
Excision of scaphoid and triquetrum, limited carpal fusion with articular branch neurectomy, gives adequate pain relief and improvement in wrist function.
Dr. Sanket Tanpure, Department of Orthopedics, Dr. Vithalrao Vikhe Patil Medical College, Ahmednagar, Maharashtra, India. E-mail: sankettanpure55@gmail.com
Introduction: Scapho-capitate syndrome is a rare variety, usually occur during high-energy trauma leads to fracture of scaphoid and capitate with 180 rotation of proximal fragment of capitate.
Case Report: We present a unique case of chronic neglected scapho-capitate syndrome, in which the rotated proximal fragment of capitate along with the early degenerative changes in capitate and lunate.
Results: Exploration of the wrist by dorsal approach, fracture fragment was resorbed and non-amenable for fixation. The scaphoid and triquetrum were excised. The cartilage between the lunate and capitate was denuded and arthrodesis was performed by 2.5 mm headless compression screw. The articular branch of the posterior interosseous nerve (PIN) was excised for pain relief.
Conclusion: Accurate diagnosis in acute injury is essential for functional outcome. In chronic cases, magnetic resonance imaging is necessary to know the status of cartilage for planning of surgery. Limited carpal fusion with neurectomy of articular branch of PIN can give adequate pain relief and improvement in wrist function.
Keywords: Scapho-capitate syndrome, scaphoid, capitate, Fenton syndrome, carpal fracture
A trans-scaphoid fracture-dislocation is a high-velocity orthopedic trauma in younger subjects [1]. A scaphoid and capitate fracture with 900 or 1800 proximal fragment rotation of capitate is known as scapho-capitate fracture. Fenton in 1956 first described this syndrome. There are various techniques for surgical management of scapholunate advanced collapse and scaphoid non-union advanced collapse described in the literature [2]. Depending on the involvement of the carpus and cartilage loss in the capitate head, either four-corner arthrodesis, total wrist fusion, or capito-lunate arthrodesis with and without scaphoid and triquetrum excision are the surgical options that have been discussed. The goal of partial wrist arthrodesis is to reduce pain with preservation of grip strength and functional mobility. In this study, a 28-year-old man fell on an out-stretched hand during a high-velocity bike accident causing a right scapho-capitate fracture syndrome. He presented to us after 3 months. Surgical management with 6-month follow-up is presented.
A 28-year-old male, right hand dominant IT student, had a fall on an outstretched right hand in a bike accident. He presented to us at 3 months with dorso-central wrist pain and grossly restricted and painful wrist flexion and extension. He was unable to bear weight on the right wrist and pain score as per visual analog scale (VAS) was 6/10. He had no extension and 100 flexion with 300 pronosupination (Fig. 1).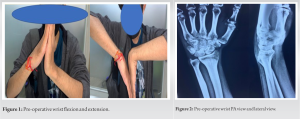 The grip rip strength of the right hand was 2 kg and the left hand was 30 kg with a Jamal Dynamometer. Radiographs and magnetic resonance imaging (MRI) demonstrated a capitate head fracture with 1800 rotation of the proximal fragment with the articular surface of the capitate facing distally toward the distal fracture fragment (Figs. 2 and 3). There was no other carpal bone injury. Early degenerative changes were noted in the capitate and lunate. Treatment options like attempting re-positioning of the rotated fractured proximal part of the capitate or capito-lunate arthrodesis with scaphoid and triquetrum excision were discussed. On dorsal exploration of the wrist, the fragment was undistinguished, found resorbed, and non-amenable for fixation. The scaphoid and triquetrum were excised. The cartilage between the lunate and capitate was denuded (Fig. 4) and arthrodesis was performed by headless compression screw (Fig. 5).
