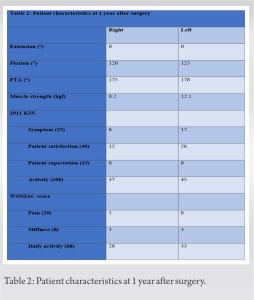 The quadriceps muscles were stronger on the left than the right, both before and after surgery (Table 2). Pre-operative varus or valgus deformity became milder after surgery as well (Table 2). The 2011 KSS patient satisfaction score and the WOMAC stiffness score were equivalent for the left and right knees, but the left knee was superior to the right knee in all other categories at 1 year after surgery (Table 2). Walking speed and stride length were higher at 8 months after surgery compared to before surgery (Table 3). Root mean square, a measure of body sway to the left or right, decreased after surgery. The Time Up and Go test score improved after surgery (Table 3).
The quadriceps muscles were stronger on the left than the right, both before and after surgery (Table 2). Pre-operative varus or valgus deformity became milder after surgery as well (Table 2). The 2011 KSS patient satisfaction score and the WOMAC stiffness score were equivalent for the left and right knees, but the left knee was superior to the right knee in all other categories at 1 year after surgery (Table 2). Walking speed and stride length were higher at 8 months after surgery compared to before surgery (Table 3). Root mean square, a measure of body sway to the left or right, decreased after surgery. The Time Up and Go test score improved after surgery (Table 3). 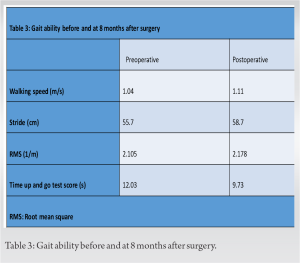 Preoperatively, the patient had left-right swaying while walking. She was walking on frosted feet. The gait was unchanged at 2 months after surgery. It remained unbalanced at 4 and 6 months after surgery. The gait became symmetrical and stable at 8 months after surgery (Fig. 7). Variation over a single gait cycle, that is, gait rhythm, was lower at 8 months after surgery than before surgery (Fig. 8).
Preoperatively, the patient had left-right swaying while walking. She was walking on frosted feet. The gait was unchanged at 2 months after surgery. It remained unbalanced at 4 and 6 months after surgery. The gait became symmetrical and stable at 8 months after surgery (Fig. 7). Variation over a single gait cycle, that is, gait rhythm, was lower at 8 months after surgery than before surgery (Fig. 8).
We performed RA TKA for osteoarthritis of the knee with WD. The pre-operative deformity of the valgus knee was more severe than of the varus knee in terms of PROMs (except for the 2011 KSS patient expectation score and the WOMAC stiffness score) at 1 after TKA. In addition, the valgus knee was inferior to the varus knee in terms of improvement in quadriceps muscle strength at 1 year after TKA. Gait ability improved after surgery, but even with the RA technique, it took 8 months to achieve left-right balance while walking and for the variability of the gait cycle to become equivalent to that of a normal knee. However, the use of RA technology to treat WD has some greatest advantages. To plan for the desired soft-tissue laxity with the RA technique, varus or valgus stress is applied to tension the soft tissues on the sides of the knee through a full range of flexion. This helps the surgeon plan for implant positioning and volume bone resection, taking into account “virtual” soft-tissue laxity before making any cuts [20, 21, 22, 23]. Similarly, we were able to determine the positioning of the prosthesis and plan for osteotomy intraoperatively to ensure the lack of medial laxity while taking soft-tissue balance into account. Krachow et al. 1991 [4] classified valgus deformity of the knee into three types. Type I was defined as valgus deformity secondary to bone loss in the lateral compartment and soft-tissue contracture with intact medial soft tissue. Type II was defined as obvious attenuation of the medial capsular ligament complex. Type III was defined as severe valgus deformity with valgus malpositioning of the proximal tibial joint line after proximal tibial osteotomy with overcorrection. This patient’s deformity was not passively correctable with the varus test. Ligament release and semi-constrained implants are more frequently used in TKA treatment of Krachow classification Type 2 or severe valgus knee [6, 7, 8]. There has been a report of revision surgery due to medial soft-tissue laxity [24]. In this case, osteotomy volume and component alignment were determined intraoperatively so that the medial soft tissue envelope would be loose and the lateral soft tissue envelope would not be stiff during extension, which allowed us to use a PS implant instead of a semi-constrained implant. On the other hand, Howell et al. 2021 [25] reported that cruciat-retaining implants can be used with calipered kinematically alignment TKA in most patients with WD with comparable outcomes scores and alignment in the paired varus and valgus deformities. Regarding reports that the use of RA technology contributes to rehabilitation, the RA lateral unicompartmental knee arthroplasty (UKA) resulted in significantly faster return to sport compared to conventional jig-based UKA [26] and robotic-arm assisted TKA (MAKO: robotic interactive orthopedic arm system, Stryker, Fort Lauderdale, Florida, USA) had significantly improved 2-year post-operative r- physical function, compared with the conventional jig-based TKA [27].
