
Synovial chondromatosis of the shoulder is a rare condition that requires a high index of suspicion in atypical shoulder pain, as early recognition and surgical removal of loose bodies are essential for optimal outcomes.
Dr. Ashish Kumar, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: ashishrikesh1609@gmail.com
Abstract
Introduction: Synovial chondromatosis (SCM) is a benign neoplastic condition manifesting as multiple loose bodies within a joint cavity, usually affecting the knee and hip joints. It is a rare cause of shoulder joint pain. There is a challenge in diagnosing this condition, as early findings reveal non-ossified, radiolucent, cartilaginous loose bodies, which significantly delay the diagnosis. Surgical excision and synovectomy are the usual treatments. Here, we present an unusual case of SCM of the shoulder joint that was successfully treated with arthroscopic excision, with good functional outcome at the 12-month follow-up.
Case Report: A 30-year-old male presented with complaints of left shoulder pain for 6 months, with a history of unknown origin. Pain was insidious in onset, characterized by a dull aching pain of mild-to-moderate intensity that worsened with throwing activities over the past 2–3 months. There were symptoms of locking and crepitus affecting daily activities. The physical examination revealed diffuse tenderness, and the range of motion was full with no obvious deformity. The clinical tests for impingement were positive, and the testing of rotator cuff integrity suggested no tear. Plain radiography was grossly normal except for some calcification seen medially. Magnetic resonance imaging demonstrated multiple loose bodies involving the subscapular recess, posterior and inferior aspect of the glenohumeral joint, and at the rotator interval, suggestive of SCM. The patient was surgically treated with arthroscopic excision, and multiple nodules were excised.
Conclusion: There were no symptoms of recurrence at the 12-month follow-up.
Keywords: Shoulder pain, synovial chondromatosis, arthroscopic removal of loose bodies.
Synovial chondromatosis (SCM) is a rare and non-malignant condition involving the joint capsule lined with synovium, the tendon sheath, and the bursa [1]. Most commonly, it affects the large synovial joints, including the knees and hips [2]. In the shoulder joint, it is particularly rare and usually occurs in the subacromial space, the sheath of the biceps tendon, and the joint cavity [3,4,5]. Patients typically present with a history of dull aching pain and may have a limited range of motion and crepitus [6]. The exact etiology is often unknown. Still, reports have been suggestive of metaplastic change in the synovial membrane and further transformation into cartilage-producing cells, which eventually break down and remain as loose bodies inside the joint capsule. These loose bodies can then calcify and ossify, leading to osteochondromatosis [7]. Secondary cause can be linked to trauma or underlying joint pathology such as osteoarthritis or rheumatoid arthritis [8,9]. Diagnosis remains challenging due to its gradual onset. It is usually confirmed by radiographic imaging. Initial X-ray findings may not show abnormalities, as in 20% of cases, it takes time for calcification to develop. Magnetic resonance imaging (MRI) can easily detect joint effusion, synovial hypertrophy, and loose bodies [8]. Furthermore, to confirm the diagnosis, histopathological examination of the obtained tissue samples is recommended [10]. Symptomatic management can be done conservatively in the acute stages of the disease. Once the diagnosis is established and loose bodies are detected, surgical intervention is necessary. Surgery typically includes either open arthrotomy or arthroscopy to remove the loose bodies and the affected synovium [11]. Recently, arthroscopic removal of loose bodies, along with synovectomy, has become the choice over open arthrotomy [12].
A 30-year-old right-hand-dominant male presented with complaints of left shoulder pain for 6 months and aggravated for 2 months, with a history of unknown origin. Pain was insidious in onset, characterized by a dull, aching sensation of mild-to-moderate intensity that aggravated with throwing activities. There were persistent symptoms of snapping and crepitus affecting daily activities. Physical examination revealed diffuse tenderness over the left shoulder joint, and the range of motion was full with no obvious deformity. Clinical tests for shoulder impingement were positive, and the testing of rotator cuff integrity suggested no tear.
Investigations
Plain radiography was grossly normal except for some medial calcification. MRI demonstrated multiple loose bodies involving the subscapular recess, posterior and inferior aspect of the glenohumeral joint, and at the rotator interval, suggestive of SCM (Fig. 1).
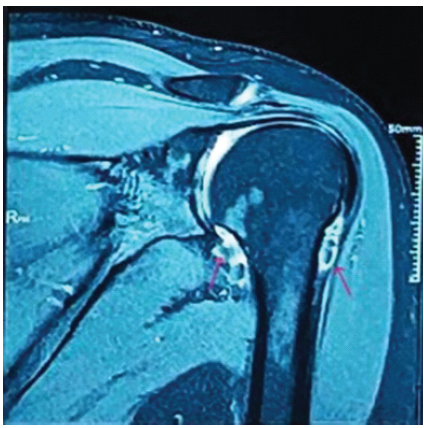
Figure 1: Pre-operative magnetic resonance imaging (MRI) of left shoulder joint: T2-weighted fat-saturated coronal MRI revealed multiple loose bodies that appeared as numerous focal filling defects, suspended within the hyperintense joint effusion.
Treatment
The patient was surgically treated with arthroscopic excision. The standard arthroscopy was performed under general anesthesia with the patient in the right lateral position, the left upper limb maintained in abduction, and traction applied. Standard posterior and anterior portals were made. Diagnostically, articular cartilage, joint space, and labrum appeared to be normal. Active intra-synovial tissue proliferation was present, and multiple pedunculated intra-articular loose bodies were revealed in the axillary pouch (Fig. 2).
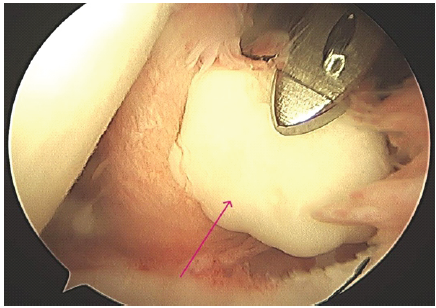
Figure 2: Arthroscopic view from the standard portal: Showing a pearly white cartilaginous loose body (arrow marked). The inflamed and hypertrophic synovium is clearly visible. The articular cartilage of the humeral head appears intact in this field of view.
A synovectomy was performed using a motorized shaver. By interchanging the portals, the loose bodies were removed with a large grasper. Approximately 25 fragments, ranging from 2 mm to 18 mm in size, were removed (Fig. 3). Two of them were large, each measuring 18 mm; for such extensive fragments, straight artery forceps were used and were removed in a piecemeal fashion. After the removal of loose bodies, radiofrequency cauterization was done.

Figure 3: Excised loose bodies: Numerous loose bodies after arthroscopic removal.
Outcome and follow-up
Postoperatively, an immediate X-ray was ordered, and a shoulder sling was provided. The patient underwent supervised physiotherapy treatment. Immediate passive range of motion exercises were encouraged, and active movement and strengthening exercises were initiated after 1 week.
At the latest follow-up, 12 months later, the patient reported a good functional outcome of the shoulder.
SCM is a benign condition characterized by the formation of multiple loose bone or cartilage fragments within the joint’s synovial lining, which can potentially cause pain and limited mobility. It usually involves the larger joints, and the shoulder joint is rarely affected. The prevalence of SCM in the shoulder has been reported as 5% of all SCM cases [13]. The etiology is not well understood, although histological reports suggest that it involves metaplastic proliferation of synovial tissue. The most common site for loose body formation has been noted as where synovium transforms into cartilage [14]. The disease usually progresses through three stages in primary SCM as described by Milgram. In stage one, the chondromas are attached to the synovium. In stage two, a breach in the synovium occurs, and the chondromas are released as loose bodies into the joint capsule. In the final stage, synovial proliferation becomes inactive, but intra-articular loose bodies remain in the joint capsule [15]. The diagnosis remains challenging, as symptoms are often vague and inconsistent with physical examination findings. The symptoms frequently overlap with those of other shoulder disorders, as in many cases, there is no history of locking and instability, which are the significant characteristics of intra-articular loose bodies. Sometimes, diagnosis is delayed when an X-ray appears normal in the case of a pre-calcified stage [2]. An MRI proved to be an effective imaging modality in cases where no calcification had occurred. MRI furthermore facilitates the localization of chondroma at various sites, including the biceps tendon sheath, sub-acromial bursa, and acromioclavicular joint [16]. We presented this rare case of SCM involving the shoulder joint. In our case, the patient presented with pain and a persistent snapping sensation during shoulder movement. Physical examination revealed tenderness and crepitus with full shoulder movement ranges in all planes. The patient underwent an MRI, which showed multiple intra-articular loose bodies. Surgical excision combined with a partial or complete synovectomy is the recognized procedure for the treatment. Arthroscopic excision is favored due to fewer complications and faster recovery. In our case, the patient was surgically treated with arthroscopic excision, and multiple nodules were removed. Approximately 25 such fragments were removed, with a maximum size of 18 mm. Technical difficulties were experienced during the removal of free pieces from the portals due to the large size of the loose bodies. Straight artery forceps were used for such large fragments and were removed in a piecemeal fashion. Postoperatively, a shoulder sling was provided, and the patient underwent supervised physical therapy management, including exercises to improve shoulder range of motion. At the 12-month follow-up, the patient was symptom-free and reported a good functional outcome of the left shoulder joint. In the most recent case series by Guo et al., involving 15 cases of shoulder SCM, the authors found that arthroscopic debridement is a reliable treatment option for shoulder SCM, offering the advantages of minimal invasiveness, rapid recovery, and low complication rates [17]. Although SCM is generally considered a benign condition, malignant transformation into synovial chondrosarcoma has been reported in rare cases. The estimated risk of malignant transformation ranges from 1% to 10%, and warning signs include rapid progression of symptoms, early recurrence after surgical treatment, and invasion into surrounding soft tissues. The recurrence rate of SCM has been reported to range between 15% and 25%, particularly in cases where loose bodies or diseased synovium are incompletely removed [18]. However, in our case, there was no evidence of recurrence at the 12-month follow-up, and the patient showed complete recovery without any evidence of malignant progression. Recent literature also supports arthroscopic management as an effective treatment option with low recurrence rates when complete removal of loose bodies and synovectomy are performed [19,20,21]. Although the patient in our study showed excellent post-operative improvement, a significant limitation is that the follow-up period was short (12 months), and the results may deteriorate over time due to irreversible degenerative changes. Furthermore, an extended follow-up period is necessary to monitor for relapse.
This case elaborated on the diagnosis and management of SCM in a patient who presented with shoulder pain. We believe that clinicians should consider a broad differential diagnosis for such a condition when imaging findings are normal and symptoms persist. Once the diagnosis is confirmed, arthroscopic surgical excision is effective in treatment with fewer post-operative complications and early functional recovery. Patients should be followed up regularly, with consideration given to the risk of recurrence.
Shoulder pain may occasionally result from rare conditions; clinicians should maintain a high index of suspicion for unusual causes in persistent cases. Diagnosis can be challenging and often delayed due to non-specific radiological findings. In patients who do not respond to initial management, repeat imaging should be considered to reassess the underlying pathology. Regular and frequent follow-up is essential, as ongoing clinical evaluation can help detect subtle changes and facilitate timely and accurate diagnosis.
References
- 1. Yucel B, Mutlu S, Komur B, Mutlu H. Arthroscopic removal of giant loose bodies in the glenohumeral joint. Int J Surg Case Rep 2014;5:459-61. [Google Scholar] [PubMed]
- 2. Murphey MD, Vidal JA, Fanburg-Smith JC, Gajewski DA. Imaging of synovial chondromatosis with radiologic-pathologic correlation. Radiographics 2007;27:1465-88. [Google Scholar] [PubMed]
- 3. Horii M, Tamai M, Kido K, Kusuzaki K, Kubo T, Hirasawa Y. Two cases of synovial chondromatosis of the subacromial bursa. J Shoulder Elbow Surg 2001;10:186-9. [Google Scholar] [PubMed]
- 4. Lunn JV, Castellanos-Rosas J, Walch G. Arthroscopic synovectomy, removal of loose bodies and selective biceps tenodesis for synovial chondromatosis of the shoulder. J Bone Joint Surg Br 2007;89:1329-35. [Google Scholar] [PubMed]
- 5. Maier D, Izadpanah K, Jaeger M, Ogon P, Südkamp NP. Biceps tenoscopy in arthroscopic treatment of primary synovial chondromatosis of the shoulder. Arthrosc Tech 2014;3:e539-45. [Google Scholar] [PubMed]
- 6. Liu B, Kim SH, Jang YH, Rhee SM, Yoo JC, Kim SC, et al. Synovial osteochondromatosis: Clinical characteristics unique to the shoulder. Clin Orthop Surg 2023;15:118-26. [Google Scholar] [PubMed]
- 7. Adelani MA, Wupperman RM, Holt GE. Benign synovial disorders. J Am Acad Orthop Surg 2008;16:268-75. [Google Scholar] [PubMed]
- 8. Wahab H, Hasan O, Habib A, Baloch N. Arthroscopic removal of loose bodies in synovial chondromatosis of shoulder joint, unusual location of rare disease: A case report and literature review. Ann Med Surg (Lond) 2018;37:25-9. [Google Scholar] [PubMed]
- 9. Ranalletta M, Bongiovanni S, Calvo JM, Gallucci G, Maignon G. Arthroscopic treatment of synovial chondromatosis of the shoulder: Report of three patients. J Shoulder Elbow Surg 2009;18:e4-8. [Google Scholar] [PubMed]
- 10. Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801. [Google Scholar] [PubMed]
- 11. Memon F, Pawar ED, Gupta D, Yadav AK. Diagnosis and arthroscopic treatment of synovial chondromatosis of glenohumeral joint: A case report. J Orthop Case Rep 2021;11:59-62. [Google Scholar] [PubMed]
- 12. Fowble VA, Levy HJ. Arthroscopic treatment for synovial chondromatosis of the shoulder. Arthroscopy 2003;19:E2. [Google Scholar] [PubMed]
- 13. Poyser E, Morris R, Mehta H. Primary synovial osteochondromatosis of the shoulder: A rare cause of shoulder pain. BMJ Case Rep 2018;11:e227281. [Google Scholar] [PubMed]
- 14. Tokis AV, Andrikoula SI, Chouliaras VT, Vasiliadis HS, Georgoulis AD. Diagnosis and arthroscopic treatment of primary synovial chondromatosis of the shoulder. Arthroscopy 2007;23:1023.e1-5. [Google Scholar] [PubMed]
- 15. Milgram JW. The classification of loose bodies in human joints. Clin Orthop Relat Res 1977;124:282-91. [Google Scholar] [PubMed]
- 16. Walker EA, Murphey MD, Fetsch JF. Imaging characteristics of tenosynovial and bursal chondromatosis. Skeletal Radiol 2011;40:317-25. [Google Scholar] [PubMed]
- 17. Guo B, Yang YF, Li T, Wang D, Xiong Y, Li J, et al. Clinical outcomes of arthroscopic treatment for shoulder synovial chondromatosis: A case series. J Shoulder Elbow Surg 2025;34:e1215-23. [Google Scholar] [PubMed]
- 18. Deng X, Liu S, Liu H. Synovial chondromatosis: Novel advances in understanding the pathogenesis and in diagnostic strategies (Review). Mol Med Rep 2026;33:33. [Google Scholar] [PubMed]
- 19. Park JP, Marwan Y, Alfayez SM, Burman ML, Martineau PA. Arthroscopic management of synovial chondromatosis of the shoulder: A systematic review of literature. Shoulder Elbow 2022;14 1 Suppl:5-15. [Google Scholar] [PubMed]
- 20. Vij N, Tran TL, Kelly BD, Dane CT, Menzer HM, Vaughn JM. Shoulder synovial chondromatosis in an adolescent athlete: A case report. J Orthop Case Rep 2022;12:101-4. [Google Scholar] [PubMed]
- 21. Banerjee S, Kumar Soni B, Prakash V, Meer F, Elhence A. Shoulder synovial chondromatosis managed arthroscopically in a young adult: A case report. Cureus 2025;17:e100445. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report
June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report
January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge
October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge October 1, 2025 A Rare Visitor at the Ankle: Synovial Chondromatosis of the Lateral Malleolus
October 1, 2025 A Rare Visitor at the Ankle: Synovial Chondromatosis of the Lateral Malleolus