The grip rip strength of the right hand was 2 kg and the left hand was 30 kg with a Jamal Dynamometer. Radiographs and magnetic resonance imaging (MRI) demonstrated a capitate head fracture with 1800 rotation of the proximal fragment with the articular surface of the capitate facing distally toward the distal fracture fragment (Figs. 2 and 3). There was no other carpal bone injury. Early degenerative changes were noted in the capitate and lunate. Treatment options like attempting re-positioning of the rotated fractured proximal part of the capitate or capito-lunate arthrodesis with scaphoid and triquetrum excision were discussed. On dorsal exploration of the wrist, the fragment was undistinguished, found resorbed, and non-amenable for fixation. The scaphoid and triquetrum were excised. The cartilage between the lunate and capitate was denuded (Fig. 4) and arthrodesis was performed by headless compression screw (Fig. 5). 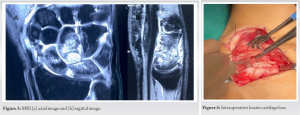
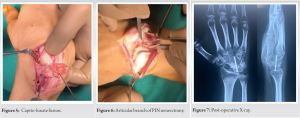 The articular branch of the posterior interosseous nerve (PIN) was excised for pain relief (Fig. 6). The capsular flap and extensor retinaculum were closed in layers. A short arm cock-up slab was given for 4 weeks. After 4 weeks, range of movement was encouraged with intermittent splinting for a total of 12 weeks. The VAS score for pain at 6 months was 2/10 which was due to capito-lunate fusion and articular branch of PIN neurectomy (Fig. 7). Extension was improved to 100 and flexion up to 200 which was 00 and 100, respectively, preoperatively with same pronosupination as pre-operative status (Fig. 8). Grip strength improved from 2 kg to 12 kg.
The articular branch of the posterior interosseous nerve (PIN) was excised for pain relief (Fig. 6). The capsular flap and extensor retinaculum were closed in layers. A short arm cock-up slab was given for 4 weeks. After 4 weeks, range of movement was encouraged with intermittent splinting for a total of 12 weeks. The VAS score for pain at 6 months was 2/10 which was due to capito-lunate fusion and articular branch of PIN neurectomy (Fig. 7). Extension was improved to 100 and flexion up to 200 which was 00 and 100, respectively, preoperatively with same pronosupination as pre-operative status (Fig. 8). Grip strength improved from 2 kg to 12 kg.
Scapho-capitate is a rare form of a carpal injury in which the scaphoid and capitate are fractured. There are cases reported in the literature with studies only in acute fractures. In such injuries, median nerve palsy with isolated sensory deficits was seen and that usually resolved after reduction [3]. Due to rarity, poor X-rays, and lack of clinical suspicion, many cases may have been undiagnosed at initial presentation [4, 5]. Delayed presentation is reported in 25% cases [6]. For this reason, we advocate the reading of wrist X-rays properly and the use of computed tomography (CT) scans to help in diagnosing a carpal injury. Delay in treatment leads to perilunate dislocation which is even more difficult to treat ultimately causing non-union, arthritis, and collapse [5]. Both the blood supply and function of the capitate and scaphoid must be restored through anatomic reduction and secure fixation. To reveal the fractures, we employed the dorsal technique. Because it offers sufficient exposure and the majority of capitate blood supply comes from palmar vessels, so this technique is advised [7]. According to Stein and Siegel [8], excessive wrist dorsiflexion causes direct compression and fracture at the neck of the capitate as it bumps up against the dorsal border of the distal radius; if this motion is continued, the proximal capitate rotates in two steps. According to Vance et al., impaction of the distal radius into the capitate from either extreme palmar flexion or dorsiflexion of the wrist joint could result in the distinctive fracture pattern and subsequent rotation [9]. Open reduction produced better results than non-operative treatment, according to Milliez et al. [10] who reviewed the literature on scapho-capitate syndrome. Each group had one instance of avascular necrosis. The most effective methods for treating midcarpal arthritis are capito-lunate and four-corner arthrodesis. Due to the additional bone surfaces that must be decorticated and the difficulty of repositioning the lunate, completing fusion of all four bone surfaces is the primary challenge of four-corner arthrodesis [11]. Facet between the hamate and lunate, which makes it difficult to reconstruct the lunate and capitate axes after capito-lunate arthrodesis due to which triquetrum excision is advantageous [11]. One major complication of capito-lunate arthrodesis is its high non-union rate. High failure rate reported in capito-lunate fusion was likely due to inadequate fixation [12, 13]. According to recent studies, screws positioned parallel to the capito-lunate joint’s loading axis apply compression at the fusion site. This has led to a fusion rate that is comparable to or even higher than that of four-corner arthrodesis [11, 14]. et al. [14] reported that the triquetrum prevents fusion by pressing against the lunate during wrist movements, which results in a lower rate of fusion in capito-lunate arthrodesis without triquetrum excision (66% in the Kirschenbaum et al. study [12] compared to 50% in the Krakauer et al. [13] study where excision was done). According to Dargai et al. [15], removal of the scaphoid and triquetrum increases the space available for radial and ulnar deviation, assisting in the improvement of extension in radial deviation and flexion in ulnar deviation.