Primary RA TKA is a viable option for osteoarthritis of the knee with WD. It took time for the gait ability of both knees to become equal and PROMs were better with the varus deformity compared to before surgery. Long follow-up is needed.
Robotic-assisted total knee arthroplasty for osteoarthritis of the knee with wind swept deformity showed inferior pre-operative deformity in valgus compared with varus at 1 year postoperatively, and it took 8 months for the left-right balance and gait cycle variability during walking to become comparable to that of the normal knee.
References
- 1.Meding JB, Anderson AR, Ritter MA, Faris PM, Keating EM. Windswept deformity in bilateral total knee arthroplasty. J Arthroplasty 2000;15:562-6. [Google Scholar]
- 2.Lonner JH, Smith JR, Picard F, Hamlin B, Rowe PJ, Riches PE. High degree of accuracy of a novel image-free handheld robot for unicondylar knee arthroplasty in a cadaveric study. Clin Orthop Relat Res 2015;473:206-12. [Google Scholar]
- 3.Batailler C, White N, Ranaldi FM, Neyret P, Servien E, Lustig S. Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2019;27:1232-40. [Google Scholar]
- 4.Krachow KA, Jones MM, Teeny SM, Hungerford DS. Primary total knee arthroplasty in patients with fixed valgus deformity. Clin Orthop Relat Res 1991;273:9-18. [Google Scholar]
- 5.Kaneko T, Igarashi T, Takada T, Yoshizawa S, Ikegami H, Musha Y. Robotic-assisted total knee arthroplasty improves the outlier of rotational alignment of the tibial prosthesis using 3DCT measurements. Knee 2021;31:64-76. [Google Scholar]
- 6.Mazzotti A, Perna F, Golinelli D, Quattrini I, Stea S, Bordini B, et al. Preoperative valgus deformity has twice the risk of failure as compared to varus deformity after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2019;27:3041-7. [Google Scholar]
- 7.Peters CL, Jimenez C, Erickson J, Anderson MB, Pelt CE. Lessons learned from selective soft-tissue release for gap balancing in primary total knee arthroplasty: An analysis of 1216 consecutive total knee arthroplasties: AAOS exhibit selection. J Bone Joint Surg Am 2013;16;95:e152. [Google Scholar]
- 8.Rossi R, Rosso F, Cottino U, Dettoni F, Bonasia DE, Bruzzone M. Total knee arthroplasty in the valgus knee. Int Orthop 2014;38:273-83. [Google Scholar]
- 9.Ueyama H, Minoda Y, Sugama R, Ohta Y, Yamamura K, Nakamura S, et al. Two-dimensional measurement misidentifies alignment outliers in total knee arthroplasty: A comparison of two-and three-dimensional measurements. Knee Surg Sports Traumatol Arthrosc 2019;27:1497-503. [Google Scholar]
- 10.Yamamura K, Minoda Y, Mizokawa S, Ohta Y, Sugama R, Nakamura S, et al. Novel alignment measurement technique for total knee arthroplasty using patient specific instrumentation. Arch Orthop Trauma Surg 2017;137:401-7. [Google Scholar]
- 11.Kaneko T, Kono N, Mochizuki Y, Hada M, Sunakawa T, Ikegami H, et al. The influence of compressive forces across the patellofemoral joint on patient-reported outcome after bi-cruciate stabilized total knee arthroplasty. Bone Joint J 2018;100-B:1585-91. [Google Scholar]
