
Management of an uncommon synovial neoplasm in an unlikely anatomic location.
Dr. Nirvin Paul, Department of Trauma Surgery, AIIMS, Rishikesh – 249 203, Uttarakhand, India. E-mail: drnirvinpaul@gmail.com
Introduction: Many loose bodies are present in the joint due to the uncommon benign neoplastic disorder known as synovial chondromatosis, which causes the production of intra-articular nodular cartilaginous lesions from the synovium. Synovial chondromatosis of the ankle joint is an uncommon condition. Here, we present a case of synovial chondromatosis of the ankle joint treated by surgical excision.
Case Report: A 42-year-old woman who had been experiencing discomfort and edema in her left ankle for 8 years and had gotten worse during the previous 2 years visited our outpatient department. Clinical and radiological examination revealed synovial chondromatosis of the left ankle joint.
Conclusion: Synovial chondromatosis of the ankle is an uncommon synovial neoplasm in an unlikely anatomic location. The diagnosis should be considered when evaluating monoarticular synovitis.
Keywords: Synovial chondromatosis, ankle joint, metaplasia, loose bodies.
Many loose bodies are present in the joint due to the uncommon benign neoplastic disorder known as synovial chondromatosis, which causes the production of intra-articular nodular cartilaginous lesions from the synovium [1]. The etiology of this condition remains poorly understood. Histologically, the synovial cells undergo a metaplastic transformation into chondrocytes [2]. Most frequently occurring in men in their third to fourth decades of life is synovial chondromatosis. Smaller joints are less frequently impacted, with big joints like the knee and hip being more frequently affected [3]. Clinically, the patient usually presents with pain, swelling, and reduced range of motion of the affected joint. The loose bodies may be palpable and crepitus may be elicited by the astute clinician. Ankle joint synovial chondromatosis is a rather uncommon condition.
A 42-year-old woman who had been experiencing discomfort and edema in her left ankle for 8 years and had gotten worse during the previous 2 years visited our outpatient department. Swelling in the region of her left ankle was initially painless; with insidious and gradually progressive pain, swelling, and stiffness. She gave the history of excision biopsy performed over the same joint done 7 years earlier. Her histopathological reports of the same were unavailable. Her symptoms recurred 2 years ago and had been gradually progressive since then. For the past 2 months, the swelling was associated with severe pain while walking and weight bearing as to limit her mobility. She had no history of loss of weight or appetite. No history of fever or trauma to the ankle joint. There was no history of swelling or similar symptoms of any other joint in her body. Her general examination revealed nothing of note. Local examination of her left ankle revealed a bony hard swelling anterior and posterior to the lateral malleolus (Fig. 1). 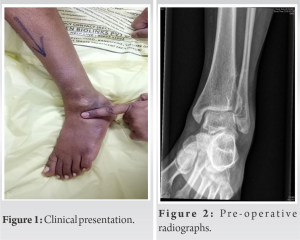 She had no distal neurovascular deficits. On a simple roentgenogram of her ankle, the joint space was intact and there were massive, calcified masses of intraarticular loose bodies anterior and posterior to her ankle (Fig. 2 and 3). There were no articular erosions or osteopenia. An anterolateral approach was used to access the tibiotalar joint. White cartilaginous masses were found in the joint distending the ankle joint anteriorly and posteriorly (Fig. 4).
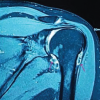
She had no distal neurovascular deficits. On a simple roentgenogram of her ankle, the joint space was intact and there were massive, calcified masses of intraarticular loose bodies anterior and posterior to her ankle (Fig. 2 and 3). There were no articular erosions or osteopenia. An anterolateral approach was used to access the tibiotalar joint. White cartilaginous masses were found in the joint distending the ankle joint anteriorly and posteriorly (Fig. 4). 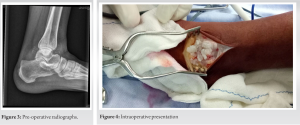 The fibular cortex was found to be intact. The masses were excised piecemeal. Her immediate post-operative period was uneventful. She was afebrile in the ward and had no local wound-related complications and she was ambulated without difficulty. She had good relief of symptoms thereafter. Histopathology reports revealed synovial tissue with attenuation of the lining. The subintima showed nodules of benign hyaline cartilage with clustering of chondrocytes displaying nuclear enlargement, hyperchromasia, and many with bi-nucleation. Few cartilaginous nodules displayed ossification with no evidence of malignant transformation.
The fibular cortex was found to be intact. The masses were excised piecemeal. Her immediate post-operative period was uneventful. She was afebrile in the ward and had no local wound-related complications and she was ambulated without difficulty. She had good relief of symptoms thereafter. Histopathology reports revealed synovial tissue with attenuation of the lining. The subintima showed nodules of benign hyaline cartilage with clustering of chondrocytes displaying nuclear enlargement, hyperchromasia, and many with bi-nucleation. Few cartilaginous nodules displayed ossification with no evidence of malignant transformation.