Accurate diagnosis in acute carpal injuries is essential for good functional outcome. Assessment of wrist X-rays taken in proper position can give reliable information about the disease. In chronic or delayed presentation, requirement of better imaging like CT scan/MRI is necessary to plan surgery. Limited carpal fusion with neurectomy of articular branch of PIN can give adequate pain relief and improvement in wrist function.
Assessment of wrist pain, accurate clinical, and radiological diagnosis with proper surgical planning is considered to be the gold standard in chronic or delayed carpal injuries for better functional outcome.
References
- 1.Aslani H, Bazavar MR, Sadighi A, Tabrizi A, Elmi A. Trans-scaphoid perilunate fracture dislocation; A technical note. Bull Emerg Trauma 2016;4:110-2. [Google Scholar]
- 2.Watson HK, Ryu J. Evolution of arthritis of the wrist. Clin Orthop Relat Surg 1986;202:57-67. [Google Scholar]
- 3.Kim YS, Lee HM, Kim JP. The scaphocapitate fracture syndrome: A case report and literature analysis. Eur J Orthop Surg Traumatol 2013;23 Suppl 2:S207-12. [Google Scholar]
- 4.Kumar A, Thomas AP. Scapho-capitate fracture syndrome. A case report. Acta Orthop Belg 2001;67:185-9. [Google Scholar]
- 5.Schliemann B, Langer M, Kosters C, Raschke MJ, Ochman S. Successful delayed surgical treatment of a scaphocapitate fracture. Arch Orthop Trauma Surg 2011;131:1555-9. [Google Scholar]
- 6.Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J. Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-79. [Google Scholar]
- 7.Grend RV, Dell PC, Glowczewskie F, Leslie B, Ruby LK. Intraosseous blood supply of the capitate and its correlation with aseptic necrosis. J Hand Surg 1984;9:677-80. [Google Scholar]
- 8.Stein F, Siegel MW. Naviculo-capitate fracture syndrome. A case report: New thoughts on the mechanism of injury. J Bone Joint Surg Am 1969;51:391-5. [Google Scholar]
- 9.Vance RM, Gelberman RH, Evans EF. Scaphocapitate fractures. Patterns of dislocation, mechanisms of injury, and preliminary results of treatment. J Bone Joint Surg Am 1980;62:271-6. [Google Scholar]
- 10.Milliez PY, Dallaserra M, Thomine JM. An unusual variety of scapho-capitate syndrome. J Hand Surg Br 1993;18:53-7. [Google Scholar]
- 11.Gaston RG, Greenberg JA, Baltera RM, Mih A, Hastings H. Clinical outcomes of scaphoid and triquetral excision with capitolunate arthrodesis versus scaphoid excision and four-corner arthrodesis. J Hand Surg Am 2009;34:1407-12. [Google Scholar]
- 12.Kirschenbaum D, Schneider LH, Kirkpatrick WH, Adams DC, Cody RP. Scaphoid excision and capitolunate arthrodesis for radioscaphoid arthritis. J Hand Surg Am 1993;18:780-5. [Google Scholar]
- 13.Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg Am 1994;19:751-9. [Google Scholar]
- 14.Calandruccio JH, Gelberman RH, Duncan SF, Goldfarb CA, Pae R, Gramig W. Capitolunate arthrodesis with scaphoid and triquetrum excision. J Hand Surg Am 2000;25:824-32. [Google Scholar]
- 15.Dargai F, Hoel G, Safieddine M, Payet E, Leonard R, Jaffarbanjee Z, et al. Ten-year radiological and clinical outcomes of capitolunate arthrodesis with scaphoid and triquetrum excision for advanced degenerative arthritis in the wrist: Single-center, retrospective case series with 10 patients. Hand Surg Rehab 2019;39:41-7. [Google Scholar]