- 12.Kaneko T, Kono N, Mochizuki Y, Hada M, Toyoda S, Musha Y. Bi-cruciate substituting total knee arthroplasty improved medio-lateral instability in mid-flexion range. J Orthop 2017;14:201-6. [Google Scholar]
- 13.Scuderi GR, Bourne RB, Noble PC, Benjamin JB, Lonner JH, Scott WM. The new knee society knee scoring system. Clin Orthop Relat Res 2012;470:3-19. [Google Scholar]
- 14.Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988;15:1833-40. [Google Scholar]
- 15.Behrend H, Giesinger K, Giesinger JM, Kuster MS. The “forgotten joint” as the ultimate goal in joint arthroplasty: Validation of a new patient- reported outcome measure. J Arthroplasty 2012;27:430-6.e1. [Google Scholar]
- 16.“AYUMIEYE,” Waseda Elderly Health Association Co., Ltd. Available: https://ayumieye.com [Last accessed on 30 Apr 30]. [Google Scholar]
- 17.Kavanagh JJ, Menz HB. Accelerometry: A technique for quantifying movement patterns during walking. Gait Posture 2008;28:11-5. [Google Scholar]
- 18.Osaka H, Shinkoda K, Watanabe S, Fujita D, Kobara K, Yoshimura Y, et al. Association between trunk acceleration during walking and clinically assessed balance in patients with stroke. NeuroRehabilitation 2017;41:783-90. [Google Scholar]
- 19.Ito T, Ota Y. Comparison of gait analysis between a triaxial accelerometer-based device and an optical motion capture system. Preprints 2020;2020120336. [Google Scholar]
- 20.Battenber AK, Netravali NA, Lonner JH. A novel handheld robotic-assisted system for unicompartmental knee arthroplasty: Surgical technique and early survivorship. J Robot Surg 2020;14:55-60. [Google Scholar]
- 21.Mergenthaler G, Batailler C, Lording T, Servien E, Lustig S. Is robotic-assisted unicompartmental knee arthroplasty a safe procedure? A case control study. Knee Surg Sports Traumatol Arthrosc 2021;29:931-8. [Google Scholar]
- 22.Bollars P, Boeckxstaens A, Mievis J, Kalaai S, Schotanus MG, Janssen D. Preliminary experience with an image-free handheld robot for total knee arthroplasty: 77 cases compared with a matched control group. Eur J Orthop Surg Traumatol 2020;30:723-9. [Google Scholar]
- 23.Oussedik S, Abdel MP, Victor J, Pagnano MW, Haddad FS. Alignment in total knee arthroplasty. Bone Joint J 2020;102-B:276-9. [Google Scholar]
- 24.Fang DM, Ritter MA, Davis KE. Coronal alignment in total knee arthroplasty: Just how important is it? J Athroplasty 2009;24 (6 Suppl):39-43. [Google Scholar]
- 25.Howell SM, Shelton TJ, Gill M, Hull ML. A cruciate-retaining implant can treat both knees of most windswept deformities when performed with calipered kinematically aligned TKA. Knee Surg Sports Traumatol Arthrosc 2021;29:437-45. [Google Scholar]
- 26.Canetti R, Betailler C, Bankhead C, Neyret P, Servien E, Lustig S. Faster return to sport after robotic-assisted lateral unicompartmental knee arthroplasty: A comparative study. Arch Orthop Trauma Surg 2018;138:1765-71. [Google Scholar]
- 27.Marchand KB, Moody R, Scholl LY, Stoker MB, Taylor KB, Mont MA, et al. Results of robotic-assisted versus manual total knee arthroplasty at 2-year follow-up. J Knee Surg 2023;36:159-66. [Google Scholar]