The production of intra-articular nodular cartilaginous lesions from the synovium is a sign of synovial chondromatosis, a benign neoplastic disorder [4]. The typical pattern of joint involvement is monoarticular, with the large joints of the body affected commonly. The literature only has a very small number of examples with synovial chondromatosis of the foot and ankle [5,6]. It is unclear what causes synovial chondromatosis exactly. The three stages of the disease’s natural history were identified by Milgram and Addison [7]. In the first stage, metaplastic changes occur in the synovium to form cartilaginous nodules. The nodules become loose bodies and detach from the synovium in stage two. The third stage is characterized by the tendency of many loose entities in the joint cavity to consolidate and calcify [8]. Synovial chondromatosis patients typically exhibit symptoms such as discomfort, swelling, locking, stiffness of the joint, and/or a well-palpable lump. Recently, there has been some interest in the malignant potential of synovial chondromatosis. Davis et al. observed that the risk for malignant degeneration was 5% [9]. Diagnosis of synovial chondromatosis is made by imaging; calcifications are seen in standard radiographs in a majority of cases. Intra-operative findings of multiple rounded osseocartilaginous loose intra-articular bodies are of diagnostic significance [10]. In the early stages of the disease process, radiographs show increased soft tissue density. In such situations, magnetic resonance imaging is useful [3]. Removal of the intra-articular loose bodies is the mainstay of treatment for synovial chondromatosis. In initial phases of active synovitis, synovectomy is usually performed. In Stage 3 of the condition, synovitis is usually not present and synovectomy is not required. Recurrence is reported in 3–23% conditions [8,11,12]. Recurrence is thought to be associated with incomplete synovectomy with retention of a portion of the activated synovium.
Synovial chondromatosis of the ankle is an uncommon synovial neoplasm in an unlikely anatomic location. The etiology is unknown and it involves synovial metaplasia to form cartilaginous nodules that tend to coalesce. Recurrence is commonly associated with inadequate resection.
We highlight the importance of considering synovial chondromatosis in the differential diagnosis when evaluating monoarticular synovitis even in unlikely locations.
References
- 1.Hocking R, Negrine J. Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-7. [Google Scholar | PubMed]
- 2.Buess E, Friedrich B. Synovial chondromatosis of the glenohumeral joint: A rare condition. Arch Orthop Trauma Surg 2001;121:109-11. [Google Scholar | PubMed]
- 3.Blandino A, Salvi L, Chirico G, Longo M, Faranda C, Romeo P, et al. Synovial osteochondromatosis of the ankle: MR findings. Clin Imaging 1992;16:34-6. [Google Scholar | PubMed]
- 4.Kistler W. Synovial chondromatosis of the knee joint: A rarity during childhood. Eur J Pediatr Surg 1991;1:237-9. [Google Scholar | PubMed]
- 5.Young-In Lee F, Hornicek FJ, Dick HM, Mankin HJ. Synovial chondromatosis of the foot. Clin Orthop Relat Res 2004;423:186-90. [Google Scholar | PubMed]
- 6.Galat DD, Ackerman DB, Spoon D, Turner NS, Shives TC. Synovial chondromatosis of the foot and ankle. Foot Ankle Int 2008;29:312-7. [Google Scholar | PubMed]
- 7.Milgram JW, Addison RG. Synovial osteochondromatosis of the knee. Chondromatous recurrence with possible chondrosarcomatous degeneration. J Bone Joint Surg Am 1976;58:264-6. [Google Scholar | PubMed]
- 8.Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801. [Google Scholar | PubMed]
- 9.Davis RI, Hamilton A, Biggart JD. Primary synovial chondromatosis: A clinicopathologic review and assessment of malignant potential. Hum Pathol 1998;29:683-8. [Google Scholar | PubMed]
- 10.Wong K, Sallomi D, Janzen DL, Munk PL, O’Connell JX, Lee MJ. Monoarticular synovial lesions: Radiologic pictorial essay with pathologic illustration. Clin Radiol 1999;54:273-84. [Google Scholar | PubMed]
- 11.Shpitzer T, Ganel A, Engelberg S. Surgery for synovial chondromatosis. 26 cases followed up for 6 years. Acta Orthop Scand 1990;61:567-9. [Google Scholar | PubMed]
- 12.Maurice H, Crone M, Watt I. Synovial chondromatosis. J Bone Joint Surg Br 1988;70:807-11. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Understanding Synovial Chondromatosis: A Rare Cause of Shoulder Impingement
April 1, 2026 Understanding Synovial Chondromatosis: A Rare Cause of Shoulder Impingement March 1, 2026 Double Whammy: Rare in-Tandem Impalement Injuries to Ipsilateral Knee and Ankle in a Rural Farmer – A Case Report
March 1, 2026 Double Whammy: Rare in-Tandem Impalement Injuries to Ipsilateral Knee and Ankle in a Rural Farmer – A Case Report January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report
January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge
October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge